
Remember me


This section provides detailed descriptions of the findings across 11 health facilities in three regions of Tanzania (Dar es Salaam, Dodoma, and Kigoma) between 13th and 30th November 2022, focusing on the coverage and fidelity of implementation of Adolescent- and Youth-Friendly SRH services.
Adolescent and youth friendly services delivery pointsFindings in Table 2 indicate that the facilities sampled included three dispensaries (27%) from Dodoma City Council (DCC), Kasuku Town Council (KTC), and Kigoma Municipal Council (KMC). Moreover, 55%(n = 6) of the facilities were health centers, three from Kinondoni Municipal Council, one from Dodoma City Council, and two from Kigoma Municipal Council. The study also sampled 18% (n = 2) hospitals, one from Dodoma City Council and another from Kigoma Municipal Council. A majority (82%) were government-owned, while the remaining 18% (n = 2) were managed by Faith-Based Organizations (FBOs).
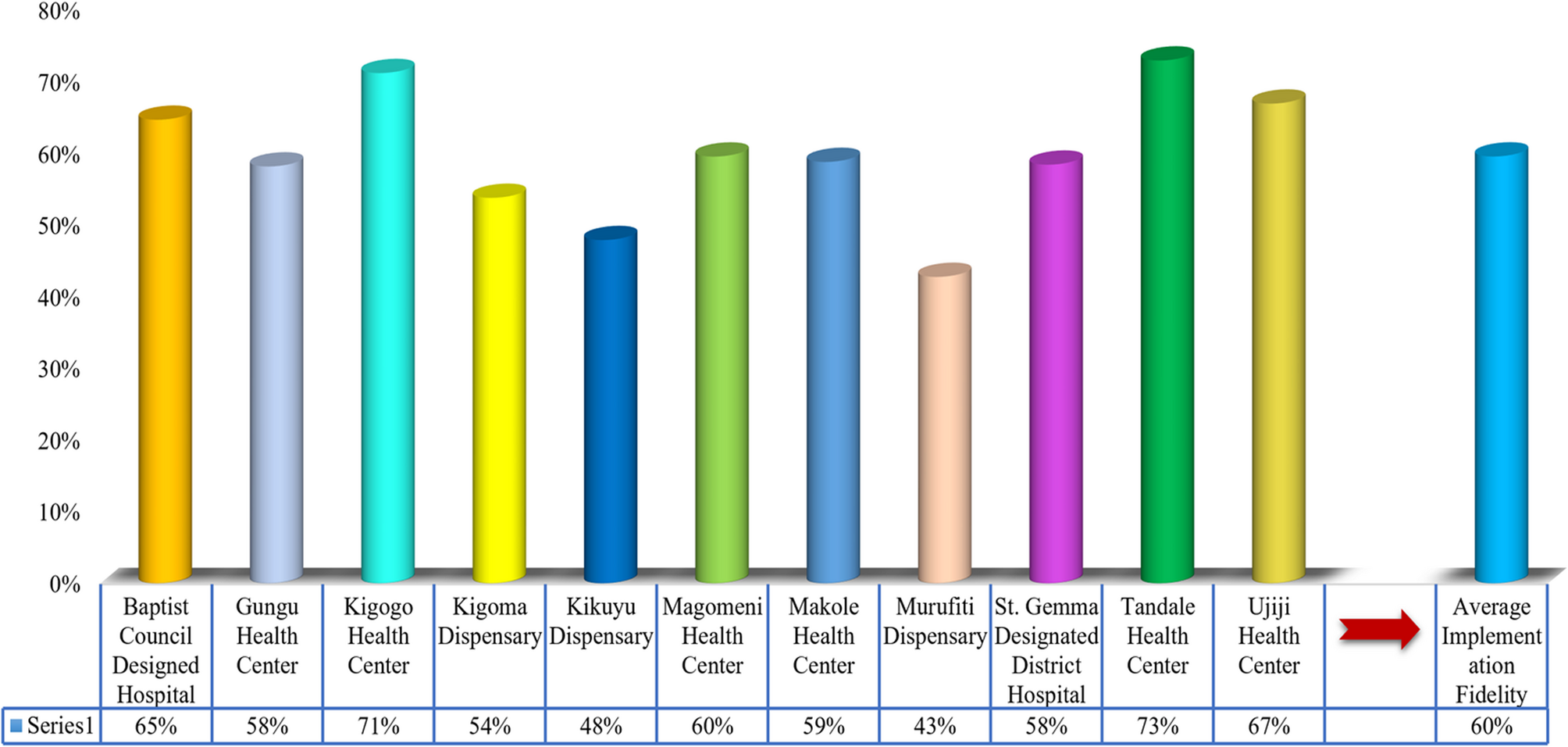
Table 2 Adolescent and youth friendly services delivery points (n = 11)Adolescent- and youth-friendly srh services coverage and implementation fidelity at health facilitiesThe findings of the study in Fig. 1 indicate that Adolescents and Youth-Friendly Sexual and Reproductive Health Services were available to all sampled delivery points (100%) in accordance with national standards by the adolescent- and youth-friendly sexual and reproductive health services guidelines in Tanzania [15, 28]. Although all facilities reported delivering adolescent- and youth-friendly SRH services, none achieved full adherence to the SRH national standards set for adolescent- and youth-friendly SRH service delivery. The average implementation fidelity of the National Standards of SRH services was 60%, which health centers achieved better than other types of health facilities. Tandale health center (73%), Kigogo health center (71%), Ujiji health center (67%), Baptist council designated hospital, and Magomeni (60%) health center had the highest coverage and fidelity implementation of the adolescent-and youth-friendly SRH national standards, while Murufiti dispensary was the lowest (43%).
Nevertheless, government-owned facilities had the highest achievement in the coverage and fidelity implementation of adolescent- and youth-friendly SRH service delivery compared to faith-based facilities. Differences in the coverage and fidelity implementation of adolescent- and youth-friendly SRH services may probably be attributed to the fact that government facilities, particularly health centers, have standardized SRH protocols, comprehensive training programs, trained staff, community and stakeholder involvement and engagement, better availability and accessibility to supplies and services, which can enhance fidelity to the standards. This indicates a significant gap between policy commitments and actual service provision practices on the ground.
Fig. 1
Adolescent- and Youth-Friendliness of the SRH Services coverage and implementation fidelity at Health Facilities (n = 11)
Proportional distribution of the SRH National standards coverage and fidelity implementation at health facilitiesThis section presents the findings that demonstrate the extent to which facilities adhered to the national standards for adolescent- and youth-friendly SRH services, with a focus on the proportional distribution of coverage and fidelity implementation. It further disaggregates performance by specific criteria under each standard, providing a detailed assessment of how comprehensively and consistently the standards are applied. The findings highlight strengths and gaps in service delivery, offering critical insights for improving quality and equity in SRH care for adolescents and youths across Tanzania. The criteria were studied as commonly practiced in the Tanzanian context to find out whether the SRH services were available, and delivered equitably, acceptably, accessibly, and effectively.
Under standard I: Adolescent health literacy, the assessment revealed that while efforts had been made to promote awareness, none of the facilities reached 100% of the coverage and fidelity implementation. Findings in Fig. 2 indicate that Tandale Health Center achieved the highest proportion at 77%, while Murufiti dispensary achieved the lowest at 54%. Particulalry weak performance was observed in the availability of adolescent-specific information, education and communication materials in waiting areas (Criterion 2 of the national standards (35%), adolescents’ basic health knowledge (Criterion 8 of the SRH national standards) (47%), and the existence of outreach programs led by trained personnel (Criterion 4 of the SRH national standards) (59%). These findings suggest that many adolescents and youth accessing these facilities may lack the information and literacy required to make informed decisions about their health, thereby limiting their ability to effectively navigate available services. The staff at these 11 health service delivery points do not have adequate health literacy to enable them to gain access to, understand, and effectively use it in ways that promote and maintain their good health.
Fig. 2
Proportional distributions of the implementation of standard I on adolescent health literacy about adolescent- and youth-friendly SRH services (n = 11)
Standard II: Parent and community support for adolescents assessed the extent to which parents, guardians, and community members were engaged in supporting adolescents’ and youths’ health needs. As shown in Fig. 3, achievements of the coverage and fidelity implementation of standard II ranged from 47% (Murufiti Dispensary) to 78% (Kikuyu Dispensary), with notable deficiencies in systematic engagement with parents, teachers, and religious leaders. Only 37% of facilities had healthcare providers who regularly informed parents and teachers during school meetings about adolescent services (criterion number 15 of the SRH national standards). Just over half (55%) of the assessed facilities had plans for community outreach activities and/or involvement of outreach workers in activities to increase caregivers’ support for adolescents’ use of services, while 59% (Criterion 12 of the SRH national standards). Nevertheless, 59% of the facilities maintained partnerships with local agencies to enhance community support. These findings imply that health services are still largely facility-centered and fail to leverage community-based support systems crucial for adolescents and access and uptake of SRH services (criterion 11).
Fig. 3
Proportional distributions of the implementation of standard II on Parent and community support for adolescents in receiving adolescent- and youth-friendly SRH services (n = 11)
In relation to standard III: Appropriate package of services, significant implementation gaps were evident. While all facilities indicated in Fig. 4 demonstrated offering some form of adolescent and youth SRH services, the comprehensiveness of those services varied widely. Tandale health center led with a 69% score, while murufiti dispensary lagged at just 27%. Critical deficits were observed in referral systems (Criterion 22 of the SRH national standards), only 4% of facilities effectively referred adolescents and youth to appropriate levels of care, and the delivery of services beyond facility-based care, such as community outreach and follow-ups. Only 51% offered a complete package of SRH services that fulfil the needs of all adolescents and youth in the facility or through referral linkages and community outreache (Criterion 23 of the SRH national standards). Just 56% had established referral procedures based on the existing policies to services within and outside the health sector, including provisions of transition care for adolescents and youth with chronic health conditions (Criterion 20 of the SRH national standards). These findings underscore the urgent need for standardization of SRH service packages and reinforcement of referral pathways to ensure continuity of care for adolescents and youths.
Fig. 4
Proportional distributions of the implementation of standard III on the appropriate adolescent- and youth-friendly SRH package for adolescents and youth (n = 11)
Standard IV: Provider competencies evaluated the preparedness and capacity of healthcare providers to offer adolescent- and youth-friendly SRH services. Findings in Fig. 5 indicate that none of the facilities achieved full compliance, with scores ranging from 44% (Murufiti dispensary) to 75% (Ujiji Health Center). Deficiencies were especially pronounced in continuing professional education for providers that includes an adolescent and youth healthcare component (Criterion 30 of the SRH national standards) (18%), the public display of adolescents’ rights and providers obligations in health facilities (Criterion 27 of the SRH national standards) (41%), and supportive supervision mechanisms in place to improve healthcare providers’ performance (Criterion 29 of the SRH national standards) (44%). These gaps reveal systemic weaknesses in maintaining provider competency and accountability, which are essential for respectful, confidential, and non-judgemental care. Notably, data elements used to evaluate whether adolescents and youth received effective services (Criterion 33 of the SRH national standards) were absent from the tools, highlighting a methodological limitation that also needs to be addressed.
Fig. 5
Proportional distributions of the implementation of standard IV on provider competences in delivering adolescent- and youth-friendly SRH services (n = 11)
The assessment of standard V: Facility characteristics highlighted concerns regarding the physical and operational environments of the health facilities. Findings in Fig. 6 show that none fully met national standards for adolescent- and youth-friendly settings. Kigogo and Tandale health centers had the highest coverage and fidelity implementation of the standard (67%), while Kikuyu Dispensary achieved the lowest (46%). Core issues included lack of essential technology, equipment, and supplies needed to ensure effective service provision to adolescents and youth (Criterion 48 of the SRH national standards, only 5% availability across facilities), insufficient privacyand confidentaliaty during consultations and provision of healthcare at all times (Criterion 47 of the SRH national standards) (48%), and poorly maintained or unwelcoming facility environment (Criterion 46 of the SRH national standards) (50%). More than half (54%) of the facilities specifically Kigogo health center, Kikuyu dispensary, Magomeni health center, Murufiti dispensary, St. Gemma designated district hospital, and Ujiji health center, lacked adequate resources to deliver adolescent- and youth-friendly SRH services effectively. These gaps reduce adolescents’ willingness to seek care and compromise service delivery outcomes.
Fig. 6
Proportional distributions of the implementation of standard V on facility characteristics in delivering adolescent- and youth-friendly SRH services (n = 11)
Standard VI: Equity and non-discrimination assessed whether adolescents and youth from diverse backgrounds could access services equitably. Again, findings in Fig. 7 demonstrate that none of the facilities scored a full 100%, with Kigogo health center achieving the highest score (94%) and Kikuyu Dispensary the lowest (25%). Several facilities lacked policy commitments to non-discrimination that are displayed prominently and take remedial actions when necessary (Criterion 52 of the SRH national standards) (35%) or formal policies and procedures ensuring universal access to SRH services regardless of age, marital status, education, ethnicity, sexual orientation or socioeconomic status (Criterion 49 of the SRH national standards) (41%). Criterion 50 of the SRH national standards for the presence and implementation of policies and procedures for services that are free at the point of use, or affordable, accounted for 52% of the facilities.
Fig. 7
Proportional distributions of the implementation of standard VI on equity and non-discrimination of adolescents and youth in friendly SRH services (n = 11)
Nevertheless, two criteria under standard VI of the SRH national standards were not scored during this assessment because the data elements to measure their achievements are not currently accommodated by the assessment and monitoring tools. These criteria are namely criterion 54: “Health-care providers and support staff demonstrate the same friendly, non-judgemental, and respectful attitude to all adolescents, regardless of age, sex, marital status, sexual orientation, cultural background, ethnic origin, disability, or any other reason”; and criterion 58: “Vulnerable group(s) of adolescents are involved in the planning, monitoring, and evaluation of health services, as well as in certain aspects of health-service provision. Moreover, at three health services delivery points (Kikuyu Dispensary, Murufiti Dispensary, and Ujiji HC); the Health-service providers did not know who the vulnerable group(s) of adolescents in their community are”. The assessment also noted that, at four health services delivery points(Kikuyu Dispensary, Makole HC, Murufiti Dispensary, and Ujiji HC); the health services delivery point does not involve vulnerable group(s) of adolescents in the planning, monitoring, and evaluation of health services, as well as in certain aspects of health-service provision.
Standard VII: Data and quality improvement evaluated whether facilities used disaggregated service data to confirm continuous improvement efforts. The results in Fig. 8 showed a clear gap in using data as a tool for quality enhancement. Kigogo health center scored the highest with 87%, while Murufiti dispensary and St. Gemma designated district hospital had the lowest scores at 49% for coverage and fidelity of SRH national implementation standards. Only 12% of facilities had reward and recognition systems for high-performing staff (Criterion 63 of the SRH national standards), while just 41% had self-monitoring mechanisms in place for the quality of adolescent- and youth SRH services (Criterion 61 of the SRH national standards). Only three(48%) facilities (Baptist, council-designated hospital, Kigogo health center, and Makole health center) had systems for recognizing and rewarding provider excellence. In contrast, St. Gemma designated district hospital had no supportive supervision framework linked to monitoring outcomes, and both Kigogo and Tandale health centers lacked systems for recognizing outstanding staff performance. These findings hinder motivation, accountability, and sustained SRH service improvement.
Fig. 8
Proportional distributions of the implementation of standard VII on data and quality improvement of adolescent- and youth-friendly SRH services (n = 11)
Lastly, Standard VIII: Adolescent participation emerged as the most underimplemented area, with no facility scoring 100% and a range from 29% at St. Gemma designated district hospital to 70% at Tandale health center, as shown in Fig. 9. Only three (7%) facilities (Gungu health center, Tandale health center, and Ujiji health center) had policies supporting adolescent and youth participation in SRH service design, implementation, monitoring, and evaluation (Criterion 72 of the SRH national standards). Adolescents and youth were not involved in planning or service delivery at five facilities (8%) (Baptist council designated hospital, Kigoma dispensary, Kikuyu dispensary, St. Gemma designated district hospital, and Ujiji health center) (Criterion 78 of the SRH national standards). Moreover, health providers and significant others are adequately prepared to support adolescents and youth engagement (Criterion 74 of the SRH national standards) in only three facilities (27%). These findings reveal that adolescents and youth are largely (36%) treated as passive recipients rather than active participants in shaping SRH services that affect their lives (Criterion 80 of the SRH national standards).
Fig. 9
Proportional distributions of the implementation of standard VIII on adolescents and youth participation in SRH services (n = 11)
Comments (0)