Parathyroid lipoadenomas are benign tumors composed of parathyroid cells and adipocytes. Histological diagnosis is occasionally problematic because normal parathyroid glands contain at least 25% adipocytes [1]. In this study, groups 1 and 4 had typical parathyroid adenoma and lipoadenoma characteristics, respectively. However, groups 2 and 3 had intermediate fat volumes. By comparing these groups, the influence of adipocyte volume on US findings was determined.
Cervical US is recommended for the detection of parathyroid adenomas in patients with hyperparathyroidism. The diagnostic accuracy is high and the cost is lower than that of other imaging modalities [6]. However, in cases with a lipoadenoma, the detection rate is 58% [12]. In the present study, the detection rate of lipoadenomas was 20.0%, which was significantly lower than that in groups with no or fewer adipocytes, and it increased to 80.0% after obtaining information from other imaging modalities. This suggests that the localization of lipoadenomas by means of US alone is difficult; however, they can be detected to the same degree of accuracy as parathyroid adenomas if the US findings are well defined. In addition, it is unlikely that the degree of experience of the technicians affected the detection rate as the debatable cases were double-checked by senior technicians.
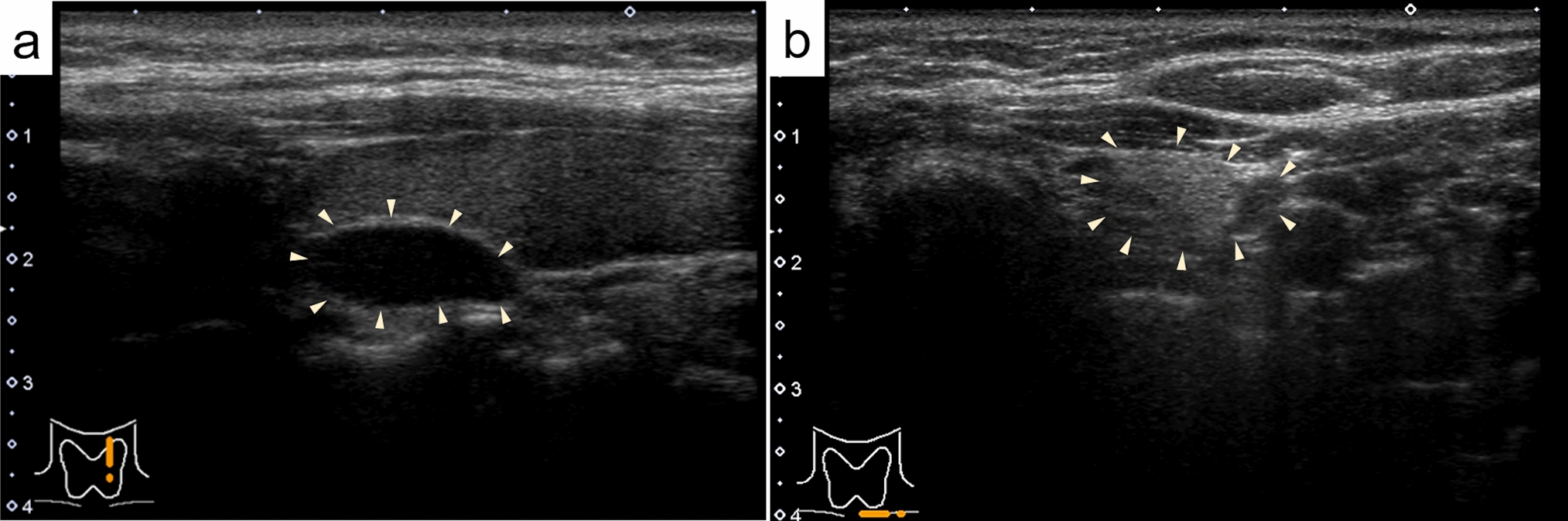
US findings of parathyroid adenomas are well documented. These tumors are characterized by an oval, predominantly solid, homogeneous, and hypoechoic nodule with a well-defined margin, polar artery, and hyperechoic line [7,8,9]. An enlarged feeding artery is also observed [9]. Parathyroid adenomas may contain a cystic area or be heterogeneous, especially when they are larger than 2 cm in size [9]. The internal vascular flow to a parathyroid adenoma varies. US findings of lipoadenomas in the literature are limited. Obara et al. reported that hyperechoic tumors are characteristic of lipoadenomas [7]. Their hyperechoic nature is due to the fatty stroma, which is the only distinction from a hypoechogenic parathyroid adenoma.
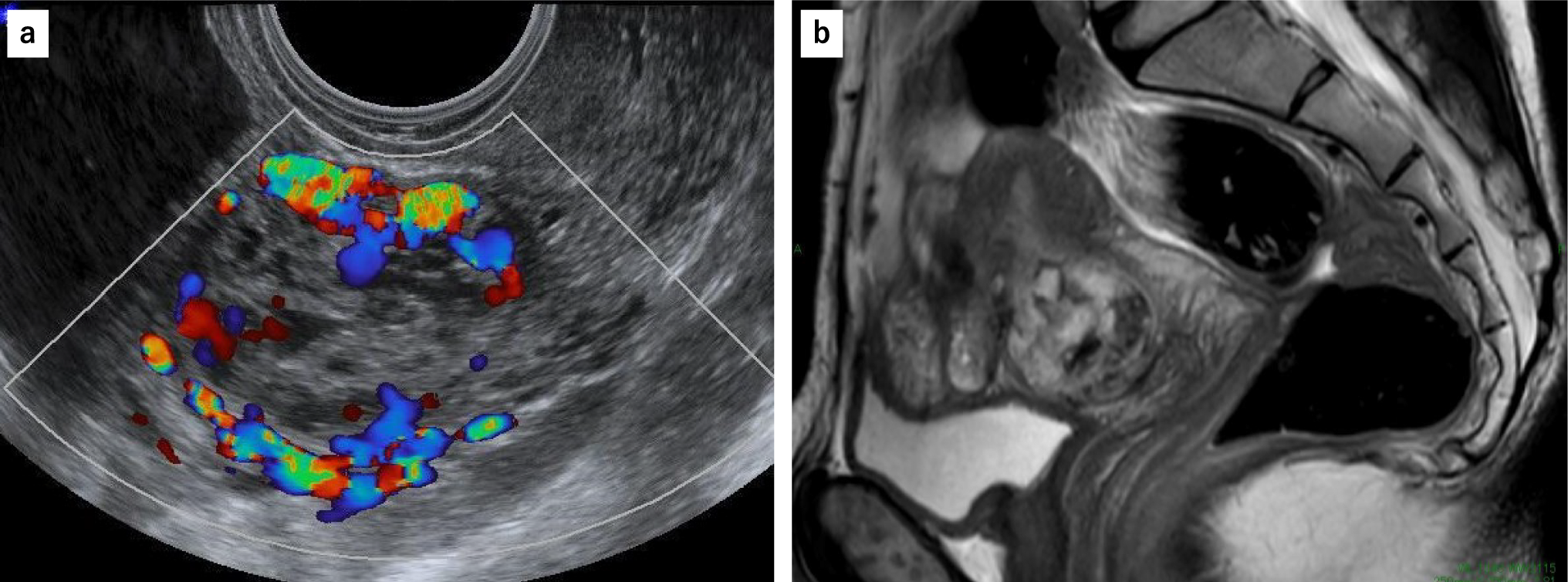
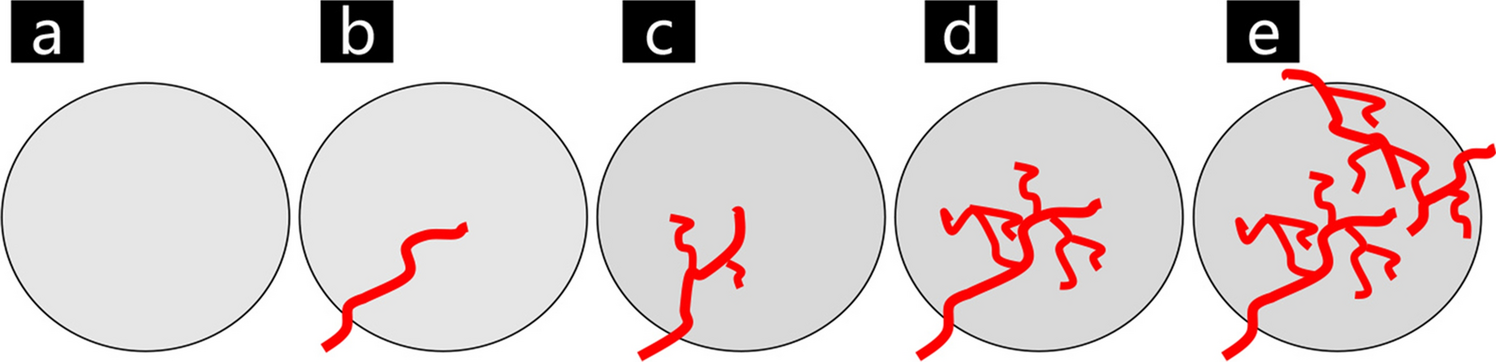
In the present study, we compared the US findings of adenomas with no or few adipocytes and lipoadenomas. Findings other than echogenicity were useful for differentiating between the two. The US findings of lipoadenomas are characterized by ill-defined margins, iso- and/or hyperechogenicity, heterogeneous consistency with a two-tone pattern, poor vascular flow, no polar artery, and no hyperechoic line. Because these findings are not features of parathyroid adenomas, they are thought to help differentiate between the two. In particular, we considered a two-tone pattern to be a significant finding suggestive of a parathyroid adenoma containing adipocytes and lipoadenoma. This may be due to the heterogeneous distribution of adipocytes. Moreover, we found that the blood flow in lipoadenomas is poorer than that in parathyroid adenomas. Previous studies have also shown that lipomas typically have a poor blood flow [19, 20]. Lipoadenomas predominantly comprise fat cells. Thus, the blood flow to a lipoadenoma is presumed to be poor relative to its size; hence, it was difficult to detect polar arteries.
Furthermore, another pitfall in the observation of lipoadenomas on US was identified. The tumor sizes of lipoadenomas on US tended to be smaller than their actual sizes. Only the hypo- or isoechogenic areas were judged to be nodules. The recognition that lipoadenomas typically have a heterogeneous consistency with a two-tone pattern may help avoid this pitfall.
A lipoadenoma containing excessive adipocytes, lipoma, and involuted ectopic thymus are considered part of the differential diagnosis for lipoadenoma. Lipomas are benign tumors composed of adipose tissue that are frequently found in the neck. On US, lipomas are oval and have varied echogenicity depending on the proportion of adipocytes and fibrous tissue. Striated echogenicity is characteristic of a lipoma [21, 22] and is helpful in distinguishing it from a lipoadenoma. An involuted ectopic thymus, called a phantom nodule, is present in the caudal region of the thyroid and appears as a well-defined, solid, homogeneous, and hyperechoic nodule [23]. In the present study, one lipoadenoma was interpreted as an ectopic thymus. An involuted ectopic thymus is usually not heterogeneous as in lipoadenoma [23]. Reactive lymph nodes may also be similar to those observed in lipoadenomas. Well-defined hypoechoic nodules with an eccentric echogenic hilum indicate reactive lymph nodes rather than a lipoadenoma [22]. The presence of hyperparathyroidism, knowledge of the US findings that are characteristic of lipoadenomas, and information on other imaging modalities may be helpful in differentiating between them.
The limitations of this study include its small sample size and retrospective nature.
In conclusion, we identified the US findings characteristic of lipoadenomas. These included ill-defined margins, iso- and/or hyper-echogenicity, heterogeneous consistency with a two-tone pattern, poor vascular flow, no polar artery, and no hyperechoic line. These findings are clearly different from those observed in parathyroid adenomas without adipocytes. We believe that focusing on these findings and referring to other imaging modalities increase the detection rate of lipoadenomas and allow us to consider them in the differential diagnosis. Future large-scale multicenter studies may be needed to further validate our findings.



Comments (0)