
記住我




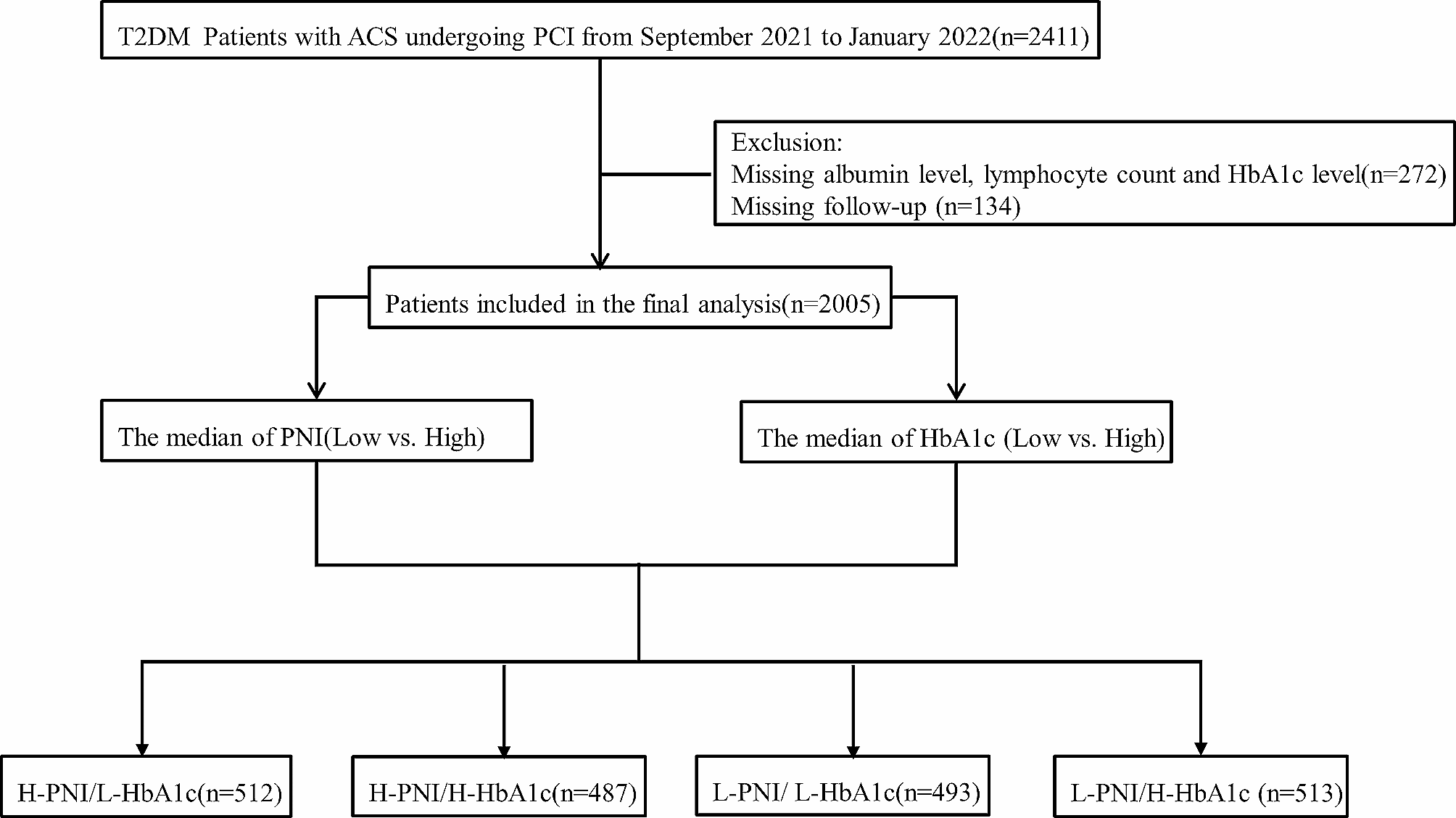

A retrospective cohort analysis encompassing 2,411 patients diagnosed with T2DM and ACS who underwent PCI between September 2021 and January 2022 was performed at Beijing Anzhen Hospital. The Electronic Medical Records System of Beijing Anzhen Hospital provided the baseline information at the time of admission. T2DM was defined as the use of oral antidiabetic drugs or insulin or the self-reporting of diabetes [10]. The existing guidelines classified ACS as either unstable angina pectoris (UAP), ST-segment elevation myocardial infarction (STEMI), or non-ST-segment elevation myocardial infarction (NSTEMI) [11]. The PCI was conducted following the standard clinical procedure [12, 13]. Study participants met the following inclusion criteria: (1) at least one clinical phenotype of ACS-UAP, NSTEMI, or STEMI; (2) diagnosis of T2DM; (3) undergoing PCI at Beijing Anzhen Hospital; and (4) complete medical records available, including data on serum albumin (Alb) levels, total lymphocyte counts (TLCs), and HbA1c levels. The exclusion criteria included age under 18 years, PCI failure, chronic liver or renal failure, infectious diseases, taking some drugs that may influence the levels of Alb, and TLCs, and missing clinical data including Alb, TLCs, and HbA1c levels. Patients without measurements of Alb levels, TLCs, or HbA1c levels (n = 272) and those who were missing follow-up data (n = 134) were excluded. Ultimately, the study included 2,005 patients (Fig. 1). All participants in the study provided their informed consent.
Fig. 1
The flowchart of participant selection
Laboratory data collectionAfter the patients fasted through the night, their blood samples were collected in the morning and examined in the central laboratory that same day using routine laboratory techniques. An automated blood cell counter was used to count the blood cells. An automatic biochemistry analyzer (Hitachi 7150, Tokyo, Japan) was used to quantify Alb, triglycerides (TG), total cholesterol (TC), low-density lipoprotein cholesterol(LDL-C), high-density lipoprotein cholesterol (HDL-C), uric acid (UA), glucose, creatinine (CR), and the estimated glomerular filtration rate (eGFR). High-performance liquid chromatography was used to measure HbA1c levels (BioRad Variant II TURBO HbA1c analyzer, USA).
Malnutrition and glycemic control assessmentThe PNI was selected as an assessment for malnutrition, and the HbA1c level was used to measure poor glycemic control. The PNI = Alb (g/L) + 5×TLCs (×109/L) [6]. The median PNI and HbA1c levels were 52.9 and 7.0%, respectively. Based on median PNI and HbA1c levels, we divided the patients into four groups: high (H)-PNI/low (L)-HbA1c, H-PNI/H-HbA1c, L-PNI/L-HbA1c, and L-PNI/H-HbA1c.
Definition of CVD risk factorsEach CVD risk factor and health condition was defined based on well-established criteria. A current smoker was defined as someone who smokes seven cigarettes or more every week for at least 6 months [14]. The 2018 Chinese Heart Failure Guidelines defined heart failure (HF) as New York Heart Association class ≥ III [15]. Chronic kidney disease (CKD) is defined as eGFR of less than 60 mL/min/1.73 m2 [16]. The definition of hypertension included self-reported hypertension, and antihypertensive drug usage [17]. To meet the definition of hyperlipidemia, patients had to satisfy at least one of the following criteria: usage of medication to lower lipids or a self-reported record of dyslipidemia [18]. Coronary angiogram characteristics were visually measured and analyzed by a minimum of two experienced cardiologists.
Endpoints and follow-upMajor adverse cardiac and cerebrovascular events (MACCE) were the primary outcome. All-cause mortality was deemed cardiac if there was no clear noncardiac cause. The identification of MI was conducted in adherence to the Fourth Universal Definition of Myocardial Infarction. The classification of stroke encompassed both ischemic and hemorrhagic stroke. The termination of the follow-up period is contingent upon the earliest occurrence of MACCE, loss of follow-up, or the date of March 10, 2023.
Statistical analysisContinuous variables are commonly reported as medians with interquartile ranges or mean values with standard deviations. Categorical variables are commonly expressed as percentages and frequencies. To identify potential disparities among subgroups, statistical tests, such as chi-square and analysis of variance, were employed.
Kaplan–Meier curves were used to examine the likelihood of survival between the groups through log-rank tests. By using Cox proportional hazard models, the hazard ratio (HR) was computed. Variables were chosen based on their established connections with poor prognosis, as determined using a univariate Cox regression analysis. Model 1 remained alone without any modifications. Model 2 was calibrated for age, sex, body mass index (BMI), and current smoking status. Adjusting for the variables obtained from Model 2 and recognized risk factors, including hypertension, hyperlipidemia, prior MI, HF, CKD, and ACS type, was modified in Model 3. Model 4 was altered to include the variables from Model 3, along with TG, TC, and LDL-C levels.
To examine whether adding the PNI to Model 5 (the variables in Model 4 plus HbA1c levels) would improve accuracy in predicting poor outcomes, the concordance index (C-index), net reclassification improvement (NRI), and integrated discrimination improvement (IDI) were collected. In Model 5, we conducted an additional investigation into the relationship between the PNI and poor outcomes using restricted cubic splines.
R software version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria) was used to perform the statistical analysis. It was determined that the data was significant by using P < 0.05.
留言 (0)