
Remember me

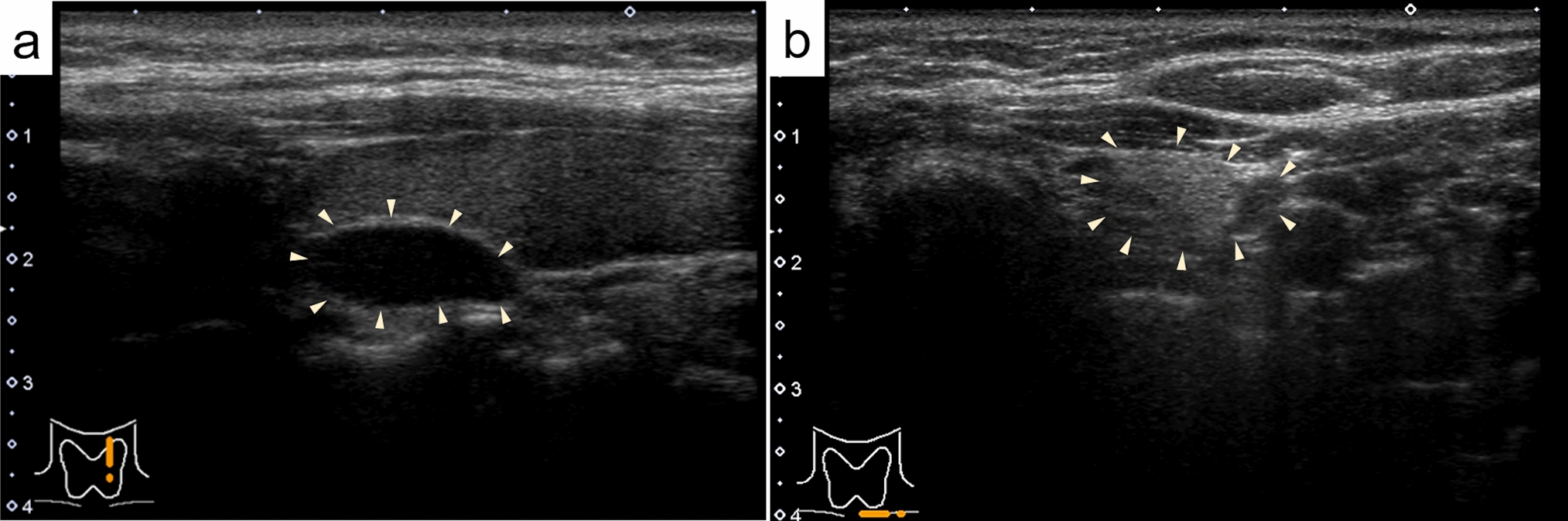
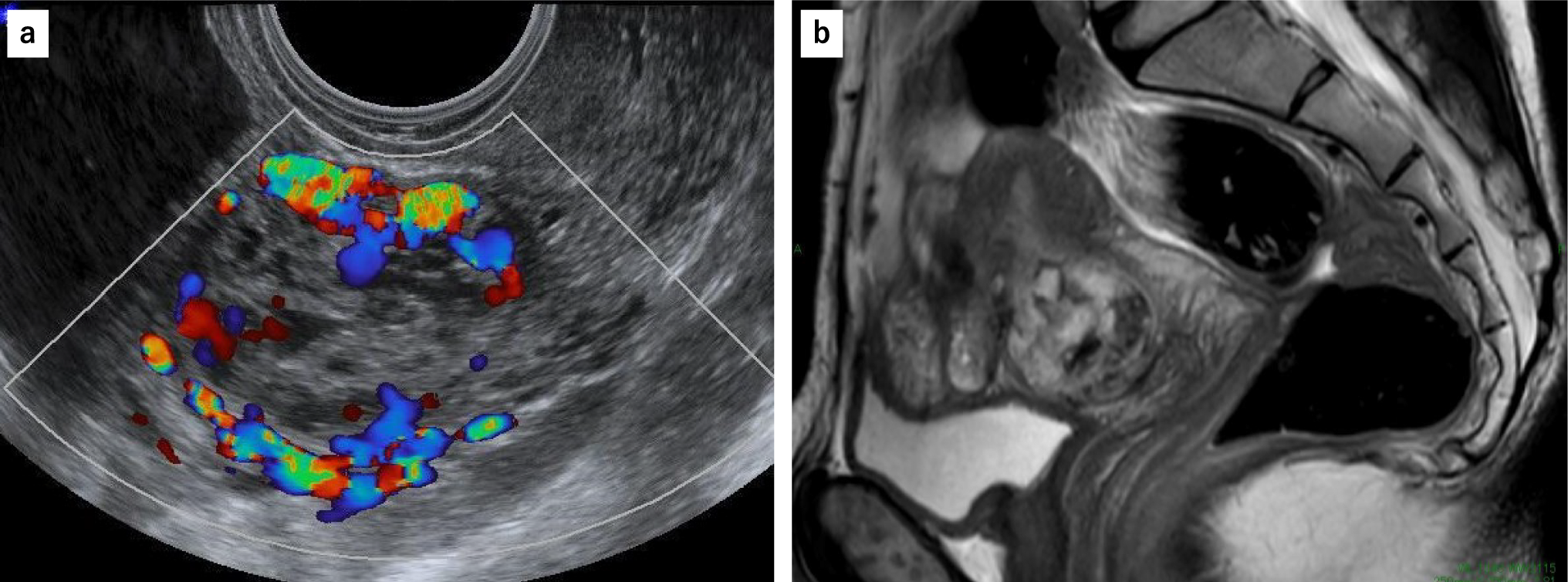

Table 1 shows the clinical findings in patients with GD and FND, with or without MPEF. The mean age of patients with GD with MPEF was 38.1 years (female/male ratio of 1.36:1) and was not significantly different from that of patients with GD without MPEF. The mean age of patients with FND with MPEF was 58.6 years, which was significantly higher than that of patients with FND without MPEF (49.9 years) (p < 0.05). The sex ratio of patients with FND with and without MPEF was not significantly different. Mean TSH levels in patients with GD with and without MPEF were 2.3 μIU/mL and 1.0 μIU/mL, respectively, which was not a significant difference. The mean serum thyroglobulin level in patients with FND with MPEF was 389.6 ng/dL, which was significantly higher than that of patients with FND without MPEF (242.9 ng/dL) (p < 0.05). Mean serum calcium levels in patients with GD and FND with MPEF were 9.1 mg/dL and 9.4 mg/dL, respectively, and no patients with hypercalcemia were found in either group.
Table 1 Clinical findings in patients with Graves’ disease or follicular nodular disease with or without multiple punctate echogenic fociUltrasonographic findingsThe thyroid volume in patients with GD with MPEF ranged between 37–441 cm3 (mean: 182.9 cm3) and tended to be larger than that of patients with GD without MPEF (mean: 142.4 cm3); however, the difference was not significant. MPEF was observed in both lobes in 21 (80.8%) patients with GD with MPEF, but it was limited to a single lobe (right lobe in two and left lobe in three) in the remaining five patients (19.2%). MPEF was diffusely distributed in 34 lobes (72.3%) (Fig. 1a) and focally distributed in the remaining 13 lobes (27.7%) (Fig. 1b).
Fig. 1
Graves’ disease. Multiple punctate echogenic foci are diffusely present (a) and densely concentrated in the lower pole (b) (B-mode ultrasonography)
Table 2 shows the ultrasonographic findings in FND cases with or without MPEF. Eighteen FND nodules with MPEF were localized in the right lobe and eight in the left lobe. MPEF was diffusely distributed in 17 nodules (65.4%) (Fig. 2a) and focally distributed in the remaining nine nodules (34.6%) (Fig. 2b). Twenty-four FND nodules with MPEF (92.3%) were solid, and their frequency was significantly higher than that of the FND nodules without MPEF (52.5%) (p < 0.01). FND nodules with MPEF showed significantly higher blood flow than those without MPEF (p < 0.05). Seven FND nodules with MPEF (26.9%) were interpreted as having intermediate suspicion, which was more frequent than that in FND nodules without MPEF (2.4%, p < 0.01). Five of these were suspected to be papillary thyroid carcinomas, and the remaining two were suspected to be follicular thyroid neoplasms. One FND nodule without MPEF, which was classified as intermediate, was suspected to be a follicular neoplasm. None of the FND cases (with or without MPEF) was highly suspicious. MPEF was not observed in non-nodular areas of the thyroid.
Table 2 Ultrasonographic findings in follicular nodular disease with or without multiple punctate echogenic fociFig. 2
Follicular nodular disease. Multiple punctate echogenic foci are diffusely present (a) and localized to the upper pole (b) (B-mode ultrasonography)
Histological findingsTable 3 shows the histological findings in GDs and FNDs with or without MPEF. CaOx crystals were observed in all GDs with MPEF, with occurrence rates of 97.9% and 93.6% for small and large crystals, respectively (Fig. 3). CaOx crystals were also observed in 71.3% of GDs without MPEF, with occurrence rates of 71.3% and 11.3% for small and large crystals, respectively. The frequency of CaOx crystals, especially that of large crystals, was significantly higher in GDs with MPEF than in those without MPEF (p < 0.00001). In the five patients with GD in whom the distribution of MPEF was limited to a single lobe, the lobe with MPEF exhibited both small and large CaOx crystals, whereas the occurrence rates of small and large CaOx crystals in the lobes without MPEF were 80.0% and 20.0%, respectively. The frequency of large CaOx crystals was significantly different between the lobes with and without MPEF (p < 0.05).
Table 3 Histological findings in Graves’ disease or follicular nodular disease with or without multiple punctate echogenic fociFig. 3
Graves’ disease. A few calcium oxalate crystals are observed in the thyroid follicles. The white bar represents 200 μm (under polarization, hematoxylin & eosin stain, 4 ×)
CaOx crystals were observed in 88.5% of FND cases with MPEF, with occurrence rates of 84.6% and 69.2% for small and large crystals, respectively (Fig. 4). CaOx crystals were observed in 48.8% of FND cases without MPEF, with occurrence rates of 48.8% and 14.6% for small and large crystals, respectively. The frequency of large crystals was significantly different between FND cases with and without MPEF (p < 0.001). Cholesterol crystals were observed in two of the three FND cases, with MPEF and no CaOx crystals.
Fig. 4
Follicular nodular disease. Mixed small and large calcium oxalate crystals are observed in the thyroid follicles. The white bar represents 200 μm (under polarization, hematoxylin & eosin stain, 4 ×)
Cystic changes were also observed in 30.8% of the FNDs with MPEF, but such changes were significantly less frequent than those in the FNDs without MPEF (56.1%) (p < 0.05). Cholesterol crystals and lymphocytic infiltration were found in 6.4% and 63.8% of GDs with MPEF, and 15.4% and 3.8% of FNDs with MPEF, respectively, with no significant difference when compared with the respective control. No psammoma bodies were observed in either GDs or FNDs.
Comments (0)