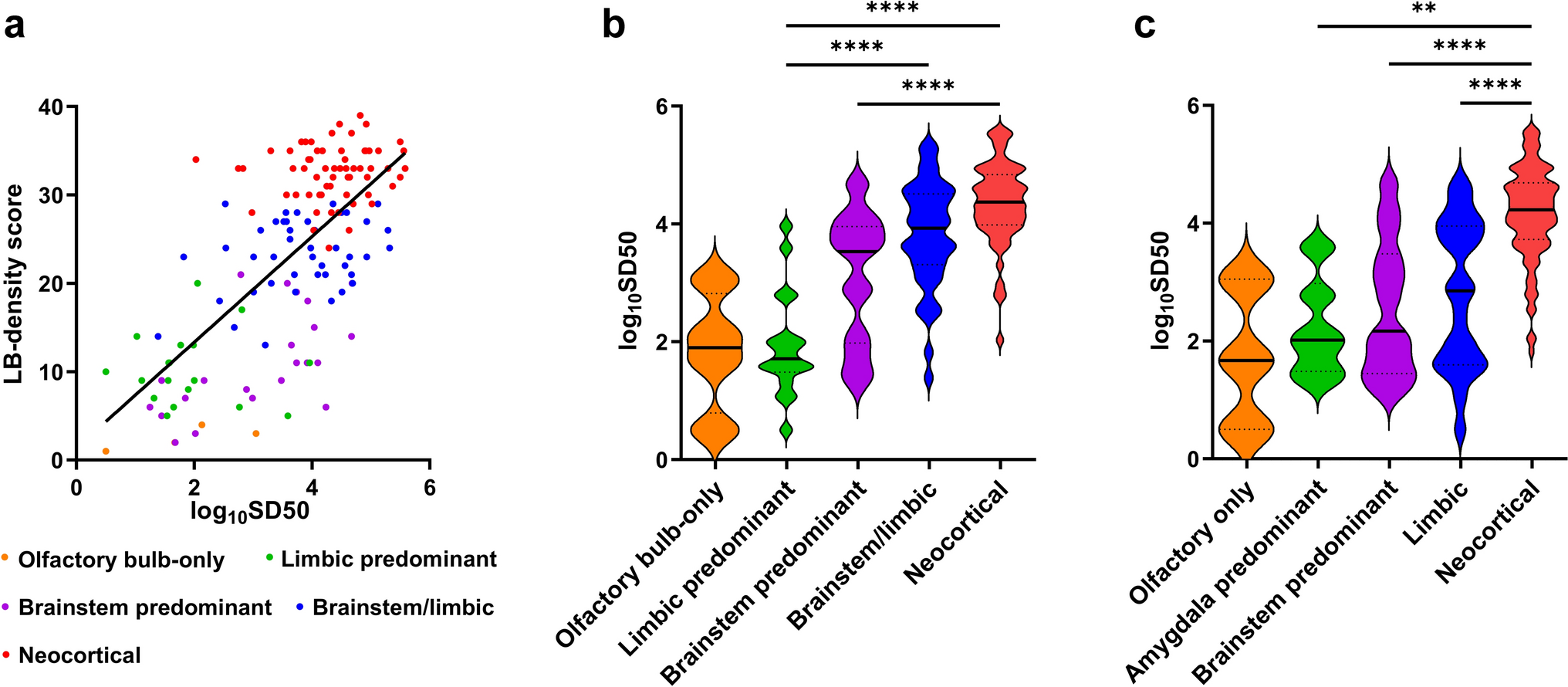
The search and validation of biomarkers that predict the stage and burden of the underlying neuropathological process are research priorities in neurodegenerative diseases. In a previous study, we demonstrated that α-syn RT-QuIC, the only pathology-specific in vivo marker available for synucleinopathies, executed on serially diluted brain homogenates, provides an estimate of the α-syn seed concentration that positively correlates with the LBD load evaluated through immunohistochemistry [8]. In this work, we tested whether a “quantitative” approach is feasible and reliable when using CSF. The results demonstrate that seed quantification based on endpoint dilution RT-QuIC applied to CSF samples enables a reliable prediction of the burden and extent of the underlying LBD. Specifically, SD50 values showed a strong positive association with the brain LB-density score, a measure of LBD burden detected by immunohistochemistry, and with LBD stages, with more advanced LBD pathology corresponding to higher SD50 values (i.e., higher seeding activity). This suggests that, in patients with LBD, α-syn seeds are effectively released in the CSF to an extent proportionate to the burden of the underlying proteinopathy. Notably, LBD patients with more extensive pathology, as expected, displayed a more severe pathology in each different brain region, as expressed by LB pathology semi-quantitative severity scores, and these were also significantly associated with SD50 values.
When examined in more detail in participants stratified by the LBD stage, SD50 values and LB-density scores showed a significant positive association only in those at the USSLB brainstem-predominant stage and those at the LPC limbic and neocortical stages. The small sample size in some groups must be considered when interpreting these results. However, the suboptimal correlations likely also reflect the heterogeneity of LB scores across groups defined by the two classification systems, affecting the discriminative power of SD50 values.
Besides the association with pathology severity, we demonstrated significant correlations between the SD50 values and the last available clinical scale scores, such as the UPDRS part III for motor impairment and the UPSIT for olfactory dysfunction. Notably, these associations remained significant in the whole LB-positive/SAA-positive group, even after excluding subjects with significant AD co-pathology, but not after stratification by clinical diagnoses. This is probably due to the limited number of participants in each subgroup. Moreover, it is relevant that even the associations between clinical scale scores and LB-density scores almost failed to reach statistical significance. Unlike motor and olfactory impairment, which are more specifically linked to LBD, cognitive impairment (as measured by the MMSE scale) was not associated with SD50 values in any analysis. This result may be explained by the multifactorial nature of cognitive impairment in patients with LBD [13, 23, 26, 42], where co-pathologies, such as AD and vascular disease, also play a significant role. In this scenario, the significant negative association between LB-density score and MMSE we obtained in the whole LB-positive/SAA-positive group may reflect the high prevalence of high-grade AD co-pathology, which may be a key driver of lower MMSE scores, although a recent study from the AZSAND cohort, but with a larger sample size, found a statistically significant association between the two variables, independent of AD pathology [7]. Other cognitive measures might show stronger associations, as the previous studies have suggested that the MMSE may not be the most appropriate tool for assessing cognitive impairment related to LBD. Further studies should investigate the associations between SD50 and other scales of cognitive dysfunction, with a focus on executive and visuospatial abilities, such as the Montreal Cognitive Assessment (MoCA).
Our analysis of the performance of the SD50 values, alone or in combination with clinical parameters, for distinguishing participants at neocortical-stage LBD or with high LBD burden from those with less-advanced pathology warrants discussion. The spread of LBD to the neocortex represents the final stage of this proteinopathy, is associated with the development of cognitive impairment, and has, therefore, independent prognostic implications [17, 20, 28, 42]. However, clinicopathological studies demonstrate that the presence of dementia alone in patients with clinical LBD is neither sensitive nor specific to neocortical-stage pathology [12, 26, 28, 35]. Our results support this finding, but also show that SD50 values, either alone or in combination with scores of olfactory impairment, are highly effective in identifying participants at a neocortical stage, outperforming the presence of dementia or UPSIT scores. This was true in the whole LB-positive/SAA-positive group, including clinically unimpaired participants, representative of the general population, as well as in participants with a clinical diagnosis of PD or AD dementia, albeit not reaching statistical significance. Notably, in participants with a clinical diagnosis of AD dementia, both SD50 and the combination SD50/UPSIT yielded full sensitivity (100%). Moreover, SD50 values accurately identified participants with a high burden of proteinopathy. The utility of olfactory function scores in identifying participants with LBD is well known from clinicopathological studies [5, 45]. Moreover, a recent study suggested that worsening olfactory function may be a surrogate biomarker of LBD progression [32]. Our data expand on these results and demonstrate that, in a cohort which is virtually representative of the general population, quantifying α-syn seeds in CSF, alone or in combination with olfactory function assessment, may help identify LBD participants at a neocortical stage in research settings. This would be relevant in clinical trials of disease-modifying agents for PD, with participants showing LBD at a higher stage or burden possibly benefiting the least from therapies, and in AD dementia, where subjects with advanced LBD co-pathology may warrant exclusion from initial recruitment.
As an ancillary result, we confirmed here the high specificity of our RT-QuIC assay in another neuropathological cohort by showing that only six participants (3.2%) without LB pathology tested positive on the assay. Notably, these subjects had low SD50 values, comparable to those obtained in LB-positive/SAA-positive participants at LBD stage I, primarily exhibiting focal pathology restricted to the olfactory bulb. Therefore, it is possible that our “false positive” subjects may indeed show focal LB pathology in some central nervous system regions due to the sparse LB-density.
Moreover, this study confirms that a low LBD burden and/or stage is the primary determinant of incomplete α-syn RT-QuIC sensitivity [8, 22]. Indeed, all our LB-positive/SAA-negative participants exhibited a low LBD burden, with LB-density scores comparable to those of LB-positive/SAA-positive individuals at USSLB stage I, and most were classified as USSLB stage I, IIa, or IIb. Regarding the diagnostic performance of α-syn CSF RT-QuIC in patients in the latter group, also known as amygdala-predominant LBD, previous studies involving both antemortem and postmortem CSF samples reported a reduced sensitivity, with values ranging from 14.3 to 63.6% [1, 8, 22]. In our cohort, α-syn RT-QuIC yielded a sensitivity of 78.3%, comparable to that of a previous study using the same staging approach for LBD [22]. However, when considering only participants with LBD strictly confined to the limbic system (i.e., an amygdala-predominant stage according to the LPC), the test's sensitivity in our cohort dropped to 54.5%, which is similar to that reported in the other studies [1, 8]. Further studies are required to define other factors, besides the low LBD burden, that influence the limited assay sensitivity in LBD participants with focal limbic pathology.
A major strength of this study is the inclusion of a large, clinically well-characterized cohort with postmortem neuropathological analysis across different stages of LBD, including clinically unimpaired subjects. Another key strength is the robustness of our α-syn RT-QuIC assay, as shown here and in the previous works, along with the meticulous dilution process performed on over 150 CSF samples.
The use of postmortem ventricular CSF instead of in vivo collected samples represents a potential limitation of this work. Although there is currently no convincing evidence that the composition of lumbar CSF significantly differs from that at the ventricular level, postmortem CSF may undergo death-related modifications, potentially altering protein concentrations [4, 24, 40]. This may also affect α-syn seed concentrations, which are likely lower in antemortem sampled CSF, as recently suggested [21, 43]. Finally, we cannot fully exclude the possibility of contamination of CSF samples through the needle passing through the corpus callosum. However, based on our extensive experience with LBD staging using α-syn immunohistochemistry, LB pathology is not significantly present in the deep white matter, including the corpus callosum. Further studies based on in vivo sampled CSF should replicate the results obtained in the present study. Another technical issue that potentially limits the applicability of the present SAA protocol concerns the need for large amounts of α-syn-negative CSF for the endpoint dilutions. In this work, we used CSF samples from NPH patients who typically undergo evacuative lumbar puncture, but we recognize that the availability of such samples may be limited. Further studies should investigate the impact of other types of diluting matrices, such as artificial CSF, on the assay kinetics and the accuracy of seed quantification.
In conclusion, we describe the first pathology-specific approach for LBD staging based on a biological fluid which can be obtained in vivo. Endpoint dilution RT-QuIC from periventricular CSF provided an accurate quantification of α-syn seeds, strongly correlating with the LBD stage and burden, as evaluated through immunohistochemistry, and was associated with clinical severity scores. The SD50 values, alone or in combination with clinical scales of olfactory impairment, showed a high value in identifying LBD participants at a neocortical stage and may be used in research settings for distinguishing subjects with advanced pathology from those at earlier LBD stages.





Comments (0)