
Remember me
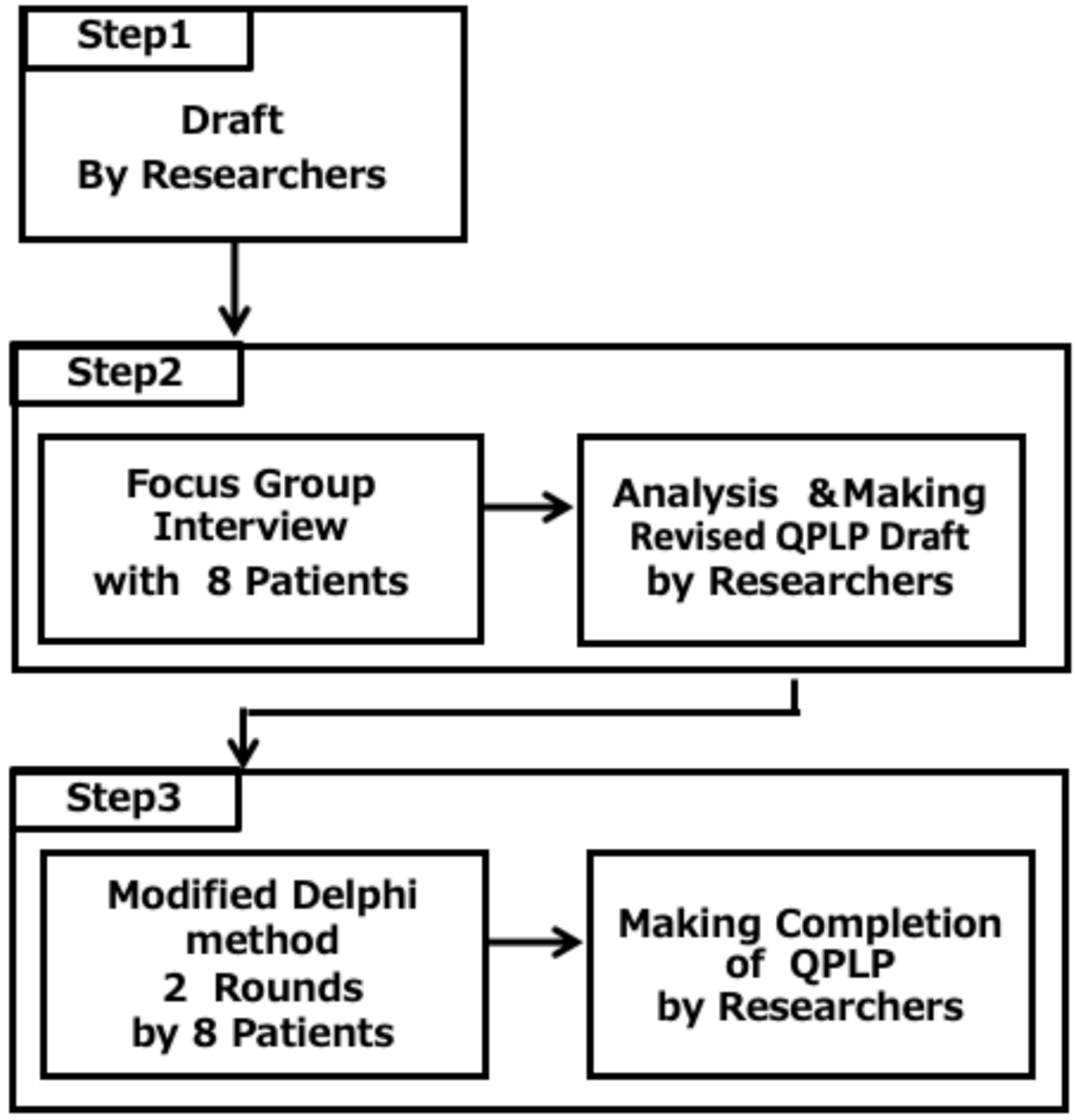


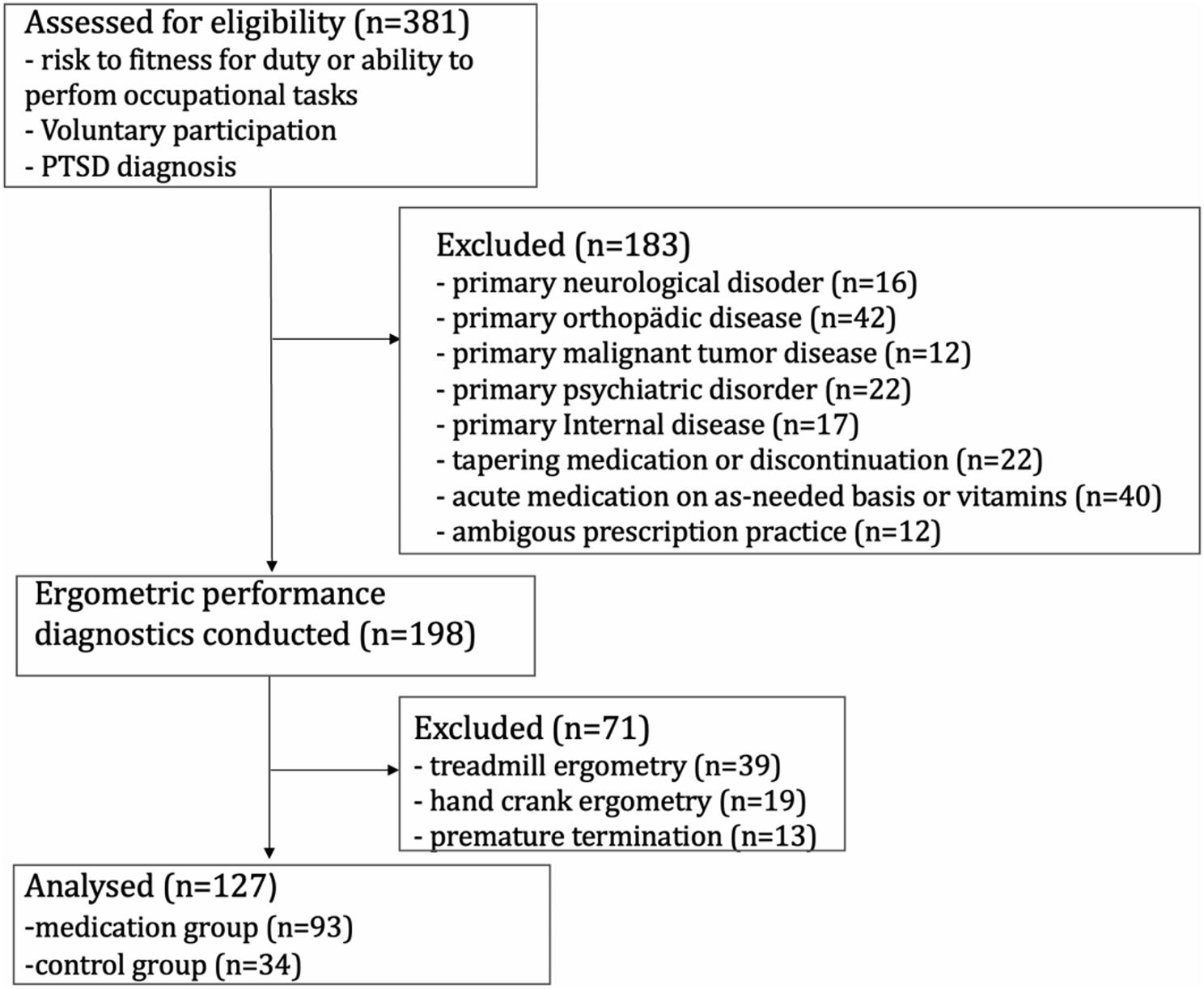

The QPLP was developed in three steps (Fig. 1). In the first step, we created a first draft. In the second step, FGIs were conducted with eight patients, and the QPLP was revised. In the third step, the QPLP was finalized through two rounds of evaluation using the modified Delphi method. The ethics committee of Keio University Faculty of Pharmacy (231124-1) approved the study protocol.
Fig. 1
Flowchart of the development of the QPLP conducted in three steps
Step 1: Preparation of the initial QPLP draftWe drafted the initial QPLP. The authors were six healthcare pharmacy researchers with pharmacist qualifications and two patient researchers with lived experience as patients (in contrast to pharmacist qualifications). The healthcare pharmacy researchers (MH, YY, KS, SI, SH) independently extracted questions from 119 existing QPLs [27, 38], and after discussion, the list was narrowed down to 57 questions. Through iterative discussion among the researchers, overlapping or ambiguous items were merged or excluded, thereby refining the list to 57 questions.
Two existing QPLs were used to help rephrase statements as questions to a pharmacist. One of these QPLs was the Question Builder, which was provided by Healthdirect Australia and established in August 2006 under an agreement with the Australian Council of Governments [31]. It was selected because it is still widely used and researched. The other was “For Patients and Families Preparing for Important Consultations,” which is used by cancer patients in Japan [27]. The existing QPL [33,34,35] used by pharmacists was not referenced because it did not include questions about anything other than medications. The patient researchers (NS, YK) participated in discussions to finalize the first draft of the QPLP. Since previous studies suggested limiting the number of questions to fewer than 20 [38] and keeping the length of the list to one page to reduce patient burden, the number of questions was further reduced to fewer than 20, and the initial draft consisted of 17 questions.
The questions were listed in order of ease of use, and were intended to be used at home or during the time they waited at the pharmacy on patients’ second or subsequent visits to the pharmacy. The aim was to promote person-centered communication by encouraging patients to ask pharmacists relevant questions and communicate their concerns, wishes, thoughts, and daily life situations, thereby enhancing communication with the pharmacists.
Step 2: Focus group interviews and revision of the draft QPLPThe FGIs were conducted using the method of Vaughn et al. [37]. Advantages of this method include group discussions that generate stimuli about the topic and the emergence of extensive cohesive data.
RecruitmentParticipants were recruited using patient organization mail lists and social media platforms. The inclusion criteria were as follows:
1)aged 18 or older
2)regularly visits pharmacies and has used prescription medications for more than three years
3)has experience in patient organization activities and sharing personal experiences with other patients
The third criterion was included to encourage participation by those whose experience in patient groups or other organizations allowed them to speak from a broader perspective, one that includes not only their personal experience but also the opinions of other patients.
Implementation of FGIsEight applicants responded within two weeks. They were divided into two groups of three and five members, which is a comfortable number for group discussions. The consent form was emailed in advance, explained, and collected on the day of the interviews. Separate schedules were established for each group. To ensure that participants met the criteria and did not all have the same health condition, participant background information was collected using questionnaires. The FGIs were designed to gather the opinions of participants regarding the initial QPLP draft, focusing on the prioritization of questions, as well as suggestions for additional questions not included in the draft. We used a self-developed interview guide (Supplement 1). The facilitator, experienced in FGIs and qualitative research, ensured that the participants could freely express their views.
Each FGI lasted for 1 h 45 min. The participants were three men and five women, with a median age (min, max) of 51 (30,73) years. These participants used a median of 3 [2, 11] medicines and visited their doctors approximately once a month. The participants had regularly used pharmacies for an average of 18.4 years (Table 1). Their conditions spanned a range of different areas: neurological, respiratory, cardiovascular, diabetic, gastrointestinal, psychiatric, otolaryngological, oncological, ophthalmological, and gynecological (Table 1).
Table 1 Participant characteristics in the focus group interview and modified Delphi methods (N = 8)The questions were revised and adjusted through the FGIs, resulting in a revised draft of 16 questions.
Analysis of FGI data and preparation of the revised QPLPAudio data from the FGIs were transcribed verbatim, using anonymized personally identifiable information that was then used for analysis. From the data, opinions were extracted for each QPLP question. These comments were reviewed and discussed by all researchers. The adoption or rejection of each question as well as its wording were revised. For questions related to “treatment,” we were mindful not to exceed the scope of the pharmacist’s role by inappropriately acting as a medical practitioner.
Step 3: Evaluation and finalization of the QPLP using the modified Delphi methodThe modified Delphi method [37] was employed to both evaluate the QPLP and collect patient opinions. The method is a structured consensus-building technique that collects expert opinions through multiple rounds with controlled feedback. It allows anonymous participation, reduces bias from dominant individuals or groups, and enhances the convergence of opinions in fewer rounds by incorporating feedback and discussion among experts.
Implementation of the modified Delphi methodWe conducted two rounds of evaluations and collected additional opinions using the modified Delphi method. Both rounds were conducted via email with the same participants from the FGIs using self-developed questionnaires (Supplements 2, 3). In Round 1, the participants rated if each of the 16 questions should be included in the QPLP using a five-point scale (Strongly Agree, Agree, Neutral, Disagree, Strongly Disagree) and provided reasons for their ratings. The feedback from Round 1 was aggregated, and all data were shared with the participants without modification. Three questions proposed in the first round were added, and 19 questions were evaluated in the second round. In the second round, participants re-evaluated the questions using the same five-point rating scale. To avoid bias, communication related to the modified Delphi method was managed by individuals not involved in the survey or analysis, with the researchers receiving only anonymized data.
Analysis of the data from the modified Delphi method and preparation of the final QPLPThe researchers confirmed that opinions had been aggregated through the two-round Delphi method and discussed the aggregated Round 2 data, providing their opinions on each question. As the QPLP is intended only as an example list to facilitate patients in asking questions, it was considered important to ensure that it caused no harm. Therefore, consensus was defined such that any item that even one participant rated as “disagree” or “strongly disagree” was deleted. This approach reflects the consensus-building process of the Delphi method while prioritizing patient safety and acceptability.
For the remaining questions, the text was adjusted based on the opinions of the researchers.
Comments (0)