
Remember me


A concurrent mixed study was employed (the quantitative study employed an institution-based cross-sectional study design, while the qualitative study employed a phenomenological study design) in the administrative town of the Wolaita zone from April 5 to May 30, 2022. The Wolaita zone borders the southern Gamo Gofa and Dawuro Zones, the northeastern Kambata Tambaro zone, the northern Hadiya Zone, and the southwestern Sidama Zone. Wolaita Sodo town is the capital of the Wolaita zone and is located approximately 312 km southwest of Addis Ababa, the capital city of Ethiopia, and 166 km from the regional capital city Hawassa. There are seven administrative towns in the Wolayita zone. Based on the 2020 population projection conducted by the Central Statistical Agency of Ethiopia (CSA), the Wolaita zone has a total population of 5,385,782 with an area of 451,170.7 hectares [23]. According to the 2019 Wolaita Labor and Social Affairs Report, there are 18,913 disabled people in the Wolaita Zone; from those 10,403 people are male, and 8,510 people are female. Of those 1561 women of reproductive age in each town, there is a disabilities association that serves people with disability [24].
Source populationAll reproductive-aged women with disabilities who live in administrative towns of Wolaita zone are known by the wolaita zone union of people with disabilities.
Study populationWe randomly selected reproductive-aged women with disabilities who lived in the administrative town of the Wolaita Zone and who were known by the Wolaita Zone union of People with Disability Association.
Eligibility criteriaAll reproductive-age women with hearing, visual or limb impairment were included in the study, except for women who were pregnant during the data collection.
Women with disabilities who were able and willing to provide detailed information were included in the qualitative study.
Sample size determinationThe sample size of the study was calculated using OpenEpi version 3.0 software, with the following assumptions: 95% confidence interval, 80% power, and anticipated proportion (p = 33.7%) [22]. With these inputs, a sample size of 313 was used; therefore, after a 10% nonresponse rate was added, 343 samples were ultimately proposed for the study. In the qualitative study, women with disabilities who were not participated in quantitative study were involved in individual in-depth interviews.
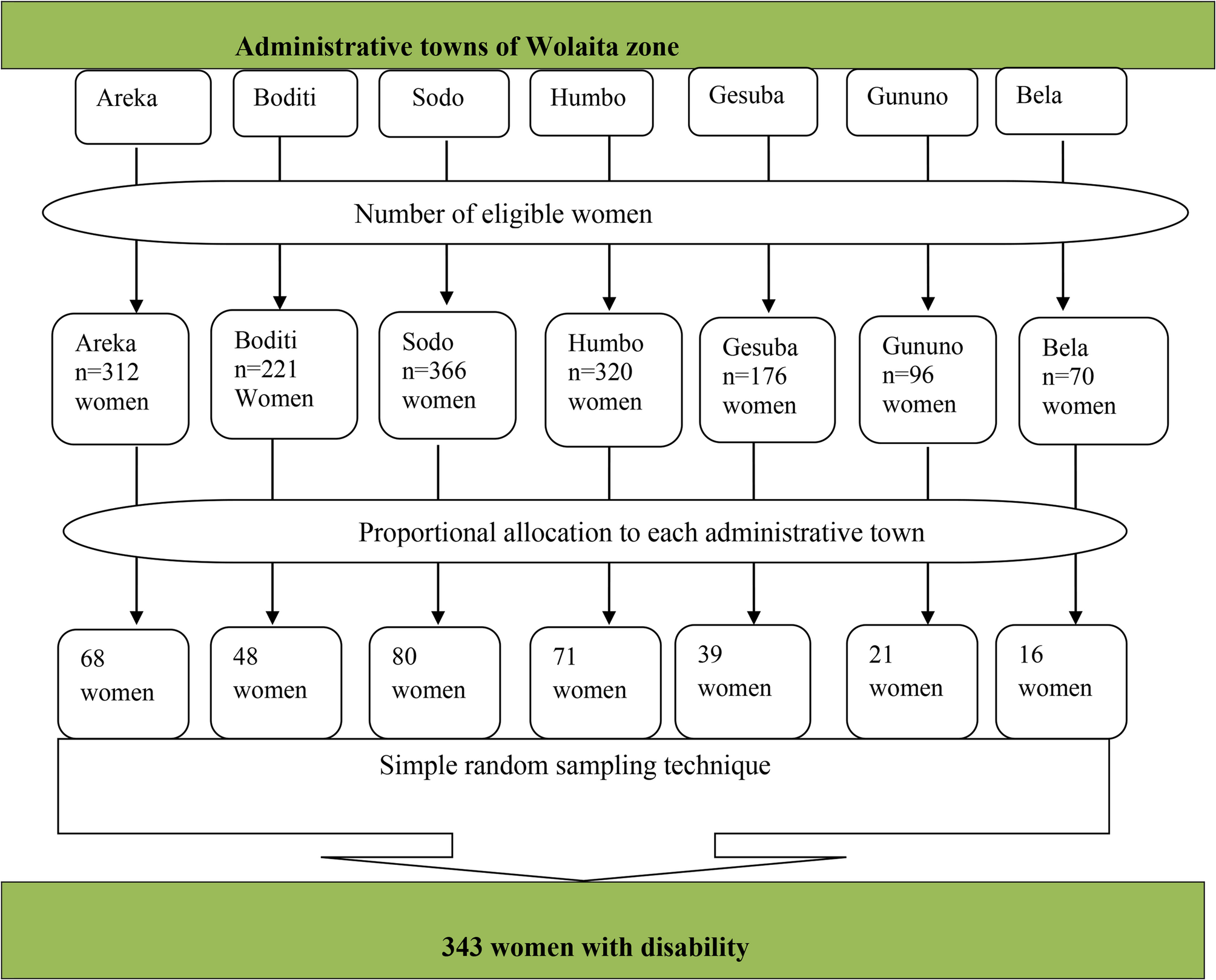
Sampling technique and proceduresAll seven administrative towns were included in the study. The sampling frame was developed from the Wolaita Zone Labor and Social Affairs Registration Book. Among the total of 8,510 disabled people in the zone, 1,561 women of reproductive age with hearing, visual, or limb defects were included in the sampling frame. The number of women included from each town was allocated proportionally to the number of eligible women. Participants in the study were recruited by simple random sampling via the lottery method using their ID number from the registration Excel sheet (Fig. 1).
Fig. 1
Schematic presentation of sampling procedure of modern family method utilization and associated factors among women with disability in Wolaita zone, Ethiopia, 2022)
For the qualitative study, participants were selected using a purposive sampling technique, participants who were well informed about the case and able to explain detail about phenomena were interviewed and the recruitment ceased after interviewing 11 participants, when data saturation was achieved, (Six women with physical impairment, 2 women with hearing impairment, and 3 women with visual impairment were included in the study.
Data collection toolQuantitative data were collected through face-to-face interviews using a pretested and semi- structured questionnaire developed from the EDHS survey tool and different literature [9, 21, 22]. The questionnaire was prepared in English and was translated into the “Wolaitegna” local language by a local language expert to maintain consistency of the language. The questionnaire included five sections: sociodemographic characteristics, sexual and reproductive health history-related questions, participants’ knowledge of modern family planning methods and attitudes toward modern family planning methods, and modern family planning methods.
For the qualitative study, the interview guiding questions were first prepared in English and subsequently translated into two languages (the Amharic and Wolaiytegna languages).
Data collection procedureThe data were collected by seven experienced health professions (3 BSc midwifery and 4 diploma nurses), and two other sign language experts for hearing-impaired participants were involved. Three health professionals (BSc midwifery) were assigned as supervisors. The data were collected in Wolaita Dona.
Qualitative data were collected through individual in-depth interview using interview guide questions by principal investigators who can speak and read local language. Audios were taped using a digital voice recorder and average length of the interview is 37 min. For hearing-impaired participants, the interview was interpreted by a sign language translator. The data collection was done in Wolayita zone union of disability association participants own office and other participants’ preferable area (home) which is free from traffic and noise.
Data quality controlFor the quantitative survey, an interviewer-administered structured questionnaire was first prepared in English and subsequently translated into the Wolayitegna local language by a language expert and subsequently returned to English to maintain consistency. Two days of training were given to data collectors and supervisors about the objective of the study, the relevance of the study, how to get/select respondents, the data collection/interviewing approach and proper filling/data recording by the principal investigator. A pretest was conducted on 5% of the sample (14 WWDs) in Arbaminch town. Based on the pretest, clarity, potential misinterpretations, appropriateness of wording, logical sequence and skip patterns were ensured accordingly before the actual data collection.
The data collection processes were closely followed by the supervisors. The completeness, consistency and accuracy of the data were checked daily by supervisors and principal investigators. Incorrectly filled or missed data were sent back to the respective data collector for correction.
The trustworthiness of the qualitative findings was maintained by focusing on four criteria: credibility, dependability, confirmability, and transferability.
Credibility: Before starting the data collection, participants were informed that they would be reported to relevant people in the association. The investigators were exposed to the qualitative data collection and analysis. Some of the study participants reviewed whether the findings correctly represented their views and ideas. The expressions of the respondents were narrated directly word by word.
Dependability: The content of the manual transcripts is verified by the investigator through reviewing the audio records of the interviews. To maintain consistency of the interpretation, cross-checking was performed with audio records of the interviews and transcription and notes taken during the interviews.
Confirmability: Before the interview, the investigators reflected on and considered their prior personal expectations and experiences to reduce bias during the data collection, coding and analysis.
Transferability: The study process was cascaded with consideration of qualitative study concepts. The findings were facilitated by providing information about the research context, methodology, and participants. Verbatim quotations from the interview transcripts were used to illustrate relevant themes. Participants were selected purposively through their ability to provide in-depth information about the phenomenon.
Data analysis processAll the field questionnaires were checked for completeness, consistency, and accuracy by an investigator, and the data were subsequently coded entered, and cleaned using Epi-Data version 4.6 software and exported into SPSS version 26 for analysis. Descriptive statistics were carried out by using simple frequency, median, and IQR. Data were presented in text, tables, and figures (charts).
Independent variables with P values ≤ 0.25 in the bivariable logistic analyses were selected for multivariable logistic analysis. Both the crud odds ratio (COR) and adjusted odds ratio (AOR) with 95% CI were determined, and variables with p-values less than 0.05 were considered statistically significant factors.
The qualitative data were analyzed using thematic analysis via an inductive qualitative data analysis approach. All the individual IDI data were transcribed and translated word by word (verbatim). Coding interesting features of the data systematically across the entire dataset was performed. The coding was executed by the qualitative data analysis software Open code version 4.03. Then, the codes were categorized according to each potential subtheme and further into themes. Finally, the findings were summarized and triangulated with the quantitative results and are presented in the text, table and chart.
Ethical clearance and consent to participateEthical clearance was obtained from the Wolaita Sodo University Research and Ethical Review Committee, and an official letter was written from the School of Public Health to the Wolaita Zone Union of Person’s Disability Association. Furthermore, a supportive and permission letter was written to each administrative town’s disability associations. Finally, informed verbal and written consent was obtained from the study participants. To maintain the confidentiality of the study, participants’ names or other identifiers were represented by code numbers. Generally, throughout the study process, the confidentiality and anonymity of the study participants were maintained.
Comments (0)