
記住我
Dear Editor,
Sexually transmitted infections (STIs) constitute a challenging health problem among youngsters.1 According to the World Health Organization (WHO), 20% of persons living with HIV/AIDS are in their 20s. Only a few studies have assessed the level of knowledge about STIs among adolescents.2,3
We did a cross-sectional study among 8th, 9th and 10th standard students attending various public and private schools in an educational sub-district in Thrissur, Kerala, with the objective of estimating the level of knowledge about STIs among high school students and their relationship with various socio-demographic parameters after obtaining ethics clearance.
One school each belonging to government, government aided, private and CBSE boards was chosen by the lottery method. Study participants were chosen using multistage stratified random sampling. Divisions from each grade were again chosen by the lottery method. Sample size was calculated based on the proportion of poor knowledge of STI (19.1%) obtained from the previous study and with 95% confidence and 20% allowable error.2 Sample size obtained was 510. A total of 526 students were recruited over a period of 1 year.
A self-administered questionnaire, prepared by us based on a reference questionnaire, was used as the study tool. Some selected questions from the reference questionnaire were used and few additional questions were added with the help of experts. For the pilot study, we used 50 samples but 10 samples were lost to follow-up. Cronbach’s alpha was used to check the reliability of the questionnaire. It showed an alpha value of 0.821 (good internal consistency). Test–retest reliability was assessed every 2 weeks using the Spearman rank correlation coefficient (0.968, a high correlation).
The questionnaire had 9 questions and questions 6, 7, 8 and 9 were given a score of 2 for each correct answer and 1 for each wrong answer. Total score of 36 was divided into 3 parts and a score less than 12 was considered to be poor, a score between 12 and 24 was considered fair and a score more than 24 was considered good knowledge. Because the frequency of students having good knowledge was low, we combined fair and good knowledge into one category for further analysis. Thus, those who scored 12 or less were considered as having poor knowledge and those who scored more than 12 as having good knowledge.
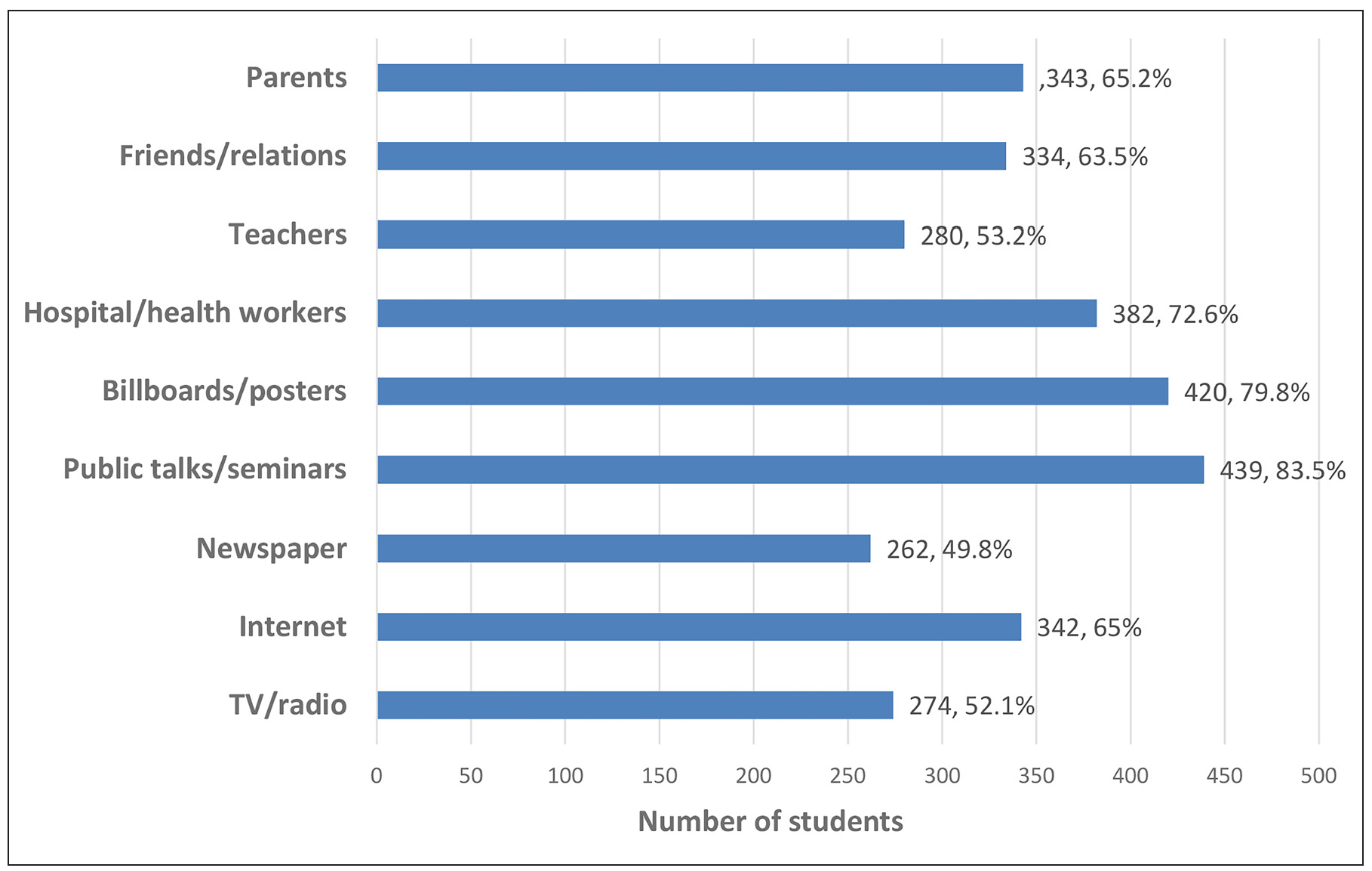
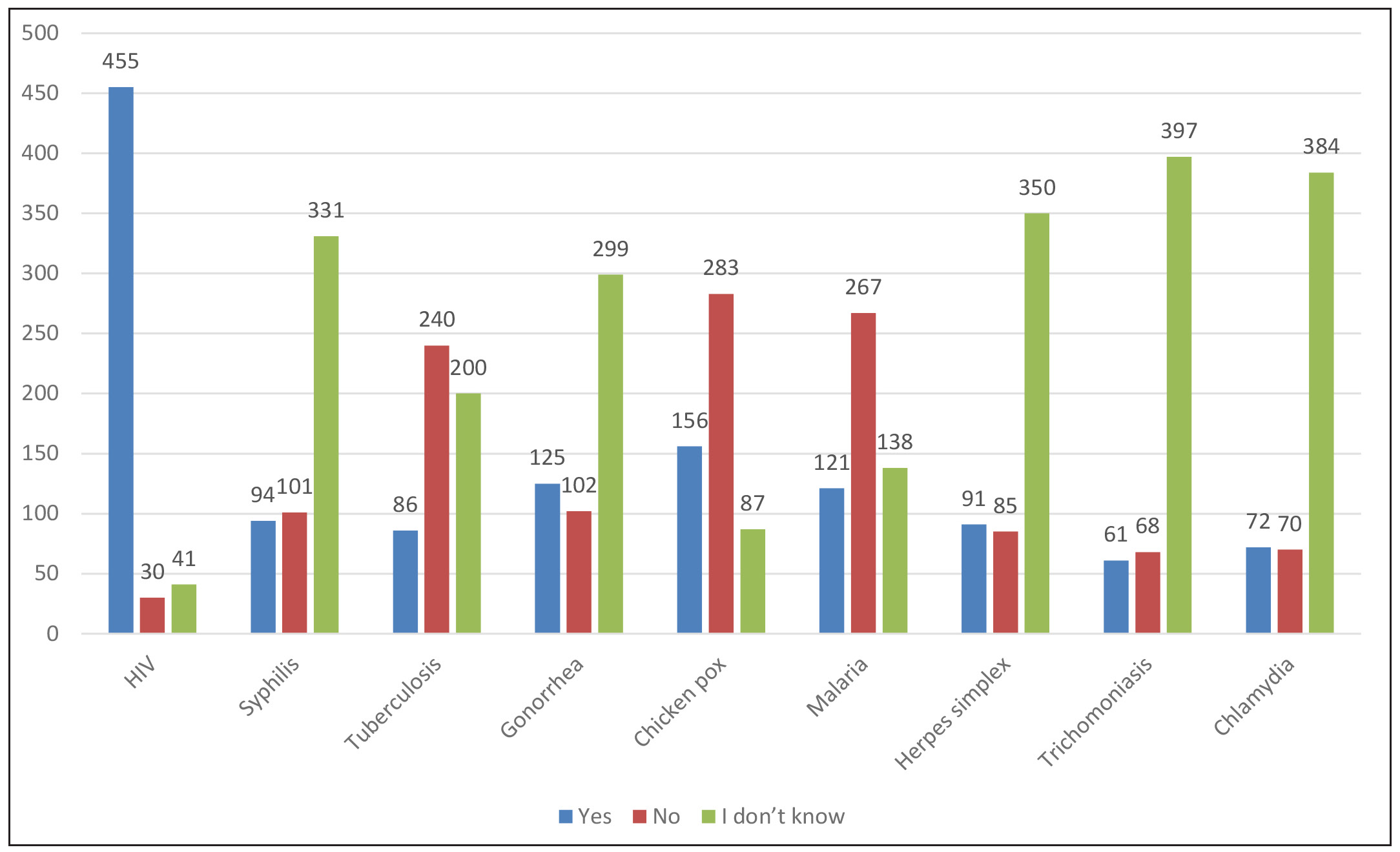
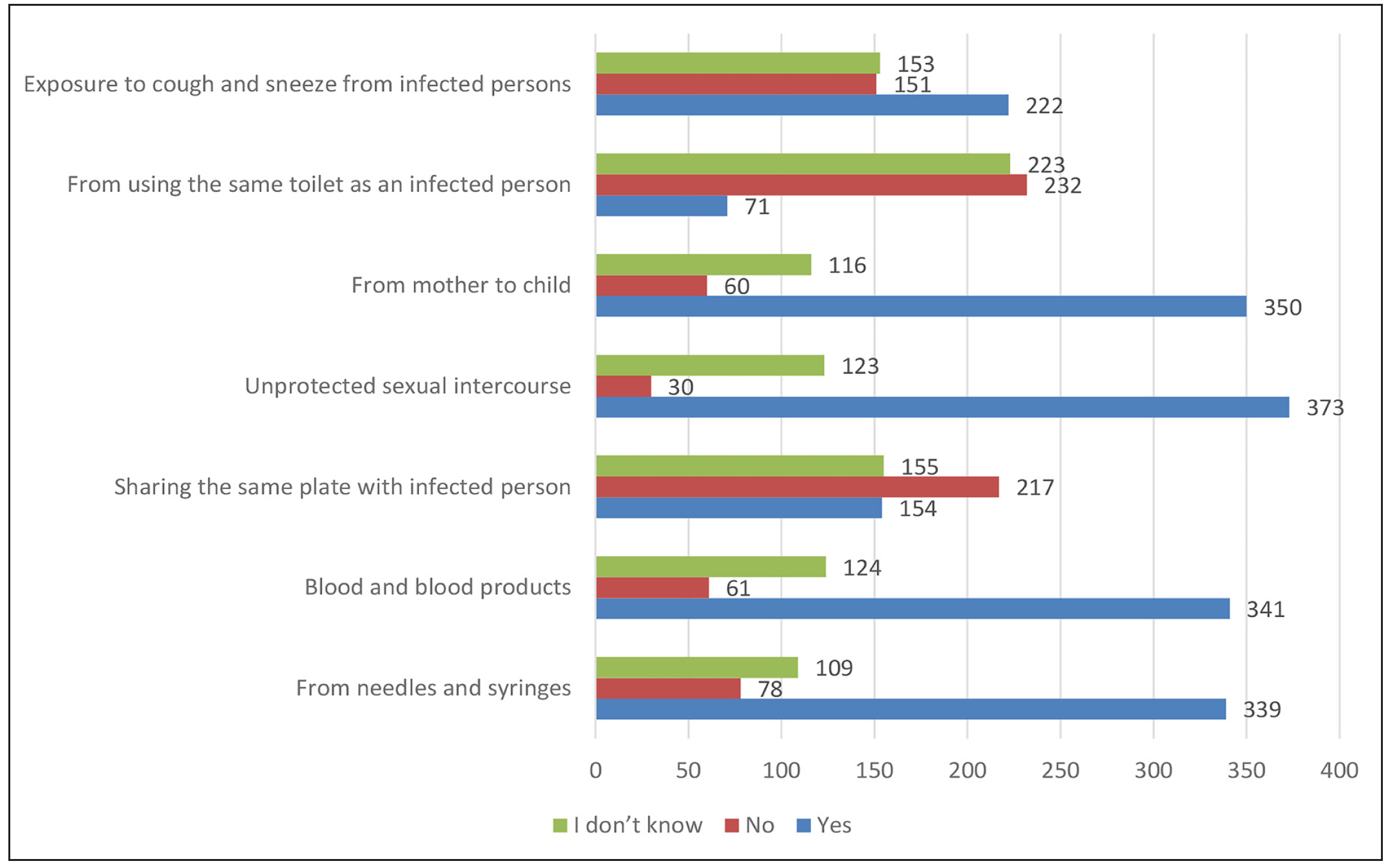
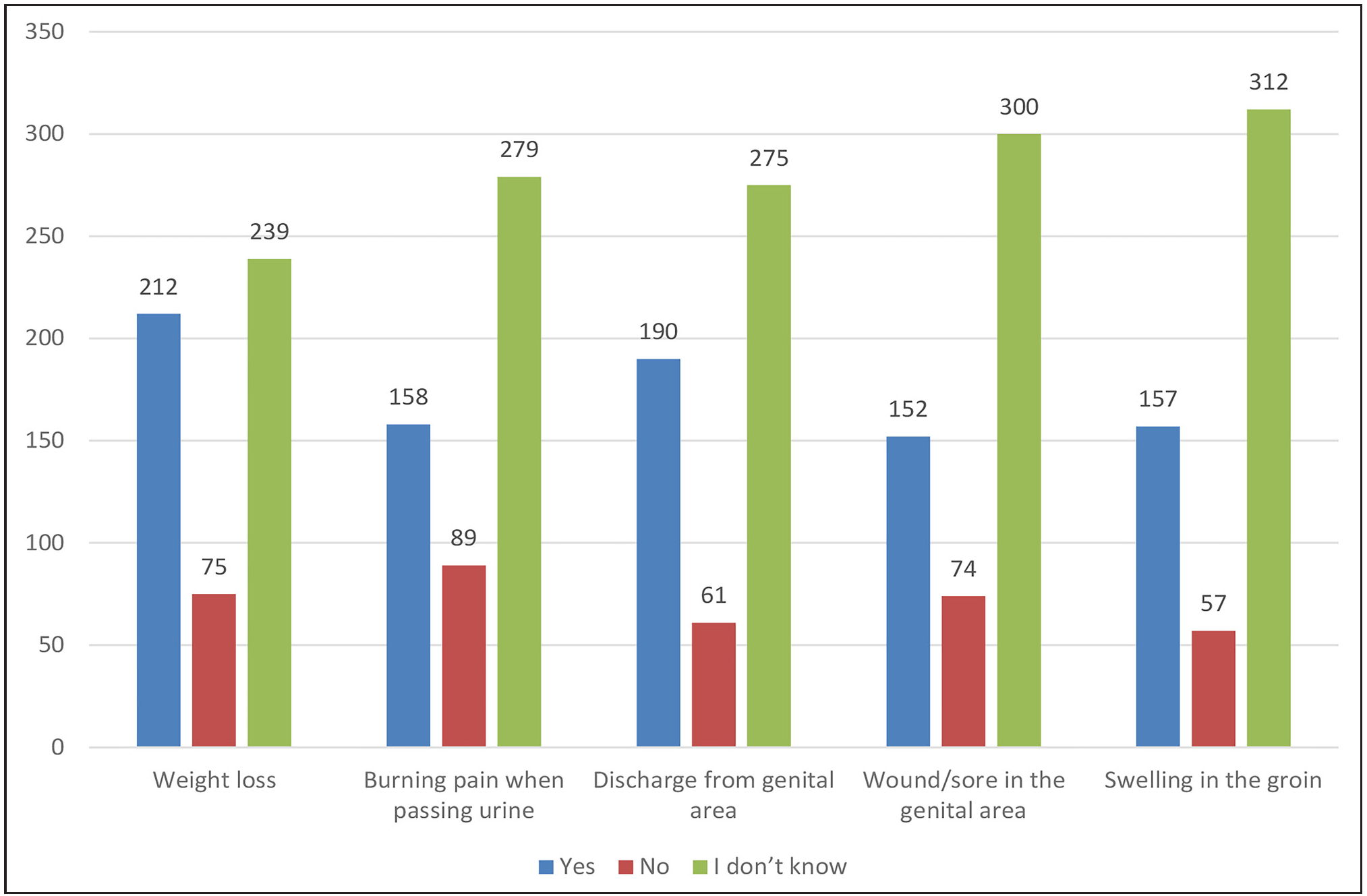
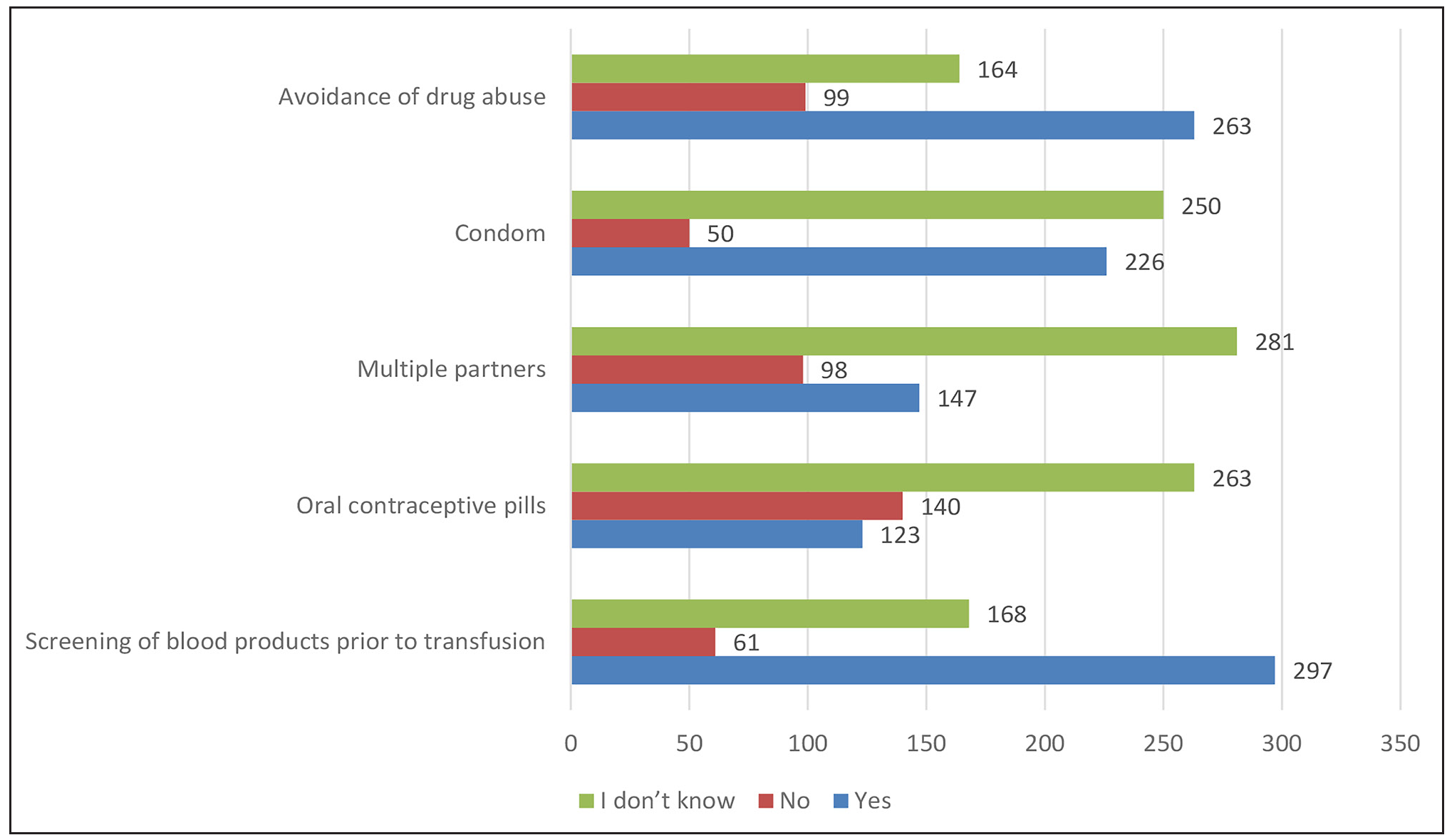
The distribution of our study participants is depicted in Figure 1. The age of the students ranged from 12 to 18 years (mean=15±2.16). Boys outnumbered girls (M:F = 1.4:1). Public talks [439, (83.5%)], posters [420, (79.8%)] and hospital and health workers [382, (72.6%)] were identified to be the common sources of information regarding STIs [Figure 2]. Majority [(n=455(86.5%)] of the students identified HIV/AIDS as an STI [Figure 3]. However, only less than 25% of students were aware of the other STIs like syphilis, gonorrhoea, herpes simplex infections, trichomoniasis and chlamydia. We observed notable misconceptions among students that STI can be transmitted by coughing/sneezing [n = 222(42.2.0%)], sharing of toilets [n = 71 (13.5%)] and sharing of plates [n = 154 (29.3%)] [Figure 4]. Majority of the respondents could not identify the common symptoms of STIs such as weight loss (n= 212, 40.3%), genital discharge (190, 36.1%) and painful micturition (n=158, 30%) [Figure 5]. Only less than 30% of the respondents could identify genital sore and swelling of the groin which are very common symptoms of STIs. Screening of blood and blood products [297 (56.5%)], avoidance of drug abuse [263 (50%)] and use of condoms [226 (43%)] were rightly identified as methods of prevention of transmission of STIs [Figure 6].

Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
A total of 313 (59.5%) students had poor knowledge and 213 (40.5%) had good knowledge of STIs [Table 1]. The factors identified as significant predictors of knowledge regarding STI on univariate analysis were higher age, male gender, CBSE school, higher grade class, parents with higher level of education and acquisition of knowledge from the Internet and health workers [Table 2]. In multivariate analysis, 10th grade class, unaided schools, aided schools, usage of the Internet and health workers were the significant independent factors to influence the level of knowledge [Table 3].
Table 1: Level of knowledge of students from different types of schools about sexually transmitted infections
Level of Knowledge of STISchool type Poor Good Total Chi-square test p-value Government school 45 (51.1%) 43 (48.9%) 88 (100%) Unaided school 46 (64.8%) 25 (35.2%) 71 (100%) CBSE school 90 (48.1%) 97 (51.9%) 187 (100%) 27.709 0.001* Aided school 132 (73.3%) 48 (26.7%) 180 (100%) Total 313 (59.5%) 213 (40.5%) 526 (100%)Table 2: Univariate analysis
Variables Category # Level of Knowledge of STI OR (95% CI of OR) p-value Poor No. (%) Good No. (%) Age <14 316 225 (71.2%) 91 (28.8%) 1 <0.001* >14 210 88 (41.9%) 122 (58.1%) 3.428 (2.376 – 4.946) Class 8th 169 124 (73.4%) 45 (26.6%) 1 0.368 9th 164 113 (68.9%) 51 (31.1%) 1.244 (0.773 -2.00) 10th 193 76 (39.4%) 117 (60.6%) 4.242 (2.713-6.632) <0.001 Sex Female 222 143 (64.4%) 79 (35.6%) 1 0.050 Male 304 170 (55.9%) 134 (44.1%) 1.427 (0.999-2.037) Educational status of mother < Graduate 282 184 (65.2%) 98 (34.8%) 1 0.019 >Graduate 234 129 (55.1%) 105 (44.95) 1.528 (1.071 – 2.181) Education of Father < Graduate 264 170 (64.4%) 94 (35.6%) 1 0.022 >Graduate 262 143 (54.6%) 119 (45.4%) 1.505 (1.06–2.136) Occupation of mother Nil 253 139 (54.9%) 114 (45.1%) 1 0.040 Job 273 174 (63.7%) 99 (36.3%) 0.694 (0.489–0.984) Occupation of father Government job 72 45 (62.5%) 27 (37.5%) 1 0.572 Non-govt. job 451 266 (59.0%) 185 (41.0%) 1.159 (0.694–1.936) Income <20000 175 114 (65.1%) 61 (34.9%) 1 0.047 >20000 346 194 (56.1%) 152 (43.9%) 1.464 (1.005-2.134) School CBSE school 187 90 (48.1%) 97 (51.9%) 1 0.642 Govt. school 88 45 (51.1%) 43 (48.9%) 0.887 (0.534 – 1.472) Unaided school 71 46 (64.8%) 25 (35.2%) 0.504 (0.287–0.887) 0.017 Aided school 180 132 (73.3%) 48 (26.7%) 0.337 (0.218 – 0.523) <0.001 Internet No 184 85 (46.2%) 99 (53.8%) 1 <0.001 Yes 342 228 (66.7%) 114 (33.3%) 0.429 (0.297 – 0.620) Television No 252 150 (59.5%) 102 (40.5%) 1 1.000 Yes 274 163 (59.5%) 111 (40.5%) 0.999 (0.705 – 1.415) Health worker No 144 75 (52.1%) 69 (47.9%) 1 0.033 Yes 382 238 (62.3%) 144 (37.7%) 0.658 (0.447–0.968)Table 3: Multivariate analysis
Variable Category Adjusted Odds Ratio 95% Confidence Interval p-value Lower bound Upper bound Age <14 year 1 0.698 >14 year 1.072 0.889 2.074 Sex Female 1 0.081 Male 0.623 0.413 1.189 Class 8th 1 0.107 9th 0.244 0.110 0.539 10th 1.356 1.024 2.532 0.036 Educational status of mother <Graduate 1 0.231 >Graduate 1.026 0.891 1.786 Education of father <Graduate 1 0.095 >Graduate 1.32 0.945 2.104 Occupation of mother Nil 1 0.102 Job 0.786 0.453 1.132 Income <20000 1 0.112 >20000 0.526 0.213 1.243 School CBSE school 1 0.356 Govt. school 0.902 0.634 1.621 Unaided school 0.625 0.327 0.912 0.031 Aided school 0.462 0.118 0.632 0.012 Internet No 1 0.045 Yes 0.694 0.235 0.876 Health worker No 1 0.023 Yes 0.732 0.564 0.842The common sources of information regarding STIs for the students were public talks, posters, hospital and health workers as compared to the Internet, teachers, TV and newspapers. This clearly points out that, despite the widespread use of social media among the current generation, there is a dearth of information on STIs in these media. Studies from Nigeria and Uganda have reported radio/television, newspapers and magazines as important sources of information about STIs.4 In our study, only less than 25 % of students were aware of the other STIs like syphilis, gonorrhoea, herpes simplex infections, trichomoniasis and chlamydia. This is probably due to lack of awareness campaigns about STIs other than HIV/AIDS in schools. Nguyen et al. also had a similar observation.5 Significant misconceptions existed regarding mode of STIs transmission, similar to the results of the Nigerian study.2 Another interesting finding of our study was the lack of awareness of the participants regarding the clinical presentations of STIs. Our results were comparable to another previous study from South India.3 Respondents correctly identified screening of blood and blood products, avoidance of drug abuse and usage of condoms as methods of prevention of transmission of STIs. This indicates that the students are reasonably well informed about the commoner modes of spread and prevention.
Older students had better knowledge about STIs. The level of knowledge about STIs varied with the type of school with CBSE students having a statistically significant higher level of knowledge. This could possibly be explained by the sex education classes that they had been exposed to prior to our survey. Boys had a higher level of knowledge as compared to girls (44.1% vs 35.6%) probably due to their increased access to various portals of information.
Following are some of the recommendations that could be made to improve the knowledge about STIs among school students:
Seminars and public talks should be conducted regularly in schools about STIs and their prevention.
The link between non-HIV STIs and HIV/AIDS should be emphasised. The fact that STIs increase the likelihood of HIV transmission may increase the concern about STIs.
The right to access age-appropriate confidential sexuality education at home and in school should be granted to all students.
Though the sample size was adequate, one major limitation of this study was the difference in the number of students belonging to different categories of schools. The number of students in different divisions was also not equally distributed. The study was representative of students studying in various types of schools in the sub-district. So, the inference of the study can be expected to represent the status of the students of various socio-economic strata.
To conclude, majority of the high school students have poor knowledge of STIs. It is important for the schools to introduce sex-education programs and incorporate them into the educational curriculum in order to increase student awareness about STIs and preventive methods.
留言 (0)