
Remember me
Dear Editor,
Koebner’s phenomenon (KP) is a well-known occurrence in active vitiligo. The role of koebnerisation in the pathogenesis of lip vitiligo is yet to be explored. In-vivo studies have shown that repetitive friction to the skin in non-segmental vitiligo results in the loss of melanocytes by melanocytorrhagy.1 After observing a patient with a vitiligo patch over the lower lip corresponding to a poorly positioned canine, we started observing the teeth alignment closely in patients having lip vitiligo, resulting in the inception of this series of unique patients who had lip vitiligo possibly triggered by misaligned teeth.
Among vitiligo patients registered in the pigmentary disease clinic, those having lip as the initial site of onset were identified and contacted. Only the patients willing to visit the outpatient department for repeat cutaneous examination and further dental assessment were included. Data pertaining to demographics and disease characteristics were collected for 10 patients [Table 1]. The mean age of the patients was 22.6 years (range: 7–36 years), with a male-to-female ratio of 6:4. Seven patients had depigmented lesions over other parts of the body, six of whom had actively progressive disease, with vitiligo disease activity score of 4+. Five patients had acrofacial vitiligo. One patient with extensive vitiligo had stable disease which showed spontaneous repigmentation at body sites other than lips. Lip lesions preceded the onset of vitiligo on other body sites by a mean duration of 10.8 months (range: 4–19 months). None of the patients had any other mucosae involved. There was no personal or family history of vitiligo or autoimmune diseases.
Table 1: Clinicodemographic details of patients with lip vitiligo
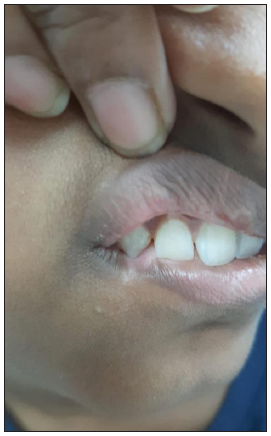
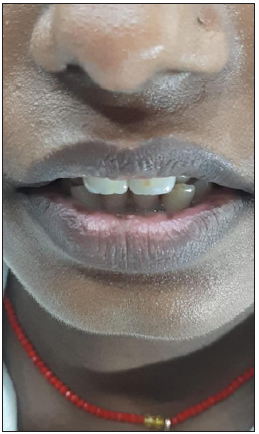
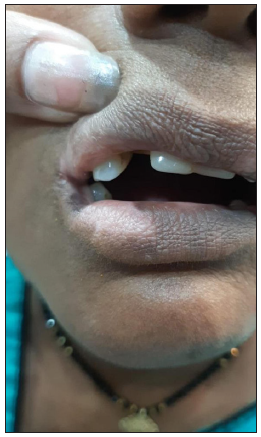
Sl. no. Age (in years) Gender Disease duration (in months) Sites of involvement Total body surface area VIDA Overjet (in mm) Interval between onset of lip lesions and body lesions 1 7 M 4 Lips <1% 4+ 3 - 2 18 M 12 Lips <1% 2+ 5 - 3 21 F 9 Lips <1% 3+ 4 - 4 36 M 16 Lips, face, hands, forearms, arms, trunk, feet 17% 4+ 4 12 months 5 23 F 17 Lips, face, hands, forearms, feet 9% 4+ 6 14 months 6 19 F 24 Lips, face, neck, trunk 12% 4+ 5 19 months 7 34 M 38 Lips, hands, feet 8% 1+ 3 11 months 8 29 M 8 Lips, hands, forearms 5% 4+ 7 4 months 9 27 F 14 Lips, hands, face 3% 4+ 8 10 months 10 12 M 18 Lips, face, hands, forearms, feet 11% 4+ 5 6 monthsExamination of lips revealed depigmented macules, predominantly affecting the lower lip, and preferentially located at the site where misaligned teeth would have contact with the lip [Figures 1a–1d]. The shape of lesions could also be attributed to the position of misaligned teeth in all cases. None of the patients had a history of prior herpes labialis. On dental evaluation, all patients were observed to have an overjet exceeding 3 mm (range: 3 mm–8 mm). The patients were diagnosed with vitiligo, arising from the koebnerising effect of misaligned teeth. Tacrolimus 0.1% ointment was prescribed to all the patients. They were also referred to an orthodontist for teeth realignment.
Export to PPT
Export to PPT
Export to PPT

Export to PPT
The Koebner phenomenon, also known as the isomorphic phenomenon, is ‘the development of the isomorphic pathologic lesions in the traumatised skin of patients having an established cutaneous disease’.2 Many patients with vitiligo first develop the disease de novo after injury. KP can be classified into three types: diagnosis is based on the patient’s history (type 1), by clinical examination (type 2a: depigmentation is present on areas of chronic friction; type 2b: linear depigmentation induced by trauma) or experimentally induced (type 3). In the present series, depigmentation corresponded to areas of repeated and chronic pressure or friction. Therefore, we classified them as type 2a KP.3
A possible pathomechanism of koebnerisation in vitiligo was demonstrated in an in vivo study by Gauthier et al., where authors demonstrated that repeated friction to perilesional skin in non-segmental vitiligo induced detachment and death of melanocytes.4 Melanocyte-specific CD8+ cytotoxic T-cells are recruited in vitiligo skin, and skin trauma acts as an additional trigger to help this process. In our case series, we propose that chronic friction to the lower lip, caused by the misaligned teeth, induced immune-based melanocyte elimination coupled with melanocytorrhagy.
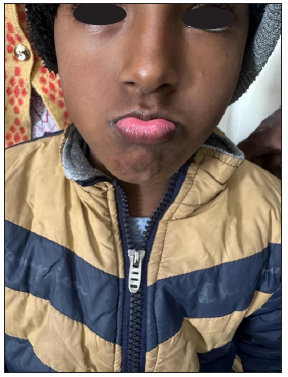
Lip vitiligo is visible, affects the quality of life disproportionately, and is difficult to treat, due to the scarcity of melanocyte reservoir.5 Mucosal lesions respond poorly to both medical and surgical treatments. Friction due to tooth misalignment is a modifiable factor in the causation of lip vitiligo, and orthodontic treatment should be considered as a part of management in such cases. The habit of lip biting is common among children and might play a key role in vitiligo initiation and maintenance [Figures 2a and 2b]. Parents should therefore be educated and children be counselled against this habit. The literature review did not reveal any previous reports that have assessed lip overjet or lip biting in the initiation and propagation of lip vitiligo. Further role of these habits should be explored in lip vitiligo, as they may contribute to progressive and/or persistent depigmentation in a subset of patients.

Export to PPT
Export to PPT
Comments (0)