
Remember me
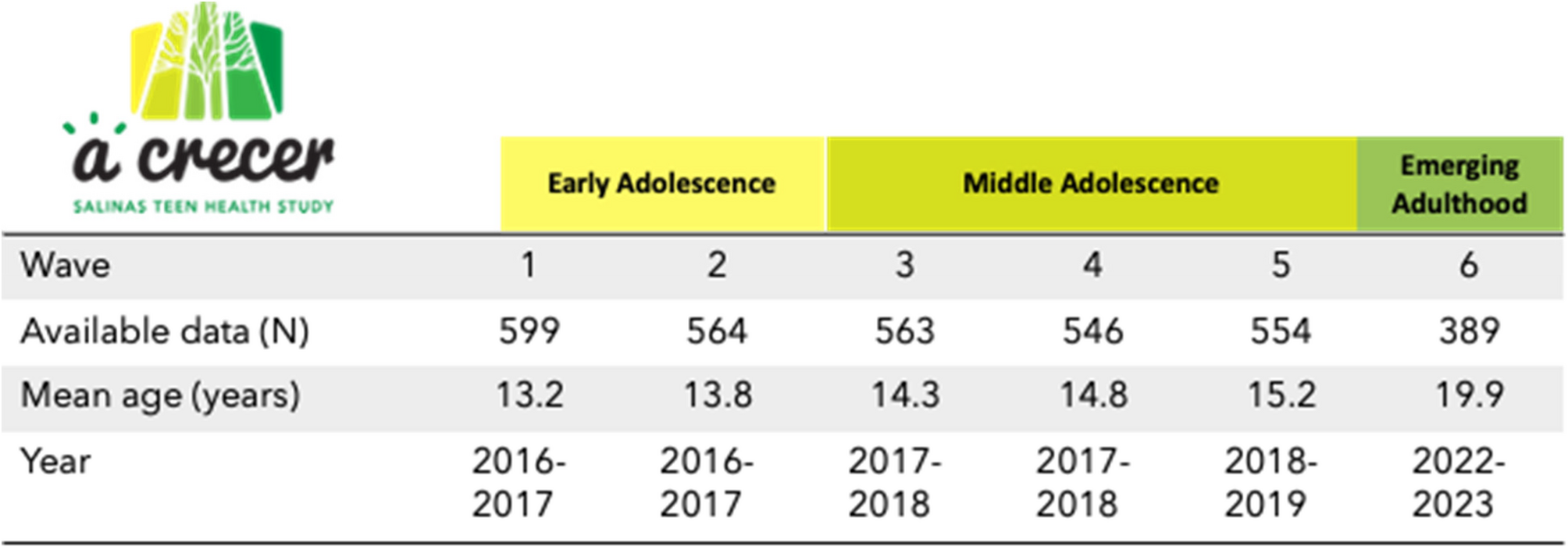


We used data from the prospective cohort study A Crecer, which aims to explore social factors influencing sexual health outcomes throughout adolescence and into emerging adulthood. The study followed a community-based participatory research (CBPR) approach and was thus developed in partnership with the Monterey County Health Department and with input from youth and community advisory boards, who informed our research questions [14]. CBPR has been demonstrated to be of particular importance when conducting research with vulnerable populations, including youth and migrants, and when conducting research on sensitive topics such as violence and SRH [13]. It follows eighth graders from four public middle schools in Salinas, California. Here we present data collected from 2015 to 2023. Participants had a total of six study visits, referred to as waves 1–6, between the ages of 13 to 20 (Fig. 1). A description of the cohort and more detail about the CBPR approach are available elsewhere [14, 15].
Fig. 1 Setting
SettingSalinas is an agricultural hub which produces much of the nation’s lettuce and other crops. While it benefits from a rich cultural diversity and strong community ties, it also faces challenges such as high poverty rates and community violence, which may negatively impact adolescent health. The area’s proximity to fresh produce and outdoor spaces provides opportunities for healthy living, but socioeconomic disparities prevent access to these opportunities and limited access to healthcare also present ongoing health concerns for youth.
ParticipantsEligible participants were aged 12 to 15 years old, able to complete the study procedures in English or Spanish, intended to live in Salinas for the next year, and were willing to provide contact information for a parent. Of the 599 participants who were enrolled in the original cohort (Wave 1–5), 389 (65%) participants re-enrolled at Wave 6 approximately 6 years after initial enrollment (wave 6 mean age: 20 years). Our analysis includes all participants who reenrolled at Wave 6 to examine TFA exposures in early and middle adolescence (Waves 1–5, ages 13–15) with health outcomes in emerging adulthood (Wave 6).
Data collectionSurveys were interviewer-administered approximately every 6-months during Waves 1–5 and again at Wave 6 using computer-based questionnaires in English and Spanish (Fig. 1). Sensitive questions were completed independently by participants using audio computer-assisted self-interviewing (ACASI) in early and middle adolescence (Waves 1–5), and CASI without audio in emerging adulthood (Wave 6). Surveys captured data on structural (e.g. community-level protective and risk factors), interpersonal (e.g. family, peer, and partner relationship factors), and individual level (e.g. substance use, relationship qualities, mental health) factors theorized to influence SRH outcomes (e.g. self-reported sexual behaviors, partner violence, and health care service access). All Wave 1–5 study visits in early and middle adolescence were conducted in-person. In emerging adulthood, Wave 6 interviews were done in person or with a study interviewer over the phone or via videoconference. To facilitate accessibility of study participation, asynchronous visits could also occur with participants completing study interviews independently on a computer or smartphone. Data collection in emerging adulthood also included biological testing for chlamydia and gonorrhea (via vaginal swab or urine) and pregnancy (via urine sample). Participants who completed their visit remotely were offered a self-sample collection kit for STIs and pregnancy, including instructions for sample collection, which they returned by prepaid mail for laboratory analysis. Participants also had the option to upload STI results if they recently tested with an external medical provider within the same month of their visit or if they planned to test with an external medical provider after their visit.
MeasuresThe outcomes that were examined at Wave 6 in emerging adulthood were related to SRH, mental health (i.e. symptoms of anxiety and symptoms of depression) and violence (IPV victimization, IPV perpetration, TFA). Symptoms of depression (yes/no) were measured using the Patient Health Questionnaire-8 (PHQ-8) for adolescents using a cutoff of ≥ 10. The measure has been validated as correlated with the diagnosis of depression in national samples and Latine populations and used in prior publications from the A Crecer study [16, 17]. Symptoms of anxiety were measured using the General Anxiety Disorder 7-item scale (GAD-7), which is widely used to screen for GAD, assessing frequency of experiences over the past 2 weeks with scores ranging from 0 to 21 (0–9 no to mild anxiety; 10–14 moderate; 15–21 severe) [18]. In-person IPV victimization (yes/no) and IPV perpetration (yes/no) were asked in relation to the past six months, and measured using a five-item version of the Revised Conflict Tactics Scale [19,20,21]. Items included experiencing from a partner (victimization) or doing any of the following to a partner (perpetration): calling them names, insulting them, or treating them disrespectfully in front of others; swearing at them; threatening with violence or to hurt them; pushing or shoving them; or throwing something at them that could hurt them. The latter two items were considered physical abuse and the remaining items, psychological abuse.
SRH outcomes included teen pregnancy, any STI diagnosis, visited a clinic for sexual health services in the last 12 months (yes/no), participant or their partner used any birth control method other than condoms to avoid pregnancy in the last 12 months (always, sometimes, never), condom use at last sex (yes/no), and use of emergency contraception in the last 12 months (yes/no). Teen pregnancy was defined as becoming pregnant or getting someone pregnant before age 20. Participants assigned female sex at birth were asked if they had ever been pregnant and how old they were when their first pregnancy began. The self-reported teen pregnancy measure was complemented by urine-based pregnancy testing at the visit in emerging adulthood. Participants assigned male at birth were asked if they had ever gotten someone pregnant and how old they were when they first got someone pregnant.
Diagnosis of any STI was measured using a combined measure of self-report and biologically-detected chlamydia and/or gonorrhea. Via self-report, all participants were asked “Have you ever been told by a doctor, nurse or other health care provider that you had a sexually transmitted infection?” If they answered yes, they were asked to select which STI had been diagnosed. Additionally, chlamydia and gonorrhea testing was conducted using a nucleic acid amplification test from a first catch urine sample or self-obtained vaginal swab (for participants with a vagina). Those testing positive were notified of their results by a study physician and referred for treatment to a provider or clinic of their choice at no cost to participants.
The exposure of TFA was self-reported using a 6-item scale of Cyber Dating Abuse that has been previously validated and used in AYA [22]. Responses were on a five-point Likert scale of frequency ranging from never to every day. Participants were asked “In the past 6 months, how many times has a partner done any of the following things using mobile apps, social networks, texts or other digital communication?” At wave 6, they were asked in relation to the past 12 months. Example items included “made mean or hurtful comments to you,” “repeatedly contacted you to see where you were/who you were with,” and “spread rumors about you.” Participants were defined as having experienced any TFA if responded that they were repeatedly contacted by a partner to see where they were/who they were with every day or almost every day or if they had ever experienced any of the other items. Participants who did not have a partner were coded as not having experienced TFA.
Drawing from approaches used in other violence exposure scales [23, 24], which incorporate frequency and severity into their assessment, an intensity score was also created from the TFA items. This was done by multiplying the number of abusive behaviors experienced by the frequency that they were experienced and by a measure of severity for each item. Severity scores ranged from 1 to 3 where 1 = mild, 2 = moderate, 3 = severe. Items were scored by a group of staff (MH and MS and reviewed by the team) and were based on their prevalence, and assessments of the psychological or physical harm they are likely to cause. For example, posting nude pictures or image-based abuse, which was less common and has been associated with severe mental health concerns including PTSD and suicidality [25], was ranked higher than mean comments. The TFA intensity score was further categorized into low [1,2,3], medium [4,5,6,7,8,9,10], and high (10 and up) scores based on the distribution of scores within the sample.
CovariatesPotential confounders were measured at baseline and included age (years), sex at birth, neighborhood disorder (high vs. low), mother’s educational level (less than high school, high school/GED, more than high school), food insecurity (yes/no), and symptoms of depression (yes/no). Neighborhood safety was measured by the number of disorder events exposed to, out of 11 types, during the past year (e.g., “I saw people dealing drugs near my home”). A sum of the total number of events occurring at least once during the past year was calculated and was dichotomized as high (≥ 5 events) versus low (< 5 events) based on prior analyses [15]. Any substance use was defined as self-reporting use of alcohol, marijuana, prescription drugs or illicit drugs in the past 6 months. Food insecurity, was measured with two questions that assess limited or uncertain access to adequate food aligned with USDA assessments (e.g., “In the last 6 months, were you ever hungry but didn’t eat because there wasn’t enough money for food?” and “In the last 6 months did you ever eat less than you felt you should because there wasn’t enough money to buy food?”) [26].
Data analysisFirst, we examined baseline (Wave 1) demographic characteristics among those who did and did not experience TFA at the Wave 2 study visit when it was first asked (median age 13.8 years). We reported frequencies and percentages for categorical variables and medians with the interquartile range (IQR) for continuous variables. We then described individual TFA items over time at all visits and bivariate relationships between experiences of any TFA in early and middle adolescence (~ ages 13–15; wave 2–5) with outcomes in emerging adulthood (~ age 20; wave 6). Again, we reported frequencies and percentages for categorical variables and medians with the interquartile range (IQR) for continuous variables. Next, we used log-binomial models to estimate risk ratios (RR) and 95% confidence intervals (CIs) for the associations between any TFA experienced from partners in early and middle adolescence (wave 2–5) with sexual health, mental health and violence outcomes in emerging adulthood (wave 6). Log-binomial models were selected because the outcome was dichotomous and because odds ratios are inflated if the outcome is common. In the case that log-binomial models did not converge, we used log-Poisson models with robust standard errors. We also explored interactions between TFA and sex at birth in all models and examined associations with TFA intensity and outcomes using log-binomial models similar to those described above.
EthicsAt study enrollment in 8th grade (Wave 1), all adolescents provided informed assent to participate following verbal parent permission. At the visit in emerging adulthood (Wave 6), all participants provided written informed consent as they were aged 18 years or older. Incentives were provided at each study visit and all youth received a referral guide to relevant community resources. At Waves 1–5, participants who screened positive for depression or had other mental health needs were offered a fast-track referral to behavioral health services through a mechanism established by the study with the local health department. At Wave 6, participants testing positive for STIs were contacted by a study physician to ensure treatment was accessed and available free of cost. Participants who reported experience of violence or screened positive for depression or had other mental health needs were offered referrals to behavioral health services. The RTI International Institutional Review board reviewed and approved all study procedures.
Comments (0)