
Remember me





A total of 297 patients with SLADC were initially screened for inclusion, of which 41 were excluded because of a history of antitumor therapy before the chest CT scan and 28 owing to poor imaging quality. Finally, 228 patients with SLADC were included for analysis. The patient selection flowchart is shown in Fig. 1. Among the 228 patients, 66 (28.9%) were classified as type I (mean age: 61.64 ± 7.75 [range: 42–80] years; 34 males and 32 females; 45 smokers and 21 nonsmokers), 123 (53.9%) as type II (mean age: 59.27 ± 10.47 [range: 30–81] years; 50 males and 73 females; 39 smokers and 84 nonsmokers), 16 (7%) as type III (mean age: 58.75 ± 6.93 [range: 49–72] years; 11 males and 5 females; 8 smokers and 8 nonsmokers), and 23 (10.1%) as type IV (mean age: 65.21 ± 8.39 [range: 50–83] years; 5 males and 18 females; 10 smokers and 13 nonsmokers) (Table 2). The diagnostic methods included surgical resection, fiberoptic bronchoscopy, puncture biopsy, and cytology, with surgical resection being the most employed method (n = 202/228; 88.6%). A total of 134 patients had undergone two follow-up CT scans, 61 had undergone three follow-up CT scans, 21 had undergone four follow-up CT scans, 7 had undergone five follow-up CT scans, 4 had undergone six follow-up CT scans, and 1 patient had undergone eight follow-up CT scans. The mean tumor size was 24.37 ± 9.29 mm in the initial CT scan and 29.43 ± 12.1 mm in the last CT scan.
Fig. 1
Selection flowchart for this study
Table 2 Baseline characteristics of patientsObserver reproducibilityThe agreement between the two radiologists was pretty good for all CT features (Supplementary Table 1). The ICC values for CT features of type I tumors ranged from 0.898 to 1.000; those for CT features of type II tumors ranged from 0.899 to 1.000; those for CT features of type III tumors ranged from 0.828 to 1.000; and those for CT features of type IV tumors ranged from 0.904 to 1.000 (all p < 0.001).
Imaging evolution and VDT of different SLADC typesIn type I tumors, the tumor diameter enlarged over time, i.e., lobulation, spiculation, air bronchogram sign, pleural retraction, vessel convergence sign, lymphadenopathy, and pleural effusion gradually appeared in the tumor (Fig. 2a). Most of the type II tumors (n = 96/123; 78.0%) enlarged over time with increased density or solid components, whereas the remaining tumors [n = 27/123; 22.0%] were fluctuating between regression and enlargement, with increasing density or solid components (Fig. 2b). Additionally, lobulation, spiculation, and the air bronchogram sign also gradually appeared in these tumors. For type III, the diameter of cystic airspace enlarged over time—cystic walls thickened, and wall nodules appeared; eventually, the cystic airspace narrowed or disappeared and the tumor became a solid mass (observed in two patients) (Fig. 2c). In type IV SLADC, the tumor enlarged over time—the attenuation increased while the air bronchogram sign, air space, and GGO component gradually disappeared, and the lesion ultimately became a solid mass (Fig. 2d).
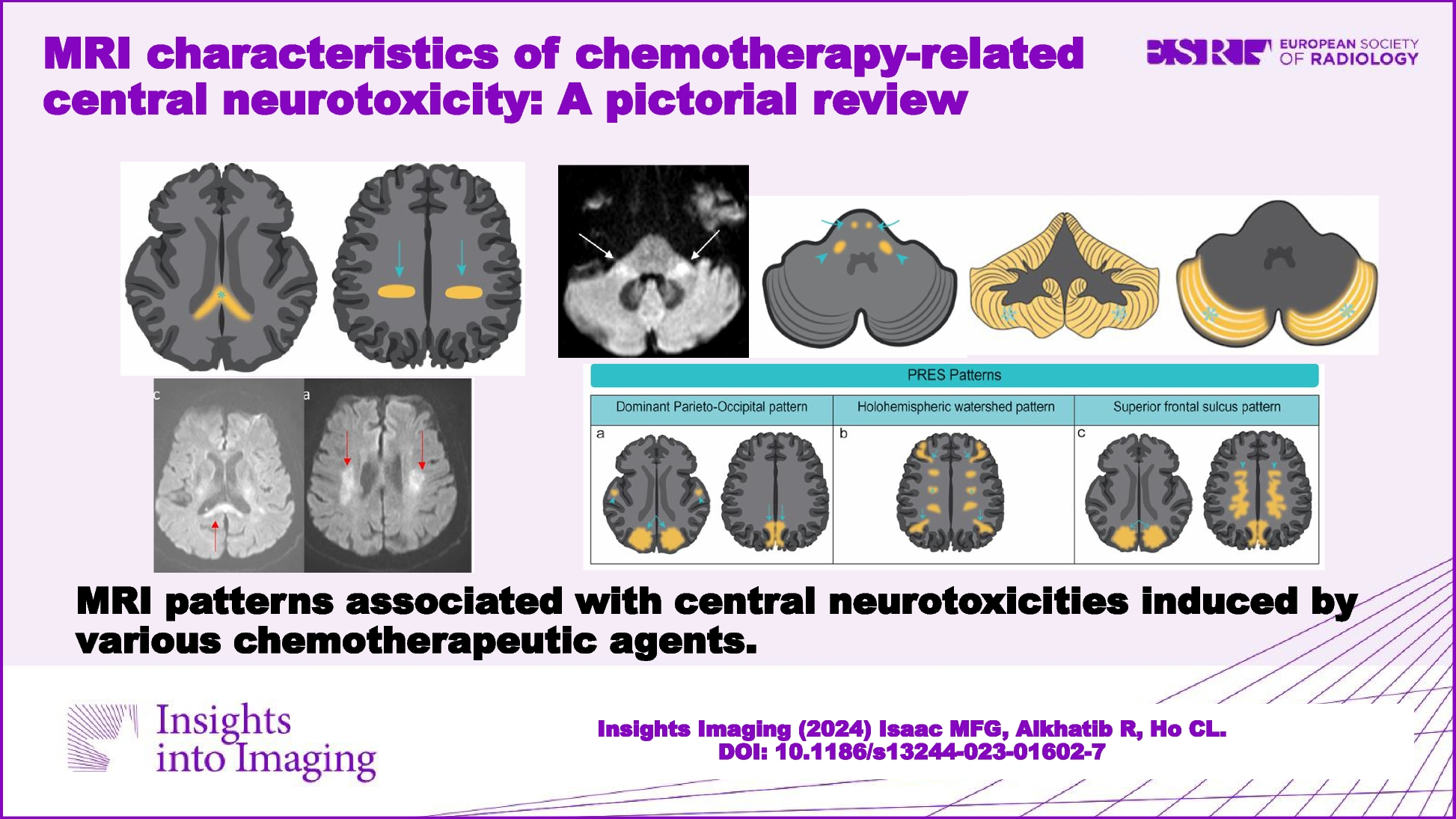
Fig. 2
Axial CT images show the evolution of type I-IV SLADCs during follow-ups. a Sequential images in a 47-year-old woman who had LADC show that the tumor enlarged over time with lobulation, spiculation, and pleural retraction appeared. b Sequential images in a 60-year-old woman who had LADC show that the tumor was stable firstly, then decreased with solid components and density increased, and then increased again. c Sequential images in a 65-year-old man who had LADC show that the cystic airspace enlarged, cystic walls thickened, and wall nodules appeared. d Sequential images in a 58-year-old woman who had LADC show that a focal consolidation enlarged over time, with attenuation increased as well as air bronchogram and GGO component gradually disappeared, and eventually became a solid mass
We observed good inter- and intra-observer reliability for tumor volume measurement (ICCs = 0.880 and 0.921, respectively). The median VDT was 601 (IQR = 975) days (range = 45–2750 days) for all patients. Type I tumors had the shortest median VDT (254 [IQR = 201] days; range = 45–1966 days), followed by type IV (median = 381 [IQR = 590] days; range = 60–2056 days), type III (median = 501 [IQR = 777] days; range = 95–2113 days), and type II (median = 993 [IQR = 812] days; range = 112–2750 days). The VDT for type I was shorter than all other tumor types (p < 0.05 each); furthermore, the VDT for types III and IV was shorter than that for type II (i.e., I < IV/III < II) (p < 0.05 each). However, no statistically significant difference was observed between the VDT for types III and IV (p > 0.05).
Correlation between histological subtypes and morphological classification of SLADCOf all patients, histological classification was available for 202 patients who underwent surgical resection. As shown in Figs. 3 and 4 and Table 3, type I tumors had a greater proportion of the solid/micropapillary-predominant pattern as compared to type II, whereas the lepidic-predominant pattern was more dominant in types II and III than in type I (p < 0.05 each). However, there were no significant differences in the proportion of acinar-predominant and papillary-predominant patterns among all types (p > 0.05 each).
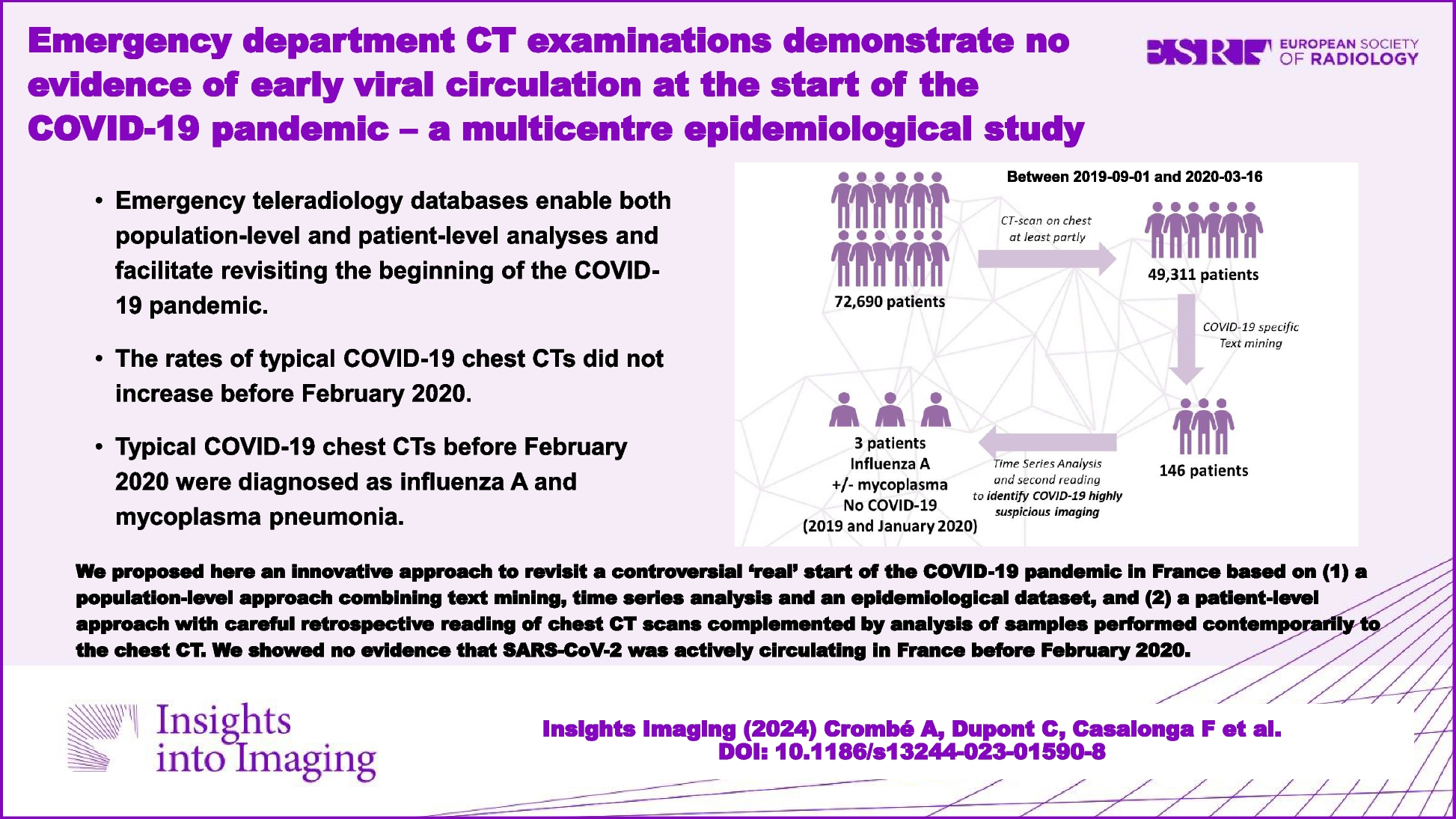
Fig. 3
The histological subtypes of SLADC and their correlation with morphological classifications. a R-SLADC in a 59-year-old man with type I. a-1 Axial CT images of lung window indicate a solid mass with evident lobulation and spiculation. a-2 Photomicrograph (H&E staining, × 200) confirmed SLADC with a solid-predominant growth pattern. b R-SLADC in a 63-year-old man with type I. b-1 Axial CT images of the lung window indicate a solid mass with evident air space and pleural attachment. b-2 Photomicrograph (H&E staining, × 200) confirmed SLADC with a micropapillary-predominant growth pattern. c R-SLADC in a 76-year-old woman with type II. c-1 Axial CT images of the lung window indicate a subsolid mass with evident pleural attachment. c-2 Photomicrograph (H&E staining, × 200) confirmed SLADC with a lepidic-predominant growth pattern. d L-SLADC in a 55-year-old man with type III. d-1 Axial CT images of the lung window indicate a cystic airspace attached to the mediastinum. d-2 Photomicrograph (H&E staining, × 200) confirmed SLADC with a papillary-predominant growth pattern. e L-SLADC in a 67-year-old woman with type IV. e-1 Axial CT images of the lung window indicate a focal consolidation with evident GGO component and air bronchogram sign. e-2 Photomicrograph (H&E staining, × 200) confirmed SLADC with an acinar-predominant growth pattern
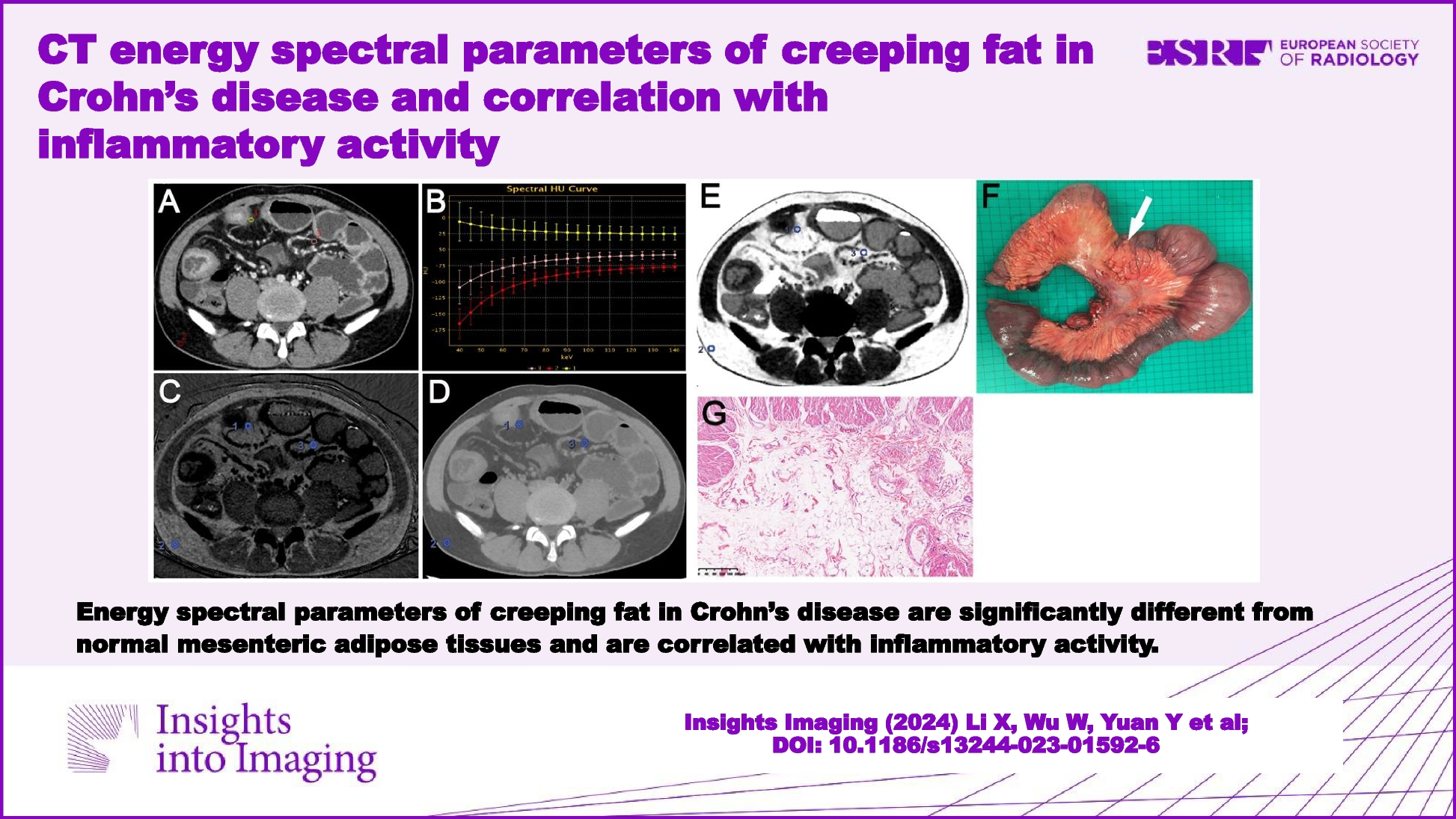
Fig. 4
Distribution histogram of type I–IV SLADCs in different histological subtypes
Table 3 Correlation between histological subtypes and morphological classification of SLADCCorrelation between gene mutation status and morphological classification of SLADCThe genetic mutation tests of EGFR, ALK, and KRAS were available for 36, 28, and 28 patients, respectively. Among them, 17 patients (n = 17/36; 47.2%) were positive for EGFR mutation, 1 patient (n = 1/28; 3.6%) tested positive for ALK mutation, and 7 patients (n = 7/28; 25%) tested positive for KRAS mutation. As shown in Table 4, types II and IV SLADCs were found to be correlated to EGFR mutation status, i.e., EGFR mutation rates were significantly higher in patients with types II and IV SLADCs than in those without (p < 0.05 each). However, no significant differences were observed in terms of ALK or KRAS mutation rates among the four tumor subtypes (p > 0.05 each).
Table 4 Correlation between gene mutation status and morphological classification of SLADCSurvival analysis of patients with SLADCFollow-up information was available for 126 of the SLADC patients undergoing surgical resection; among them, 29 patients (23%) experienced disease recurrence, and 14 patients (11.1%) died. Overall, the median DFS was 33 months; individually, the median DFS time for each tumor subtype was as follows: type I = 29 months, type II = 47 months, type III = 37 months, and type IV = 36 months. We found that the CT morphological classification was correlated with the DFS of patients. The Kaplan–Meier curves displayed those patients with type II SLADC had the longest DFS, followed by patients with types III and IV, and then patients with type I (i.e., II > III/IV > I) (p < 0.001 each) (Fig. 5). Among the 9 patients with type III tumors whose follow-up information was complete for survival analysis, their DFS correlated negatively with the thickness of cystic walls before operation (r = − 0.69, p < 0.05).
Fig. 5
Survival analysis of patients with type I–IV SLADCs
Comments (0)