
Remember me


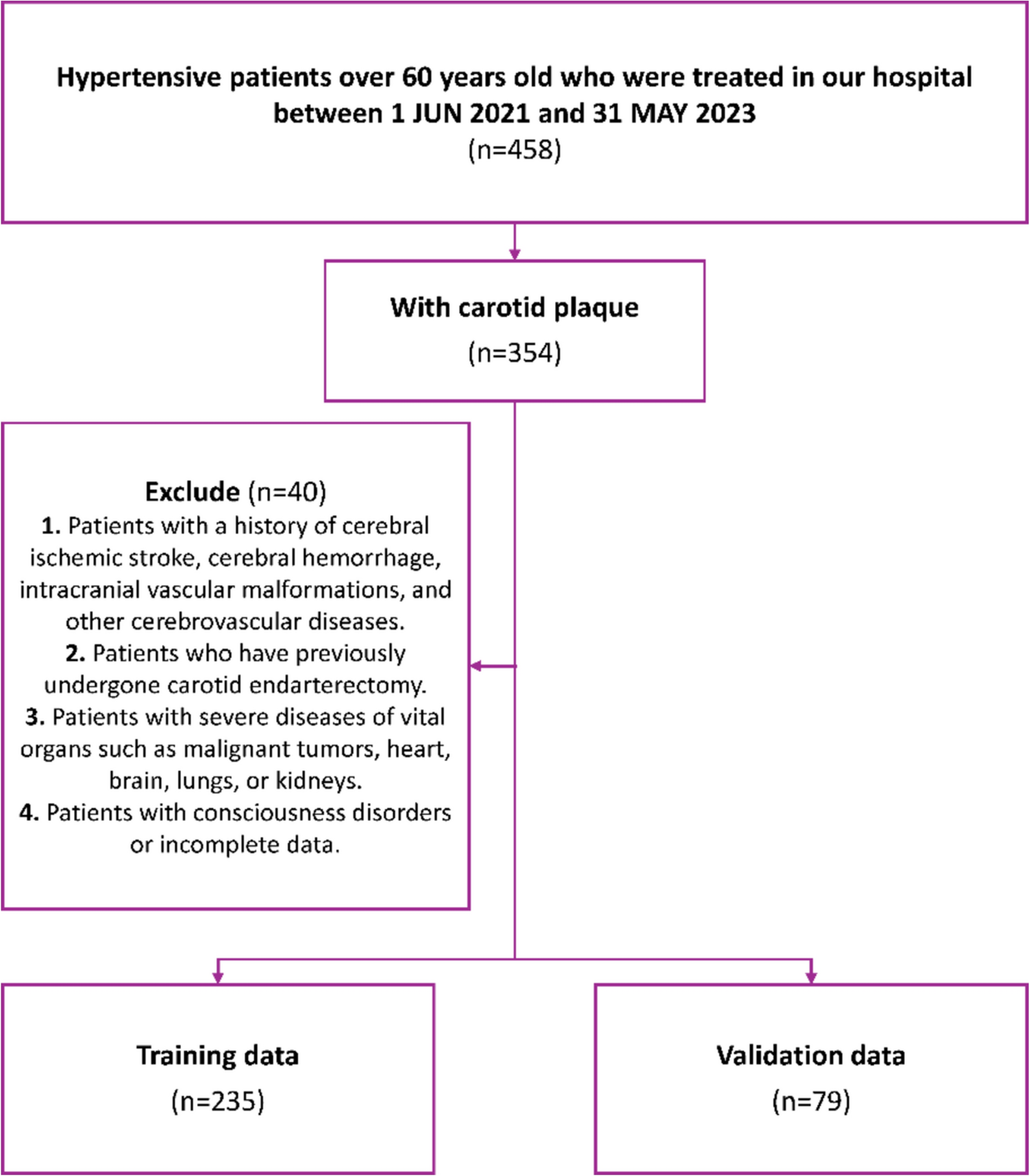
Based on the predefined inclusion and exclusion criteria, this study retrospectively included 314 elderly hypertensive patients with carotid plaques who were treated at our hospital between June 1, 2021, and May 31, 2023. The patients were randomly divided into a training cohort (235 patients) and a validation cohort (79 patients). They were categorized into a stroke group and a non-stroke group based on the diagnosis of ischemic stroke events (see Fig. 1).
Fig. 1
Flow chart showing selection of cohort
Inclusion and exclusion criteriaThis study was reviewed and approved by the Ethics Committee of the Chengde Central Hospital (CDCHLL2023-469). All enrolled patients signed written informed consent forms, in accordance with the Declaration of Helsinki.
Inclusion Criteria: (1) Age ≥ 60 years; (2) Diagnosed with primary hypertension, according to 2018 ESC/ESH Guidelines for the management of arterial hypertension [8]. (3) Diagnosed with carotid plaque by SMI examination at our hospital; (4) The patient or their legal guardian signed the informed consent form.
Exclusion Criteria: (1) Patients with combined or existing brain space-occupying lesions, cerebral hemorrhage, intracranial vascular malformations, or a history of cerebrovascular disease; (2) Patients who have previously undergone carotid endarterectomy (CEA) or carotid artery stenting (CAS); (3) Patients with severe diseases of vital organs such as malignant tumors, heart, brain, lung, or kidney; (4) Patients with chronic inflammatory diseases, infectious diseases, or wasting diseases; (5) Patients with consciousness disorders or incomplete data.
Criteria for hypertension diagnosisAccording to the 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension [8], hypertension is diagnosed when office blood pressure (BP) is ≥ 140/90 mmHg on at least two different occasions during separate visits, or if ambulatory BP monitoring shows a 24-h average BP of ≥ 130/80 mmHg, a daytime (awake) average BP of ≥ 135/85 mmHg, or a nighttime (asleep) average BP of ≥ 120/70 mmHg.
Hypertension is graded as follows: Grade 1 Hypertension is 140–159/90–99 mmHg, Grade 2 Hypertension is 160–179/100–109 mmHg, and Grade 3 Hypertension is ≥ 180/110 mmHg.
SMI examinationFor SMI examination, a TOSHIBA Aplio300 color Doppler ultrasound diagnostic instrument with a probe frequency of 3.0 to 11.0 MHz (model: 11L3) and built-in SMI imaging software was used. During the examination, the patient lay supine without a pillow, maintaining calm breathing, and the head was tilted back slightly toward the opposite side to fully expose the head and neck. Examination procedure: The target for observation was a plaque with a thickness of ≥ 2 mm and predominantly hypoechoic or mixed echogenicity. After clearly displaying the plaque image using two-dimensional ultrasound and keeping the probe in position, the patient was instructed to breathe calmly. The SMI mode was activated for examination, instrument parameters were set, and depth and gain were appropriately adjusted. The plaque was observed for more than 30 s to check for enhanced echoes within the plaque. Images were recorded and stored. SMI Detection Criteria for Neovascularization: continuous blood flow signals were detected in both transverse and longitudinal sections of the plaque. Transient or unstable flickering signals were considered artifacts and excluded.
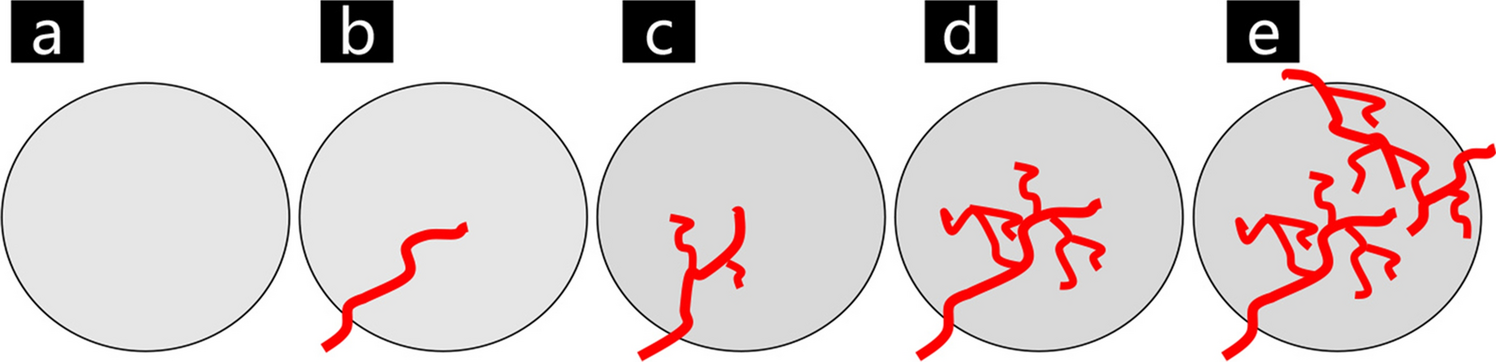
SMI blood flow grading is classified into four levels [15]: grade 0, no blood flow signal within the plaque; grade 1, one or several punctate blood flow enhancement signals within the plaque; grade 2, punctate or 1–3 linear blood flow enhancement signals within the plaque; and grade 3, multiple linear enhancement signals within the plaque, some traversing the entire plaque (Supplementary Fig. 1).
During the SMI examination in this study, measurements and recordings were performed by the same doctor with over three years of experience in vascular ultrasound examination, following standard operating procedures.
Clinical variablesBaseline characteristics: Gender, age, Body Mass Index (BMI), smoking history, and comorbidities (diabetes, hyperlipidemia, hyperuricemia, hyperhomocysteinemia, coronary heart disease, heart failure, COPD, gastritis and gastric ulcer, blood pressure system diseases) (Table 1).
Table 1 Baseline characteristics of hypertensive patients with carotid plaquesSMI features: Plaque acoustic features, plaque length, plaque thickness, plaque surface morphology, percentage area of stenosis, intraplaque neovascularization (IPN) grade, and blood flow rate within the plaque microvasculature (flow rate) (Table 2).
Table 2 SMI characteristics of hypertensive patients with carotid plaquesStatistical analysisStatistical analysis was performed using R (version 4.4.0). Categorical data were described as percentages (%) or composition ratios, and group comparisons were performed using the χ2 test. Normally distributed measurement data were described as mean ± standard deviation (M ± SD), and group comparisons were performed using the independent samples t test. Student’s t tests, Wilcoxon rank-sum tests, and univariate logistic regression were used to select features. Finally, Least Absolute Shrinkage and Selection Operator (LASSO) regression analysis was employed to identify significant variables and construct a multivariate binary logistic regression prediction model. The validation group externally validated the prediction model using receiver operating characteristic (ROC) curves and calibration curves. A P value of less than 0.05 was considered statistically significant.
Comments (0)