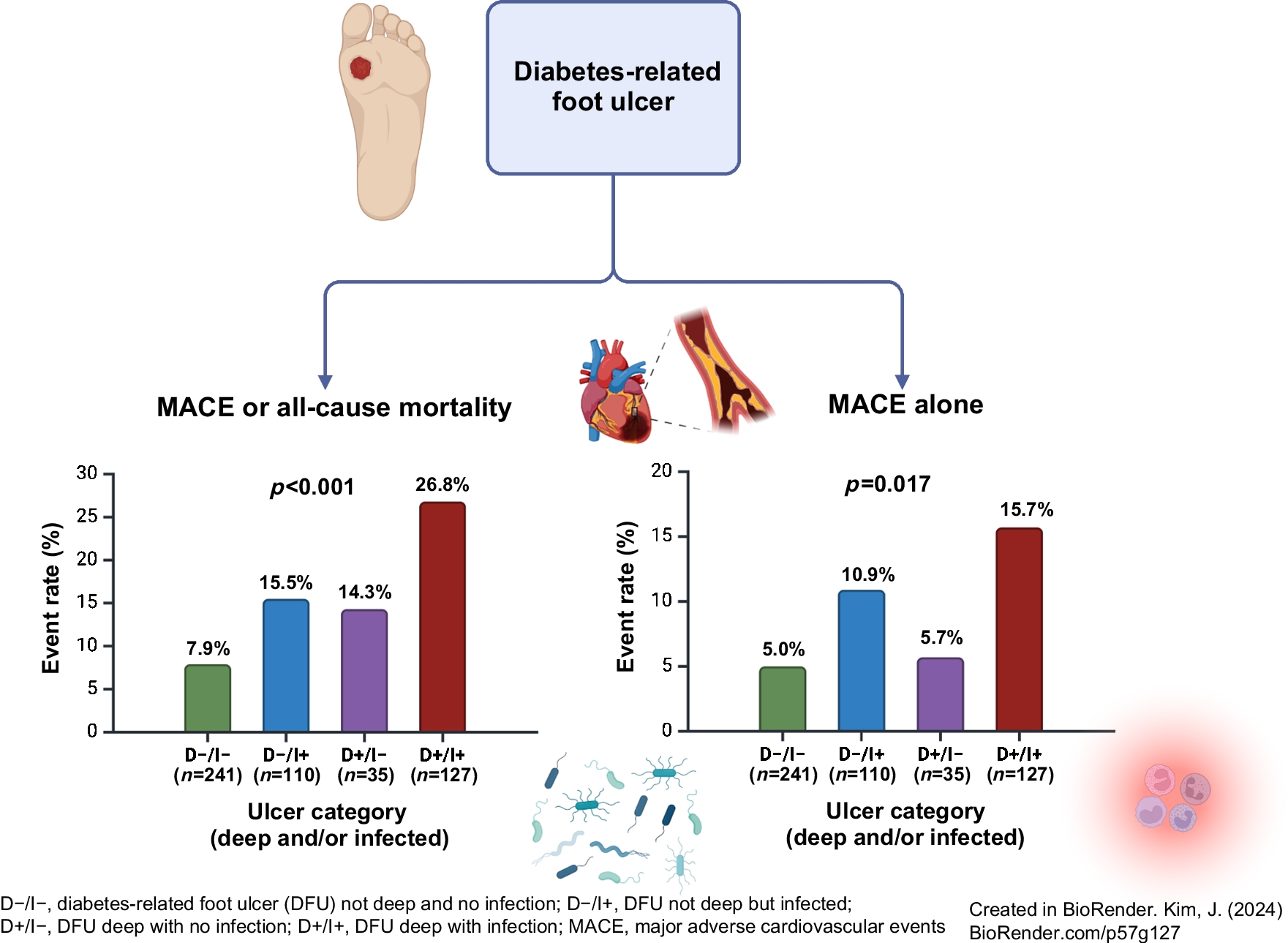
To the best of our knowledge, this is the first study demonstrating that deep ulcers (reaching muscle, tendon or deeper structures) and/or infected ulcers are associated with an increased risk of MACE, as well as MACE or mortality, in patients with DFU. This study also highlights a relatively high rate of MACE on the background of a high prevalence of major cardiovascular risk factors (or ‘risk enhancers’), including hypertension, dyslipidaemia, microvascular disease and established atherosclerotic CVD, including PAD and prior coronary artery revascularisation. The high rate of MACE is plausible, as the pathogenesis of DFU is multifactorial and is closely associated with underlying microvascular disease (e.g. peripheral neuropathy) and macrovascular disease (e.g. PAD) [31]. Despite this, multivariate analyses adjusting for several baseline comorbidities that are known to portend worse cardiovascular outcomes revealed that deep and/or infected DFU remains an independent predictor of future MACE. These findings provide a potential mechanistic explanation for the observed excess risk of CVD in people with DFU.
DFU represents a significant and highly morbid complication of diabetes, leading to lower-extremity amputation, disability, hospitalisation and substantial healthcare costs globally [32]. Among people with diabetes, the lifetime incidence of DFU ranges from 19% to 34% [33]. Notably, a meta-analysis has shown that five-year mortality approaches 50% in people with DFU, with approximately half of the explainable deaths being attributed to CVD [1]. In addition, a systematic review and meta-analysis demonstrated that people with DFU have a more than twofold higher risk of cardiovascular death compared with people with diabetes without DFU [4]. A higher prevalence of stroke in people with DFU has also been reported [34]. Even in the case of neuropathic DFU, as opposed to ischaemic DFU, CHD is the leading cause of death [2, 3]. Numerous observational studies have demonstrated that DFU is associated with all-cause mortality, an association that persists after adjusting for confounders such as cardiovascular risk factors, pre-existing CVD and nephropathy [2, 35,36,37]. Despite these findings, few studies have investigated the mechanisms linking DFU to worse cardiovascular outcomes. Concomitant infections, such as osteomyelitis or polymicrobial growth in deep tissue, gangrene, the severity of the DFU and hindfoot location, have been previously shown to be associated with a significantly higher risk of mortality, but their impact on incident MACE has not been reported [10,11,12,13,14].
Inflammation and infection as a mediator of MACE
We hypothesise that chronic low-grade inflammation, compounded by superimposed infections, further exacerbates the systemic inflammatory response that contributes to an accelerated development and progression of CVD and HF in people with DFU. The complex interplay between inflammatory, immune and metabolic abnormalities associated with DFU and the potential implications on the risk of CVD have been highlighted previously [38]. DFU induces marked upregulation of inflammatory markers such as TNF-α, IL-6 and CRP, which correlate with ulcer severity [23,24,25]. It is well-established that inflammation promotes endothelial dysfunction, oxidative stress, atherothrombosis and atherosclerotic plaque destabilisation, leading to myocardial infarction or stroke [15]. Moreover, persistent inflammation can lead to myocardial fibrosis and cardiac remodelling, ultimately leading to HF [16]. Clinical trials of anti-inflammatory therapies support inflammation as being a driving force behind CVD; therapies such as canakinumab (a human monoclonal antibody against IL-1β) and colchicine have been shown to significantly reduce MACE in very-high-risk patients [39, 40]. Thus, it is conceivable that inflammation in the context of acute and chronic DFU plays a role in increasing cardiovascular risk over and above the inflammation that is observed in the context of diabetes.
Chronic infections in extravascular locations, such as DFU, may provide a persistent inflammatory stimulus that contributes to the overall inflammatory burden [15]. A somewhat analogous example is periodontitis, which has been shown to increase the risk of CVD [41]. Deep infection of DFU may also introduce a significant bacterial load, often polymicrobial, into the systemic circulation, leading to immune system activation and subsequent inflammation [15]. In addition, there is evidence that infecting microorganisms can directly stimulate vascular inflammation [15]. It has also been shown that acute infections, such as pneumonia, may trigger myocardial infarction, potentially due to the cytokine response causing atherosclerotic plaque rupture and/or as a result of myocardial ischaemia due to supply/demand mismatch during sepsis [42]. In the present study, it is noteworthy that CRP levels were higher in patients diagnosed with infected DFU and those who experienced MACE. Furthermore, heightened inflammation may persist even after resolution of acute infections; this has been highlighted in studies of pneumonia and may also be relevant to DFU [43]. These observations underscore the need for further research to elucidate infection-related factors in the context of DFU that potentially contribute to the heightened cardiovascular risk.
Clinical implications
The management of people with DFU is complex, necessitating attention to multiple inter-related, multi-system issues. Despite the recognised high cardiovascular risk among this population, there remains a significant gap in their cardiovascular care [44]. Our findings underscore the critical need to assess cardiovascular risk and intensively manage risk factors in patients with DFU, especially if deep infection is present. Promisingly, an observational study demonstrated that implementing an intensive cardiovascular risk factor screening programme and utilising risk-reducing therapies, such as statins, in people with DFU was associated with a reduction in five-year mortality from 48% to 27% [45]. However, there is still a need for a deeper understanding of the underlying mechanisms linking DFU and CVD. ‘Metabolic memory’ for example, can occur due to chronic hyperglycaemia, leading to epigenetic changes that may affect DFU healing, inflammation, infection risk and vascular function [46]. Given the findings of our study, it may be further postulated that anti-inflammatory approaches have a role in reducing cardiovascular risk in people with DFU. To modify chronic inflammation in the context of diabetes, strategies optimising smoking cessation, dietary modification, physical activity, weight loss and the use of statins, GLP1 agonists and SGLT2 inhibitors, may be required [26]. Whether people with DFU derive greater cardiovascular benefits from anti-inflammatory therapies, such as colchicine, requires investigation. Furthermore, ulcer duration has been associated with an increased risk of mortality [47]. Strategies that promote the resolution of inflammation, such as earlier treatment and/or therapies to accelerate wound healing, could potentially reduce cardiovascular risk but would require further studies. Timely and improved access to multidisciplinary DFU care may reduce infections and major amputations, and improve healing [31].
Limitations and strengths
Limitations of this study include its observational nature and relatively modest sample size. The sample size may have resulted in this study being underpowered to detect significant differences between groups (e.g. D−/I− vs D+/I−). Sex-disaggregated analyses were not performed due to the relatively small sample size for each ulcer depth and infection category. The results of multivariate analyses should be interpreted with caution due to the low absolute number of events. Outcome data could only be accessed from public hospital records; thus MACE and mortality rates may have been underestimated. Furthermore, the cause of death could not be ascertained for many patients, which may also have led to an underestimated rate of MACE. In addition, no specific biomarkers were available to separate inflammation from infection. We also did not have information on other factors that may impact cardiovascular risk such as lipoprotein(a) levels, physical activity levels, family history, recreational drug use, cognition and measures of vascular function [46]. As a single-centre study in a major metropolitan area, our findings may not be generalisable to other contexts with differences in care delivery. For example, SGLT2 inhibitors have prognostic benefit in people with diabetes but were less often prescribed in those with deep DFU [48]. This may reflect concerns relating to increased lower-extremity amputations based on the CANVAS trial and guideline recommendations [49, 50]. However, the current findings add to the small body of evidence examining infection of DFU and cardiovascular outcomes. Strengths of this study include the analysis of standardised data regarding wound characteristics, the presence or absence of clinical infection, and the presence or absence of comorbidities that were prospectively collected in consecutive patients for an electronic registry. Moreover, data were collected from the year 2022 onwards, reflecting contemporary practice.
Conclusion
In conclusion, deep and/or infected DFU is associated with a significantly increased risk of future cardiovascular events. This supports the concept that inflammation and infection can drive adverse atherosclerotic CVD and HF outcomes, expanding the evidence base to include patients with DFU. Given our findings, comprehensive cardiovascular risk assessment and intensive risk factor modification should be prioritised in patients with DFU, particularly when deep infections are present. Our novel findings also suggest the existence of potential mechanistic pathways that should be evaluated in future mechanistic research and larger studies.


Comments (0)