This case–control analysis comprised 60 children and adolescents (up to 18 years old) with CLD of various causes, selected from Benha University Hospital's Pediatric Department's Pediatric Hepatology Clinic (32 patients were males and 28 were females with a mean age ± SD of 9 ± 4 years). An additional 60 healthy children from the overall community who were matched by age and sex served as the control group (22 children were males and 38 were females with a mean age ± SD of 11 ± 2 years).
Inclusion criteria for cases
Children under 18 years of both sexes were diagnosed with CLD, including hepatitis B or C, autoimmune hepatitis, cholestatic liver disorders, or metabolic liver disorders, with liver fibrosis previously identified through clinical, biochemical, and radiological assessments and confirmed by LB.
Inclusion criteria for controls
Controls were healthy children who volunteered from outpatient clinics during routine check-ups for the purpose of sport training and school routine examination, matched for age/sex, with normal liver function investigations, with no previous history of a liver disorder.
Exclusion criteria for both case and control
Malignancies, severe systemic diseases (active sepsis, advanced cardiopulmonary or renal dysfunction, connective tissue or neoplastic disorders), and hematologic conditions (e.g., von Willebrand disease, thrombotic thrombocytopenic purpura, bone marrow disorders, or possible hemolytic–uremic syndrome) were excluded.
Sample size calculation
The sample size was calculated using G*power software version 3.1.9.7 based on a previous study [13], which reported a large effect size of Von Willebrand Factor between patients and controls. The total sample size needed to detect a large effect size (d = 0.8) of Von Willebrand Factor between the studied groups was 90 patients. The sample was increased to 120 patients (60 per group) to compensate for possible use of non-parametric tests and possible laboratory failure. Alpha and power were adjusted for 0.05 and 0.95, respectively.
All participants were subjected to
A.
Clinical Evaluation
A thorough physical examination and history were taken. Body mass index (BMI), weight, and height were all assessed as part of anthropometrics. Egyptian pediatric references were used to compute percentiles.
B.
Radiological investigations
All cases were asked to report abdominal ultrasound and Doppler for detection of ascites, portal hypertension, and size of liver and spleen.
C.
Laboratory investigations
A complete blood count (CBC) was made with 1 mL of whole blood collected in an EDTA (Ethylene-diamine-tetra-acetic acid) vacutainer and gently mixed to prevent clotting. Hematological parameters, including hemoglobin concentration (Hb), mean corpuscular volume, mean corpuscular hemoglobin, red cell distribution width, and mean corpuscular hemoglobin concentration, were measured using the Sysmex KX-21N automated hematology analyzer (Sysmex Corporation, New York, USA). For differential leukocyte counts, peripheral blood smears were prepared and stained using Leishman’s stain.
Liver function tests, including aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase, gamma-glutamyl transferase (GGT), total serum protein, serum albumin, total serum bilirubin (TSB), and direct serum bilirubin (DSB), were performed following the collection of 4 mL of venous blood into plain tubes devoid of anticoagulant. Samples were given time to coagulate, then centrifuged at 1500 rpm for 15 min. The biochemical analyses were carried out using the Biosystem A1A autoanalyzer (Spain).
Coagulation profiles, including prothrombin time (PT), partial thromboplastin time (PTT), and international normalized ratio (INR), were evaluated using the HUMACLOT DUE PLUS® coagulation analyzer (Wiesbaden®, Germany).
In cases diagnosed with autoimmune hepatitis, gamma globulin titer, anti-nuclear antibodies (ANA), anti-smooth muscle antibody (ASMA), and anti–liver-kidney microsomal (anti-LKM) antibody titers were determined using the indirect immunofluorescence technique with INOVA Diagnostics, Inc. (Germany), offering NOVA Lite Rat Stomach, Kidney, and Liver kits.
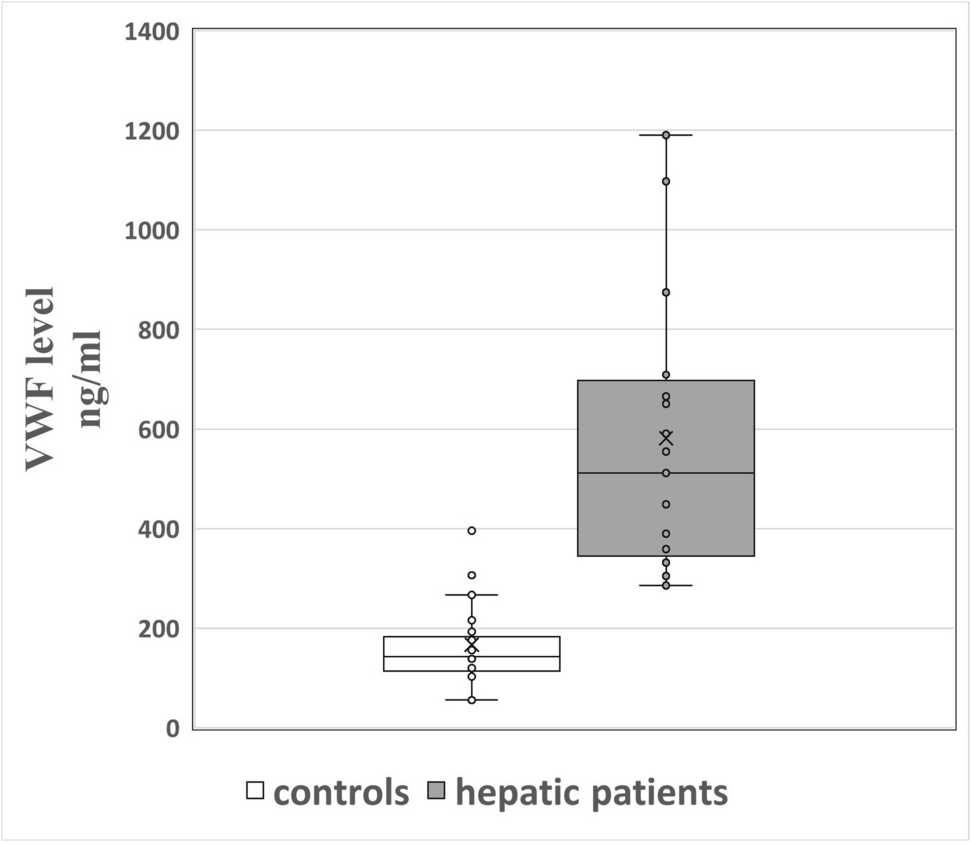
Plasma VWF antigen (VWF Ag) titer was measured using the Human vWF ELISA Kit (Catalog No: DLR-vWF-Hu). Samples of peripheral blood were drawn without the use of a tourniquet, placed in tubes with heparin or EDTA as anticoagulants, and brought to the lab in an iced box. Samples were centrifuged at 1000 × g for 15 min at 2–8 °C within 30 min of assembly. For further examination, the extracted plasma was aliquoted and kept at −20 °C or −80 °C. VWF Ag typically ranges between 50 and 200 ng/ml.
Non-invasive serological markers were used for detection of fibrotic liver. These include APRI score (AST/platelet ratio index) and fibrosis-4 (FIB-4) score using age, platelet count, ALT and AST.
D.
Liver biopsy (LB) and staging
LB was done for CLD patients only. Every patient had a liver biopsy performed using the Menghini aspiration needle method under ultrasound guidance. All biopsies contained ≥ 11 portal tracts (median: 15, ranged from 11 to 20) as confirmed by histopathology. Formalin and paraffin were used to preserve biopsy specimens, which were then placed on a glass slide and stained with hematoxylin and eosin to determine the histological activity of hepatitis using the Ishak score. Masson trichrome was used to determine the stage of fibrosis. The fibrosis stages extended from F0 to F6 (F0 = no fibrosis, F1 = mild, F2-3 = moderate, F4-6 = severe) [14]. Patients with cirrhosis were categorized clinically according to Child–Pugh, MELD, and PELD scores as follows:
PELD score: For younger children (below 12 years old), it was used to evaluate its impact on growth and decide whether liver transplantation was necessary. It is useful for estimating the predicted death rate from hepatic disease. It was calculated according to the formula; PELD = 4.80[Ln serum bilirubin (mg/dL)] + 18.57[Ln INR]—6.87[Ln albumin (g/dL)] + 4.36 (< 1 year old) + 6.67(growth failure) [15].
MELD score: It proved to be helpful in assessing prognosis and setting priorities for liver transplant recipients. It was calculated according to the following formula: MELD = 3.78 [Ln serum bilirubin (mg/dL)] + 11.2 [Ln INR] + 9.57 [Ln serum creatinine (mg/dL)] + 6.43 [16].
Child–Pugh scoring system: Its purpose was to forecast mortality in cirrhosis patients. Patients were divided into three groups: those with excellent liver function (A), those with mild liver function impairment (B), and those with advanced liver dysfunction (C). To classify patients, they used five clinical and laboratory criteria: prothrombin time, ascites, neurological disorders, serum bilirubin, and serum albumin [17, 18].
Statistical analysis
Data were analyzed using SPSS v28. Normality was assessed via the Shapiro–Wilk test and visual inspection. Normally distributed data were reported as mean ± SD, non-normal as median (range), and categorical variables as n (%). Group comparisons used t-test/Mann–Whitney U (quantitative) or chi-square/Fisher’s exact (categorical). Kruskal–Wallis test with Dunn’s post-hoc correction was used for ≥ 3 non-parametric groups. ROC analysis evaluated VWF’s diagnostic performance for liver fibrosis (area under the curve, AUC, cutoff, sensitivity/specificity). Spearman’s correlation assessed relationships. Significance was set at p < 0.05 [19].


Comments (0)