In this study, we demonstrated that protein binding rate of VCM is 40%, although being highly variable. These data provide a basis for reconsidering the importance of free concentration in VCM therapy. We have shown that free VCM concentration was influenced by total serum protein concentration. Therefore, free VCM concentration may be a better indicator of clinical outcome than total VCM concentration in patients with hyper- or hypoproteinemia. In Fig. 3, we compared target attainment AUC and fAUC, and no significant differences were observed. On the other hand, our study suggested it was possible that the protein binding rate of VCM was lower (40%) than as has been reported (50%) [12]. Given that Butterfield et al.. also reported a similar result to ours [10], future studies should be based on new protein binding rate (40%) instead of conservative protein binding rate (50%) for vancomycin. Despite free concentration is supposed to be better indicator than total as PK/PD indices, the Japanese guideline recommended an AUC target of 400–600 mg・h/L based on total VCM concentration presuming MIC being 1 µg/mL [5]. It is not ideal that the AUC-guided TDM is generally conducted for VCM. The fAUC-guided TDM should rather be more appropriate for VCM therapy. However, fAUC target has not been examined sufficiently. Judging from protein biding rate of 40% in our study, the target fAUC may be 240–360 mg・h/L for the future. Likewise, Leroux, et al. reported that AUC/MIC of 400 mg・h/L corresponds to fAUC/MIC of 240 mg・h/L, assuming median protein binding rate of 40% in adult [13]. In addition, fAUC is supposed to be the most appropriate PK/PD indices. Rybak has stated 24-h bacterial count of methicillin-sensitive S. aureus correlates with AUC in neutropenic mouse thigh infection model [14]. However, one should note that the correlation between AUC and antimicrobial effect was evaluated by semi-quantitative interpretation, and the target value of fAUC was not mentioned in this review. Further animal study is necessary to investigate the target fAUC of VCM.
In this study the measurement of free VCM concentration raises two important issues. The first one is high variability in protein binding rate. Furthermore, protein binding rate of VCM varied in this study. Moise-Broder also reported that the protein binding of this drug ranged from 29 to 71% [15]. Berthoin, et al. reported that there was a significant variation in protein binding rate (12–100%) [16]. These variabilities indicate that free VCM concentration cannot be predicted precisely. Therefore, although vancomycin is binding-insensitive, we should pay attention to free concentration to practice more precise TDM. The second is the influence of hypoproteinemia. We found serum total protein was a significant covariate for free VCM concentration in multivariate linear regression since VCM is predominantly bound both by albumin and immunoglobulin A [17]. However, albumin and total protein are potentially confounding, and therefore we did not select albumin as an explanatory variable in multivariate linear regression [10, 17, 18]. From these findings, we should adopt free VCM target approach, particularly in hyper- or hypo-proteinemic population.
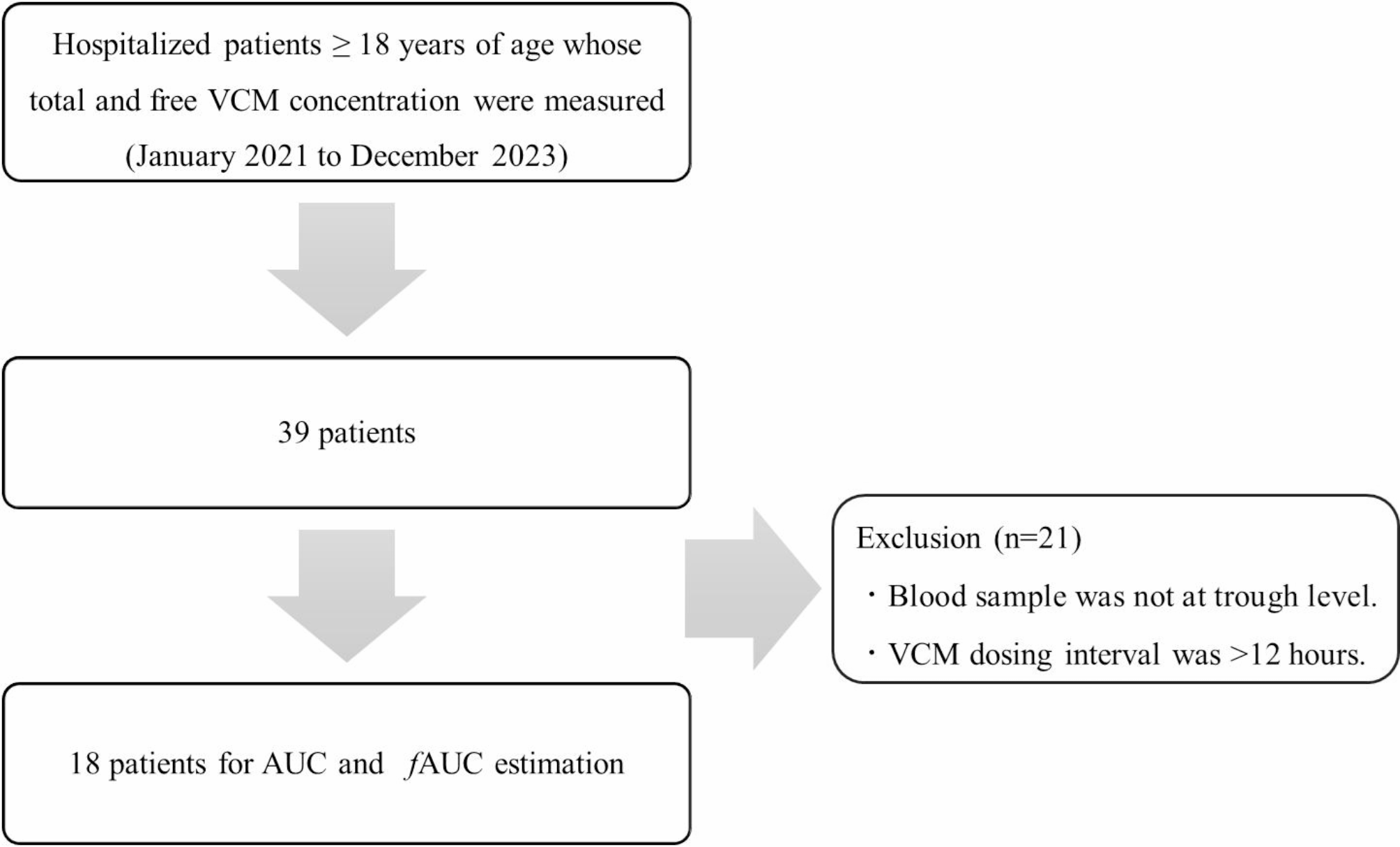
Since few studies have measured the fAUC of VCM, we calculated fAUC based on the protein binding rate and the AUC by the Bayesian method. We estimated AUC by only the trough level. Since K. Oda, et al. reported that AUC estimation solely based on the trough level produced strong bias in patients receiving VCM every 24 h [9], we targeted the patients receiving VCM every 12 h and less for AUC estimation. The Japanese guideline recommended target AUC is 400–600 mg・h/L. Given that vancomycin protein binding rate is 50%, the therapeutic range of fAUC is broadly 200–300 mg・h/L [19]. In our study, 9 patients (50.0%) had an AUC > 600 mg・h/L and 12 (66.7%) had an fAUC > 300 mg・h/L. No significant differences were observed in the probability of target attainment. Therefore, we should perform AUC-guided TDM in principle. On the other hand, the above result suggests that TDM based on fAUC may strictly reduce the VCM dosage in a selected population. Namely, the fAUC-guided TDM for VCM has the potential to reduce side effects such as acute kidney injury in hypoproteinemic population.
Our study has limitations. First, this is a single-center noninterventional enrolling limited number of patients. Second, we had not performed correlation between free vancomycin concentration as determined by high-performance liquid chromatography and by the particle-enhanced turbidimetric inhibition immunoassay. Third, we did not investigate the impact of liver disease, concomitant medications and serum immunoglobulin concentration on free vancomycin. Because this is a retrospective study, we were unable to accurately calculate the Child-Pugh Score. And the influence of drug-drug interactions on protein binding of vancomycin is complex and difficult to assess comprehensively. Because immunoglobulin is a part of total protein in serum, we used only serum total protein for free VCM estimation. Lastly, we couldn’t compare the target attainment rates of AUC and fAUC dividing into hyperproteinemia and hypoproteinemia groups because of small sample size, so further research is needed.




Comments (0)