
Remember me

The data collection was conducted online from March 2022 to April 2022 using the databases of two German-based market research agencies (Dynata, https://www.dynata.com; respondi, https://www.respondi.com; last access 17.01.2024). The agencies used the database information to recruit parents of children aged 8–17 years. Participants were informed of the purpose of the data collection and the privacy policy and were requested to provide consent for the assessment of sensitive data (i.e., their children’s health information). Parents were asked if their child had a history of pTBI or a serious life-threatening medical condition. If either was confirmed, participation was discontinued. All other parents were directed to the sociodemographic questions and then asked if the child was currently available. If the child was currently unavailable, the survey could be completed later. If the child was present, they were invited to participate and, after confirming readiness to begin, the pediatric PROMs were presented. Incentives were provided to participants in the form of either tokens or certificates.
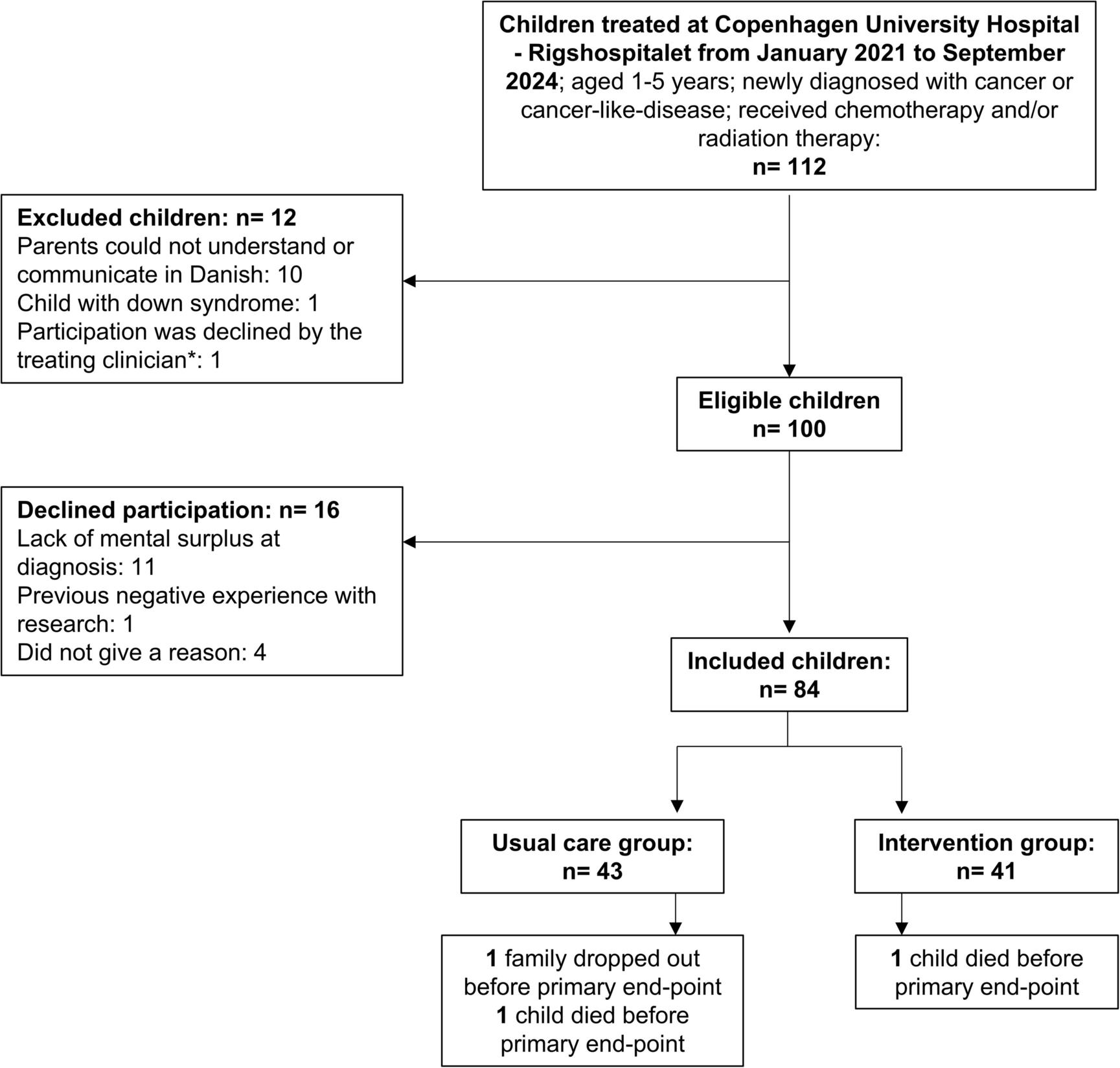
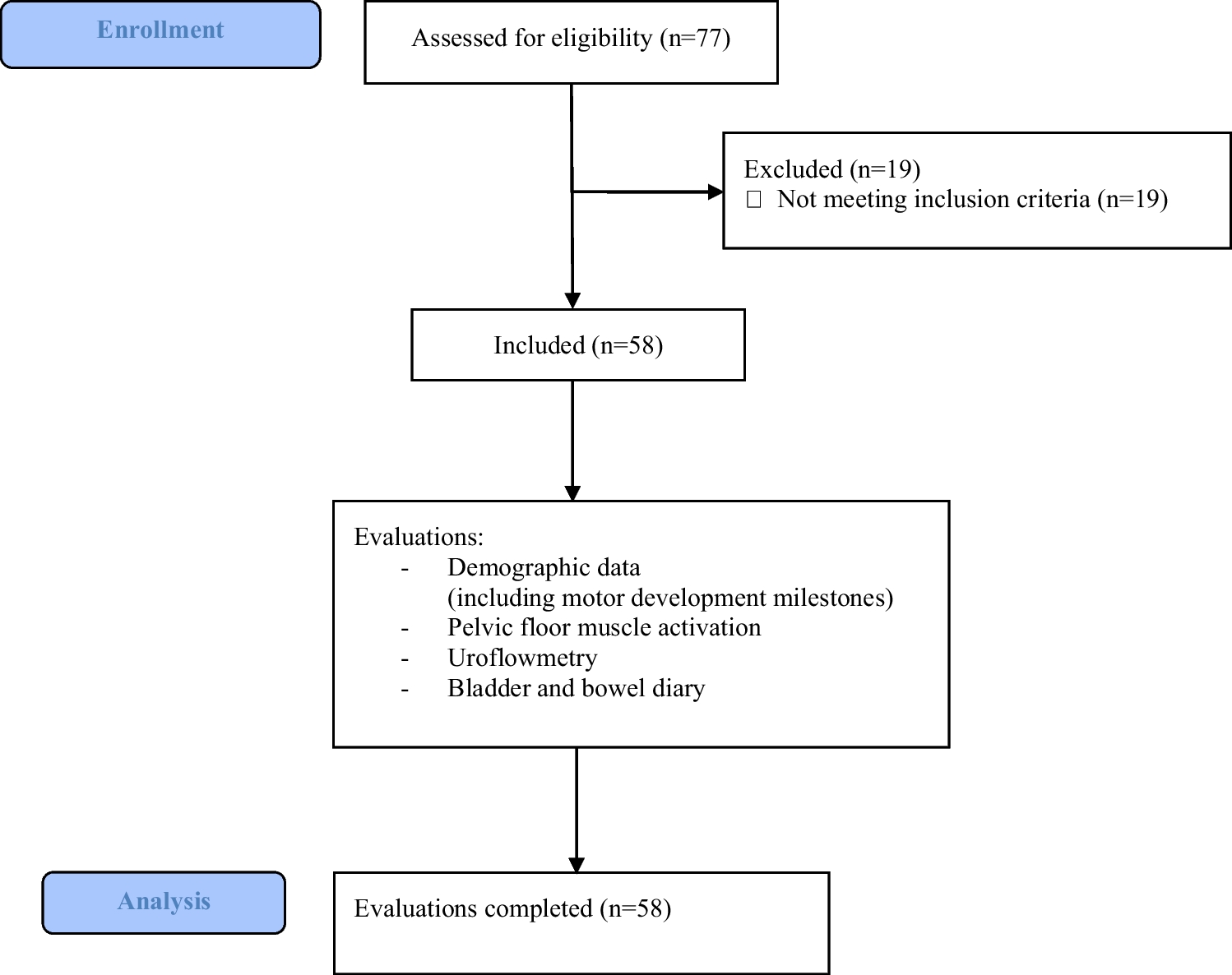
For data quality purposes, we excluded participants who provided inconsistent responses (e.g., reported no health problems but provided a description of their health status in the text box), unusable information (e.g., a comment not related to the question), and those who completed the survey in less than five minutes. As the survey did not allow missing responses, no further missing data were generated. The only exception was the question on receiving integration assistance at school, which was only asked if children and adolescents were attending any type of educational institution. A total of 950 adolescents aged 13–17 years from 2164 completed child and adolescent surveys were included in the analyses (see Fig. 1).
Fig. 1
Composition of the general population sample
For comparative analyses on construct validity, we used PCSI-SR13 data from the pTBI population assessed in the Quality of Life after Brain Injury in Children and Adolescents project, collected in Germany and Austria from January 2019 to February 2023. The questionnaire was administered in both phases of the study, the pilot and the final validation study, with post-pTBI participants completing the PCSI-SR13 pre-post form in the first phase and the post form only in the second phase. To avoid a potential effect of repeated data assessment using the same questionnaire, data from the first phase of participation was preferred for those who participated twice. Further details on the study description, inclusion and exclusion criteria, and recruitment procedures can be found elsewhere [14]. A total of N = 234 adolescents after pTBI were included in the comparative analyses (see Supplementary Figure S1).
Materials and measuresSociodemographic data (gender, age, education level) and health-related information were reported by the parents. Questions on health status allowed multiple responses in the following nine categories: central nervous system disease; alcohol and/or psychotropic substance abuse; active or uncontrolled systemic disease; psychiatric disorders; severe sensory deficits; use of psychotropic or other medications; intellectual disability or other neurobehavioral disorder; pre-, peri-, and postnatal problems; other. If there was at least one endorsement, the presence of at least one chronic health condition was assumed.
The PCSI-SR13 [11] is a 21-item self-report questionnaire for adolescents aged 13 to 18 years covering four groups of symptoms (i.e., physical, emotional, cognitive, and fatigue). The response scale is a seven-point Guttman scale with three anchor categories: 0 (not a problem), 3 (a moderate problem), and 6 (a severe problem). For the present study, the post version of the PCSI-SR13 was administered and adapted for use in the general pediatric population by omitting the reference to pTBI. The adaptation consisted only of changing the instructions, which were worded as follows: “We would like to know if you have any of these complaints at the present time (yesterday and today).”
Statistical analysesTo ensure the applicability of the PCSI-SR13 in the general population, we conducted psychometric analyses using the classical test theory framework. We examined the internal consistency of the instrument using Cronbach’s α and McDonald’s ω (values ≥ 0.70 desirable [15]), and calculated Cronbach’s α when omitting each item of the respective scale and (corrected) item-total correlations ([C]ITC; values of 0.40 or greater desirable) to further investigate the reliability.
Confirmatory factor analysis (CFA) using the diagonally weighted least square estimator for ordinal data was used to assess construct validity. Multiple goodness-of-fit indices were considered to assess model fit: \(^\)-value (p > 0.05) and \(^\)-value and degrees of freedom ratio (\(^\)/df ≤ 2) [16], comparative fit index (CFI ≥ 0.95) [17], Tucker-Lewis index (TLI ≥ 0.95) [17], root mean square error of approximation including 90% confidence interval (CI90%) (excellent to close fit: RMSEA < 0.05) [18], and standardized root mean square residual (SRMR < 0.08) [17]. Scaled values were reported for all fit indices except SRMR.
To ensure that the PCSI-SR13 measures the same construct in the general population as it does in the pTBI population, we applied a measurement invariance (MI) approach involving three steps of estimating models with increasing constraints [19, 20]. Negative binomial regression models were used to examine the potential effect of gender, age, and health status and their interactions (e.g., gender × age or gender × health status) on PCSI-SR13 total and scale scores. Significant interactions indicated the need for further stratification of the reference values. Information on these analyses is provided in the Supplemental Material.
We used percentiles to provide reference values because they are the easiest to interpret in a clinical context. A percentile is a value below which a certain relative proportion of the reference population falls. The distribution of PCSI-SR13 scores in the general population sample was divided by the following percentiles: 2.5%, 5%, 16%, 30%, 40%, 50%, 60%, 70%, 85%, 95%, and 97.5%. Values exceeding 50% (i.e., the median or also the mean of the percentile distribution) by one standard deviation, which is the 85% percentile (rounded up to the next integer) for normally distributed data, were considered clinically relevant.
Finally, we performed scale-wise comparisons of total and scale scores (Mann–Whitney U tests) between participants from the general population sample with and without chronic health conditions separately and the pTBI sample. Propensity score-matching was used to adjust for age and gender. For comparisons between the healthy general population and the pTBI sample, matching was performed using the pTBI sample as the reference. For analyses between adolescents with chronic health conditions and the pTBI sample, matching was done the other way round, using the general population sub-sample as the reference. Only male and female participants were included due to the small size of the diverse gender group. Vargha and Delaney’s effect size (A) [21] was calculated and interpreted using the following classification: group equal (0.50), small (0.35–0.44 or 0.56–0.63), medium (0.30–0.34 or 0.64–0.70), and large effect (greater than 0.29 or 0.71).
All analyses were performed with R (version 4.2.3) [22] using the packages table1 [23] for descriptive statistics, psych [24] for psychometric analyses, lavaan [25] for the CFA and the MI analyses, matchIt for sample matching [26], and effsize for sample comparisons [27]. The significance level was set at α = 5%. Where appropriate, Bonferroni correction was applied for the number of scales (α = 5%/4 = 1.25%).
Comments (0)