
記住我


CEL is commonly observed in connective tissue disorders and other conditions that lead to the dislocation of the lens from its natural position. The findings of the current analysis of clinical features and multimodal biometric parameters in children with CEL and myopia demonstrate that AL/CR may be a new potential predictor for the identification of lens dislocation in children, especially for the differential diagnosis with myopia. Lens subluxation was observed after dilatation with compound topicamide, and results of eye examinations support the findings of the current study in terms of AL/CR changes in ocular parameters (Fig. 3). Therefore, the abnormal biological parameters may alert the ophthalmologists to a child with not only myopia but also CEL in a non-mydriasis setting.
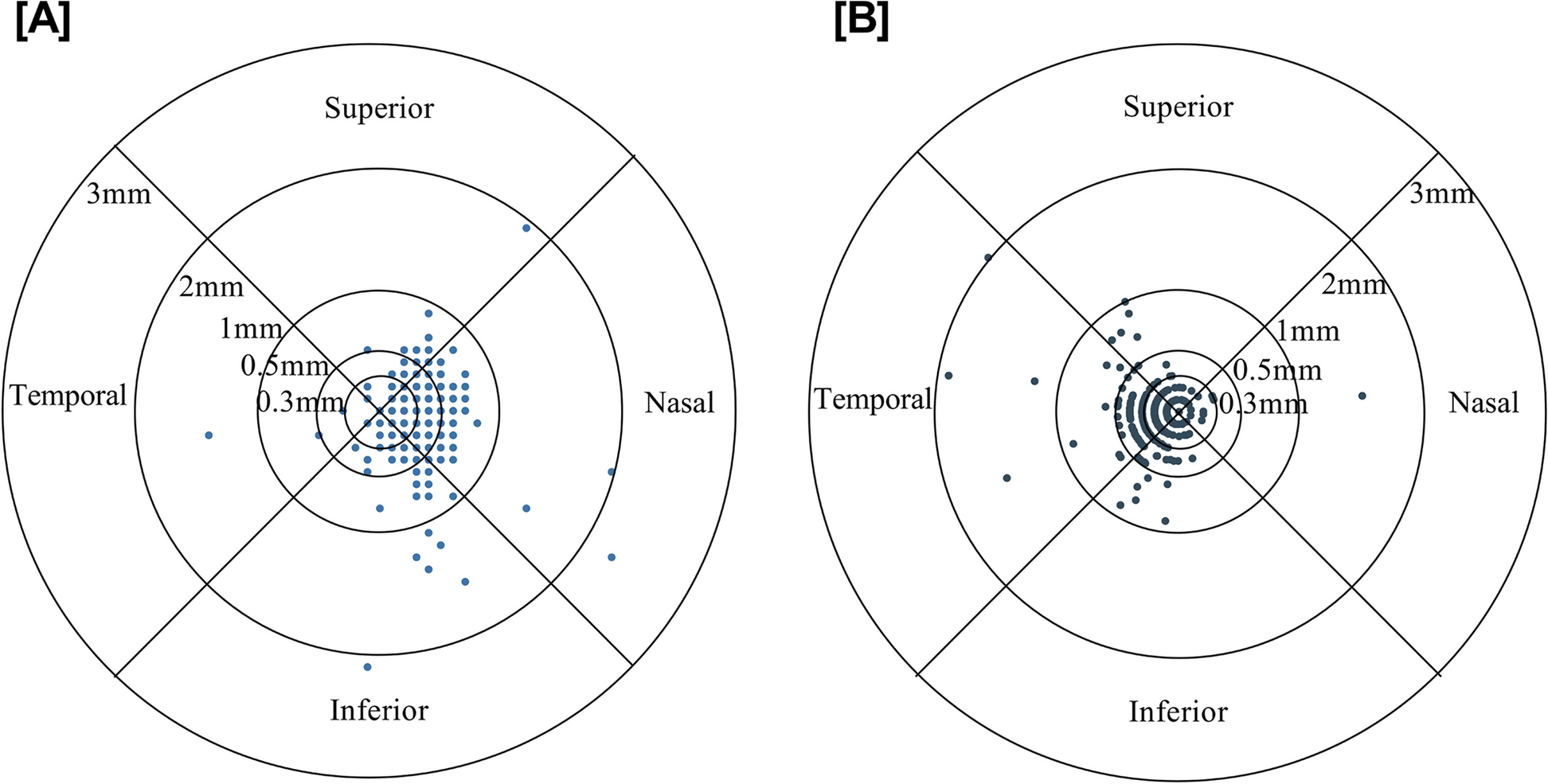
Fig. 3
Representative case in the congenital ectopia lentis group. The left eye of a 5-year-old girl with a temporally subluxated lens. The pupil is dilated with compound topicamide. Poor vision in both eyes is observed at her eye examination. Ophthalmic examination reveals a visual acuity of 6/21 in the left eye. Other ophthalmic examinations show mean keratometry of 40.88 D; axial length of 21.89 mm; and axial length-corneal radius ratio of 2.715 in the left eye. Refractive astigmatism is greater than corneal astigmatism in the left eye (-1.50 D and − 0.97 D, respectively). Slight iridodonesis is observed
In the current study, we matched the CEL group and control group in terms of the SE, and found that changes in ocular biological parameters, especially AL/CR < 3.024, were used to initially screen for occult lens subluxation, while avoiding missed diagnosis.
SE and ALLenticular and axial myopia are the two components of myopia in CEL. Lenticular myopia may result from increasing curvature of the lens (spherophakia) due to the degeneration and relaxation of zonular fibers [6]. Mutations in FBN1 or other genes may also result in axial myopia owing to enlargement of the eyeball, and causing a longer AL [18]. Moreover, defocus and vision deprivation caused by lens displacement can cause pathological AL development, resulting in moderate-to-high myopia [9]. In the current study, the average SE was − 6.25(-8.719~-4.688) D in 3–7-year-old children with CEL, which was far greater than the Ghent-2 criteria for MFS.
Previous studies have reported that MFS patients AL was increased [13, 14, 19,20,21]. Wang et al. found that MFS patients had longer AL (24.71 ± 1.93 vs. 24.00 ± 1.54, p = 0.049) compared with non-MFS patients in a group of 3–6-year-olds [21]. Mulvihill et al. demonstrated that ocular AL was significantly increased in individuals with homocystinuria and lens dislocations [22]. However, the results of the current study showed that the AL in CEL patients was significantly shorter than in myopic patients. In our study, the SE in the two groups was identical, we propose that the main cause of myopia in CEL may be the displacement and deformation of the lens. Although we did not set healthy eyes as a control group, the AL of children with CEL still increased compared to previous studies [23, 24].
Corneal curvatureA number of publications have demonstrated that CC in MFS eyes was flatter than that in non-MFS eyes, and some have proposed a threshold for corneal power of < 41.5 D [9, 13, 15, 25]. It has been suggested that the flattened corneas observed in CEL eyes are due to the increased dimension of the whole eyeball caused by fibrillin gene mutations in the sclera and cornea [9, 15]. Another explanation is that the lower corneal power compensates for the defocus of vision caused by axial growth in myopia [25, 26]. The present study revealed that the average Kmed in the CEL group was dramatically flatter than that in the myopic group. In the CEL group, 71% of eyes were flattened below 41.915 D versus only 7% in the myopic group. However, the AL in the CEL group was significantly shorter than that in the myopic group. Our study demonstrated that the decrease in CC in CEL may not be explained by the concerted mechanism alone and that total ocular enlargement is the major cause.
AstigmatismCAMost studies have indicated that eyes with MFS and ectopia lentis have higher CA [13, 27]. The pathological changes in the cornea might be due to fibrillin gene mutations and associated corneal underdevelopment, a mechanism similar to the one that causes zonular instability and ectopia lentis [27]. However, Sultan et al. showed that in their control group, the mean astigmatism in the 3.0-mm central corneal zone (0.78 ± 1.4 D) was not significantly different from that in the MFS group (1.09 ± 0.87 D) [15]. Wang et al. found no significant difference in CA (1.79 ± 1.13 vs. 1.92 ± 1.07 D, p = 0.584) between MFS and non-MFS patients [21]. In our study, we found that the CA was lower in the CEL group than in the myopic group. In our opinion, the reason may be that our control group had moderate-to-high myopia. Touzeau et al. reported a mean CA of + 0.92 D×91.3° in the high myopic group and + 0.65 D×89.3° in the control group (p < 0.05) [28]. Their study indicated that the correlation with AL was significant for SE and the corneal cylinder. In the present study, the AL in the CEL group was shorter, and the CA was correspondingly lower. Therefore, the CA in the myopic group was higher than that in the CEL group, which might have increased to that of normal eyes, according to previous studies [13, 27].
CA and RAIA and CA are the two components of RA, and CA is critical in normal eyes [29]. In our study, there was a significant difference in magnitude and axis between RA and CA in the CEL group and control groups. The results indicate that ectopia lentis is an important factor leading to internal astigmatism and, therefore, increased RA. Therefore, we should be aware of the possibility of ectopia lentis when a significant difference is found between the RA and CA.
AL/CRMany types of research studies have demonstrated that UBM is of great value in diagnosing lens subluxation and may be invaluable in surgical planning and therapeutic management [12, 30]. The implementation of UBM in children is more difficult than in adults because some procedures are invasive and cause discomfort in children, and additionally, they require the cooperation of the patient. Therefore, researchers have been trying to explore more effective diagnostic methods for lens subluxation in children. Extensive evidence indicates that, for emmetropic participants, a high AL/CR ratio (> 3.0) may serve as a risk factor for the development of myopia [31]. Previous studies have reported that the AL/CR was significantly larger in myopic eyes compared with nonmyopic eyes [32]. Chen et al. proposed that axial length / total corneal refractive power is a potential diagnostic factor that can be used for the early diagnosis of MFS [33]. Wang et al. showed that there was no significant difference in AL/CR (3.03 ± 0.29 vs. 3.01 ± 0.29, p = 0.993) between MFS and non-MFS patients [21]. The results of the current study showed that the AL/CR of CEL group were lower compared with the myopia group. Axial shortening and corneal flattening might have resulted in the reduction of AL/CR in the CEL group. Results from Wang et al. indicate that axial elongation may not be the main cause of myopia in CEL eyes [21].
ROCLuebke et al. reported that Kmax (area under the ROC 0.82, cut-off 41.36 D) provided the strongest effect for differentiation between the MFS and non-MFS groups [25]. Wang et al. found that the area under the ROC was 0.761 for AL, 0.736 for Kmed, and 0.713 for central corneal thickness in the MFS group compared to the non-MFS group [21]. They further indicated that a Kmed of 41.36 D combined with a central corneal thickness of 537.32 mm was the optimal cut-off point (sensitivity 89.8%, specificity 68.7%). The shorter AL, lower Kmed, and longer CR led to decreased AL/CR in CEL patients. AL/CR (area under the ROC 0.960, cut-off 3.024, sensitivity 92.90%, specificity 88.30%) could be used as a screening tool for the differential diagnosis of CEL and myopia. Compared to previous reports, this study suggests a highly specific, easy to master and convenient for use in the clinic [22, 26]. Our method shows additional advantages in the differential diagnosis of CEL, especially when SE < -6.00 D.
This study had several limitations. First, since it was not possible to conduct genetic testing for all children with CEL, a definitive diagnosis, such as MFS or homocystinuria, could not be obtained. Second, because the chosen age range was only 3–7 years, and some children did not cooperate with eye examination, a relatively small number of CEL patients were included, and thus, bias cannot be ruled out. Lastly, this was a retrospective study, and AL, which is a crucial parameter for eyeball development, can be influenced by many factors such as age and genetics.
留言 (0)