
Remember me


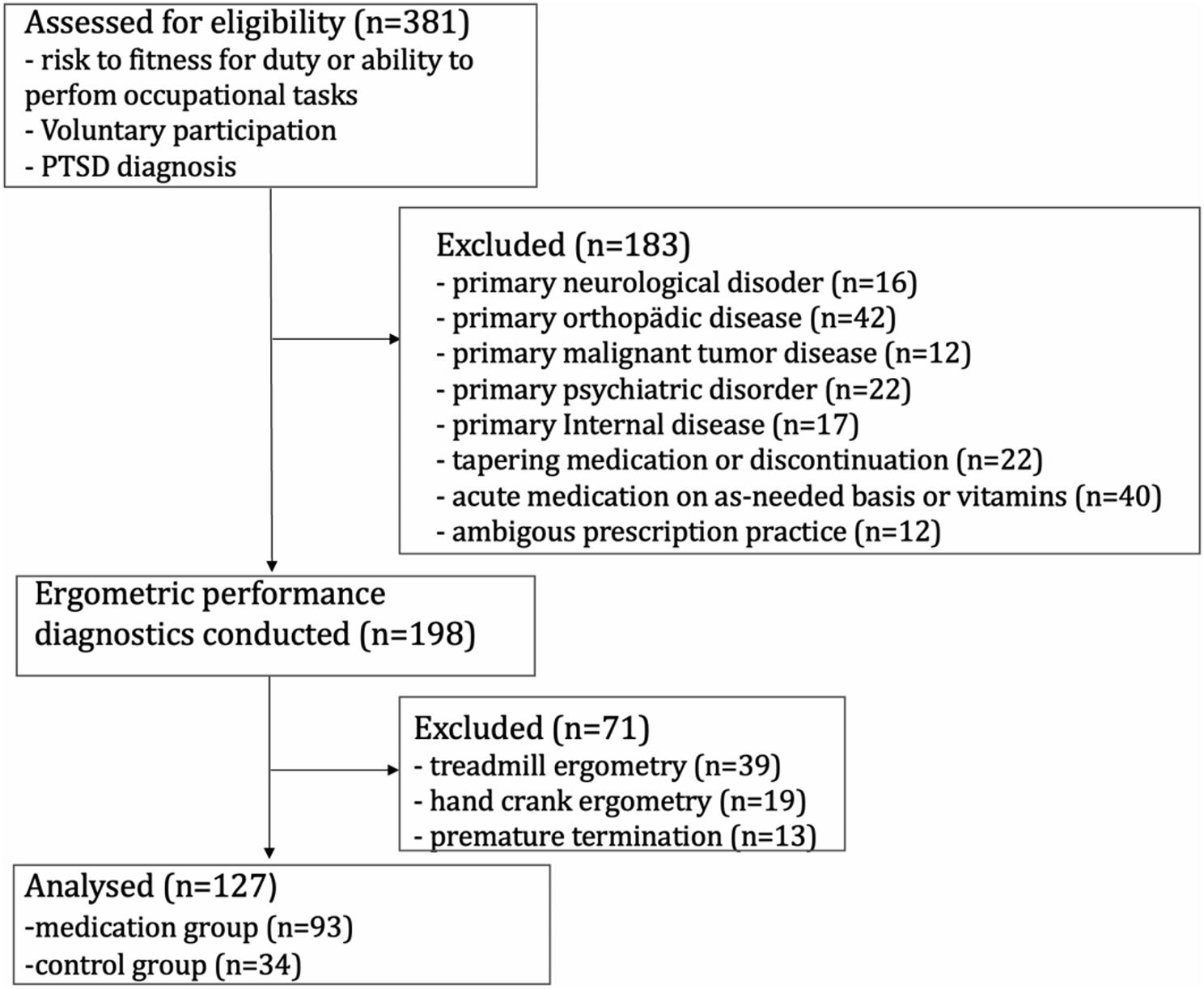

Out of the initial pool of 381 patients, 127 (males: 121 (95.3%)/females: 6 (4.7%)) met the specified inclusion criteria. A total of 93 (73.2%) patients were taking medication, whereas the control group consisted of 34 (26.8%) patients. A comprehensive medication regimen was noted for 42 patients (33.1%). The specific demographic characteristics of this cohort and corresponding comparisons are presented in Table 1.
Table 1 Characteristics of patients enrolled (n = 127)Upon comparing the demographic data across the entire population, no significant differences were detected in any parameter.
Long-term medication and drug-drug interactionsA total number of 283 drugs were identified to be taken on a long-term basis, with an average of 3.0 (± 2.0) drugs per patient. Additionally, 122 potential DDIs were detected. The distribution of drugs per patient is shown in Fig. 2.
Fig. 2
Distribution of the number of long-term medication (LTM) (N = 283) across the entire cohort (N = 93)
All medication groups were compared to a control group, which consisted of 26.8% of all included patients, that did not take any LTM. While primary diagnosed with PTSD, these patients exhibited comorbidities that were predominantly from orthopedic or surgical origin, such as chronic or functional back pain, lumbar and cervical spine syndromes, compartment syndrome, impingement syndrome of the shoulder, and postoperative complaints (52.9%). Additional comorbidities were of internal-orthopedic origin (18.6%) or purely internal origin, such as arterial hypertension, type 2 diabetes mellitus, hyperlipidemia, hyperuricemia, or obesity (14.4%). Moreover, psychiatric-internal complaints were observed, including attention-deficit disorders, recurrent depressive episodes, and concurrent obesity, lipid metabolism disorders, or metabolic syndrome (14.1%).
To facilitate systematic comparison and analysis of drug use patterns, the drugs were categorized based on their therapeutic and chemical properties according to the Anatomical Therapeutic Chemical (ATC) Classification. The total number of drugs was assigned to eight different main ATC groups as well as four therapeutic subgroups, as presented in Fig. 3.
Fig. 3
Allocation of all prescribed LTM categorized according to their anatomical main group (a) and the therapeutic subgroups for ATC N (b). The number of patients whose medication included one, two, three or more drugs within each anatomical main group is depicted in (a). The prescribed LTMs were assigned to eight ATC main groups, targeting the following organ systems: A = Alimentary Tract and Metabolism, B = Blood and Blood Forming Organs, C = Cardiovascular System, G = Genitourinary System and Sex Hormones, H = Systemic Hormones (excluding Sex Hormones and Insulin), M = Musculoskeletal System, N = Nervous System, R = Respiratory Tract (a). A detailed depiction of the subdivision of ATC N into the therapeutic subgroups N02 (Analgesics), N03 (Antiepileptics), N05 (Antipsychotics), and N06 (Psychoanaleptics) is shown in (b) as the number of patients whose medication included one or two drugs within each therapeutic subgroup
Among all patients, 72 (77.4%) patients received medication consisting of at least two long-term drugs, while the medication of 66 (71.0%) patients included drugs assigned to ATC N. The last resulted into 113 potential DDIs. Out of these interactions, 76 (65.0%) were classified as potentially moderate and 41 (35.0%) as potentially severe. 16 patients (24.2%) were at intermediate risk of experiencing an interaction due to their medication, 18 patients (27.3%) of the drug combinations posed low risk, 13 (19.7%) patients were identified with both DDI from intermediate and low risk, while 19 (28.8%) patients did not experience any DDI. On average, each patient experienced 1.7 (± 1.3) drug interactions. Figure 3 illustrates the potential effects of DDIs and their frequency of occurrence observed.
Performance in relation to LTMATC N – drugs that target the nervous systemData analysis revealed that 80 out 93 patients (86.0%) took at least one drug that was systematically assigned to ATC N, which target the central nervous system. Comparing all main ATC groups identified in this cohort with each other, drugs assigned to ATC N made up the largest share in terms quantity. The group of patients taking ATC N medications included 63.0% of all enrolled patients, who consumed an average of 3.1 ± 2.1 long-term medications (LTM). Overall, 17.6% of the patients took one LTM, 36.4% took two LTMs, and 44.0% took three or more LTMs. Comorbidities were primarily of a purely orthopedic or surgical nature (43.8%), orthopedic-internal origin (26.3%), or orthopedic-neurological origin (3.8%), such as neck pain and back pain occurring alongside migraines. Additional comorbidities included psychiatric-orthopedic conditions (5.0%) and psychiatric-internal conditions (21.1%).
For the therapeutic subgroups it is N06 which made up the largest share and is the subgroup that hosts the drugs explicitly approved for PTSD treatment in Germany. In total, 22 patients (27.5%) received one drug approved for PTSD in Germany and 50 patients (62.5%) received a selective monoamine reuptake inhibitor, which was either a selective serotonin reuptake inhibitor (SSRI), a serotonin norepinephrine reuptake inhibitor (SNRI) or a selective serotonin norepinephrine reuptake inhibitor (SSNRI), which exhibit antidepressive properties.
Overall, patients who consumed three or more drugs obtained significantly poorer p-max. than control (N = 42, 217 (200–250) W vs. N = 34, 250 (225–267) W, P = 0.021). Maximum performance regime was inversely correlated with inclining numbers of drugs belonging to ATC N in each medication regime leading to a complex medication containing two or more ATC N drugs among others (Table 2). Moreover, it was found that patients receiving medication that contained two or more drugs, whereby at least two drugs classified as ATC N exhibited a significantly poorer maximum performance than control (N = 39, 208 (221–255) W vs. N = 34, 250 (225–267) W, P = 0.024), while patients taking an equivalent number of drugs with only one drug classified as ATC N did not differ from controls. P-4-mmol Lac. was not significantly different in any of these cases. The number of drugs belonging to ATC N in each medication regime were inversely correlated with maximum performance, albeit weakly (Table 2).
Table 2 Spearman correlation of p-max. And p-4-mmol Lac. With ATC main group N, presence of serotonin monoamine reuptake inhibitors And potential occurrence of QT interval prolongationDrugs provoking QTc- interval prolongationOf all patients with medication, 8 (10%) took drugs that did not include drugs exhibiting QT interval prolongation as a potential adverse side effect, while 36 (44.4%) took one, 26 (32.5%) took two and 10 (12.5%) took three medications known to prolong QT interval. A total of 15.0% of all included patients were assigned to the group of patients experiencing at least one DDI resulting from their overall medication that has potential to prolong QT interval. Patients in this group took an average of 3.3 ± 1.8 medications per person, with 52.6% taking at least two medications and 47.4% taking three or more medications. Patients in this subgroup predominantly suffered from orthopedic and surgical comorbidities (52.6%), including functional musculoskeletal complaints, lumbar spine syndrome, and postoperative complaints following fractures. Additionally, orthopedic-psychiatric complaints (18.4%) were observed, such as lower back pain along with depressive episodes or trauma-related disorders sleep disturbances. Further comorbidities included orthopedic-internal medical conditions (29.0%), which for example involved musculoskeletal pain alongside arterial hypertension, hypo- and hyperthyroidism, hyperlipidemia, and obesity.
As indicated in Figs. 4 and 47.5% of all potential DDIs involving at least one ATC N drug were identified as potential cause of QT interval prolongation. Statistical analysis revealed that patients exclusively exposed to at least one DDI that potentially prolongs the QT interval exhibited significantly reduced maximum performance compared to control (N = 19, 208 (175–258) W vs. vs. N = 34, 250 (225–267) W p = 0.021). The maximum performance correlated negatively with the occurrence of QT interval prolonging drugs in a complex medication regime (Table 2). Drugs that have been determined to have interactions that increase the risk of developing QT interval prolongation was included in the appendix ( Table 3).
Fig. 4
Emerging effects due to potential DDI and the frequency of their occurrence. Data are presented as percentage (%)
Table 3 List of drugs that have been determined to have interactions that increase the risk of developing QT interval prolongationPatients who experienced different DDI at the same time did not exhibit a decline in performance compared to the control group. There were no significant differences in p-4mmol Lac. levels in any of the groups in terms of maximum performance on bicycle ergometry, however it correlated negatively with the occurrence of potential QT interval prolonging drugs in a complex medication regime (Table 2), although we did not observe any abnormal cardiac changes by ECG.
Selective monoamine reuptake inhibitorsA total of 35.5% of all included patients were assigned to the SMRI group. These patients took an average of 3.1 ± 2.0 medications per person, with 45.5% taking two medications and 54.5% taking three or more medications. Patients in this subgroup predominantly suffered from orthopedic and surgical comorbidities (32.7%), such as functional back pain, various forms of osteoarthritis, knee joint pain, postoperative complaints following upper or lower leg fractures, or polytrauma. Additionally, orthopedic complaints were present along with internal medical conditions, such as hyperlipidemia, arterial hypertension, or obesity (28.8%). Further comorbidities included purely internal medical conditions (15.4%) as well as psychiatric and orthopedic complaints (23.1%), such as depressive episodes with low back pain or panic disorders with functional back pain.
In cases where the patient’s medication contained at least two drugs with one being SSRI, SNRI or SSNRI, the patients achieved significantly lower maximum performance compared to controls (p-max. N = 44, 208 (200–250) W vs. N = 34, 250 (225–267) W, P = 0.004) with a trend towards significance for p-4-mmol Lac. (N = 44, 158 (129–174) W vs. N = 34, 171 (148–191) W, P = 0.052). For all other cases characterized by the absence of a selective monoamine reuptake inhibitor (SMRI) but the presence of one other ATC N category drug, no significant differences compared to control were identified. Both maximum performance and performance at 4 mmol/l lactate threshold in capillary blood correlated negatively with the presence of selective monoamine reuptake inhibitors in the course of no medication, medication lacking selective monoamine reuptake inhibitors, and medication including SMRI.
Comments (0)