
記住我
Dear Editor,
Anaplastic large-cell lymphoma is a CD30+ lymphoproliferative disorder. Skin lesions in anaplastic large cell lymphoma could be primary cutaneous or secondary to systemic disease. Rarely, skin lesions can be the first presenting feature of systemic anaplastic large-cell lymphoma. Negative expression of anaplastic lymphoma kinase (ALK) protein generally indicates primary cutaneous disease but can also be seen in systemic anaplastic large cell lymphoma. Herein, we report an ALK-negative systemic anaplastic large cell lymphoma presenting as localized zosteriform skin nodules.
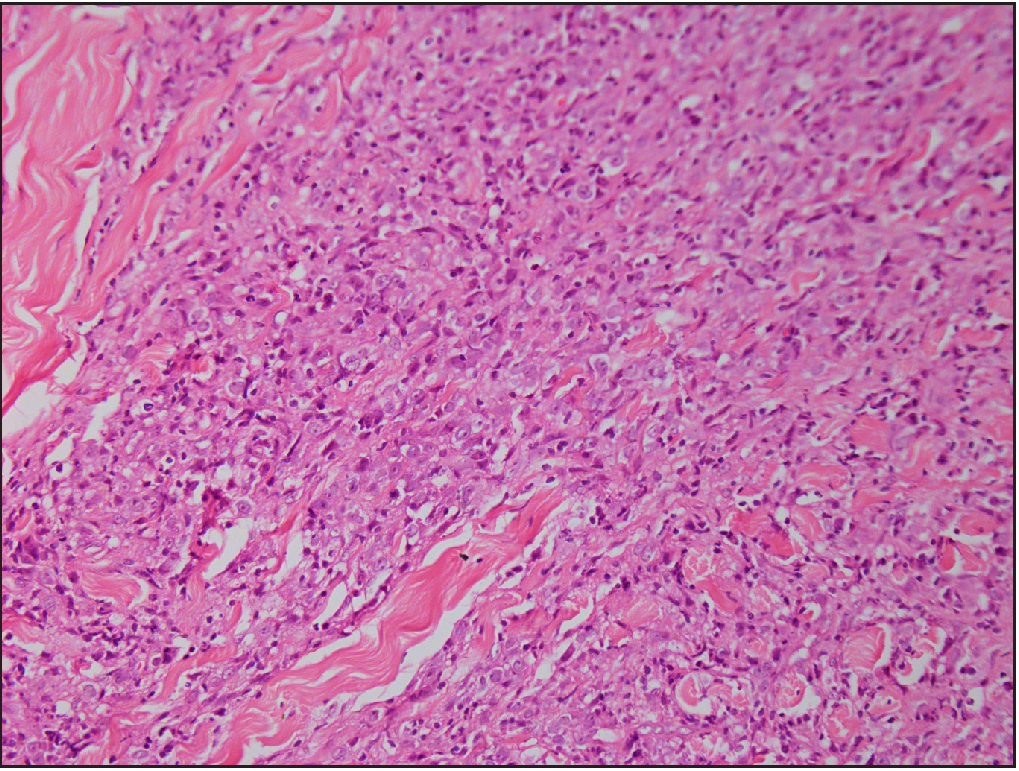
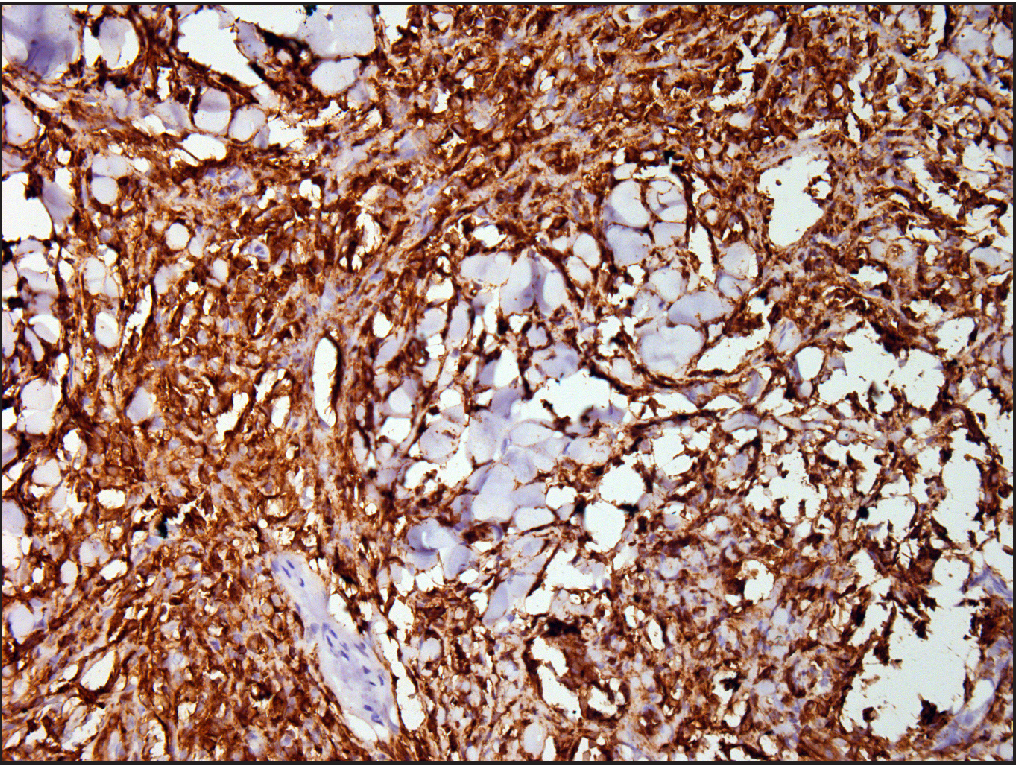
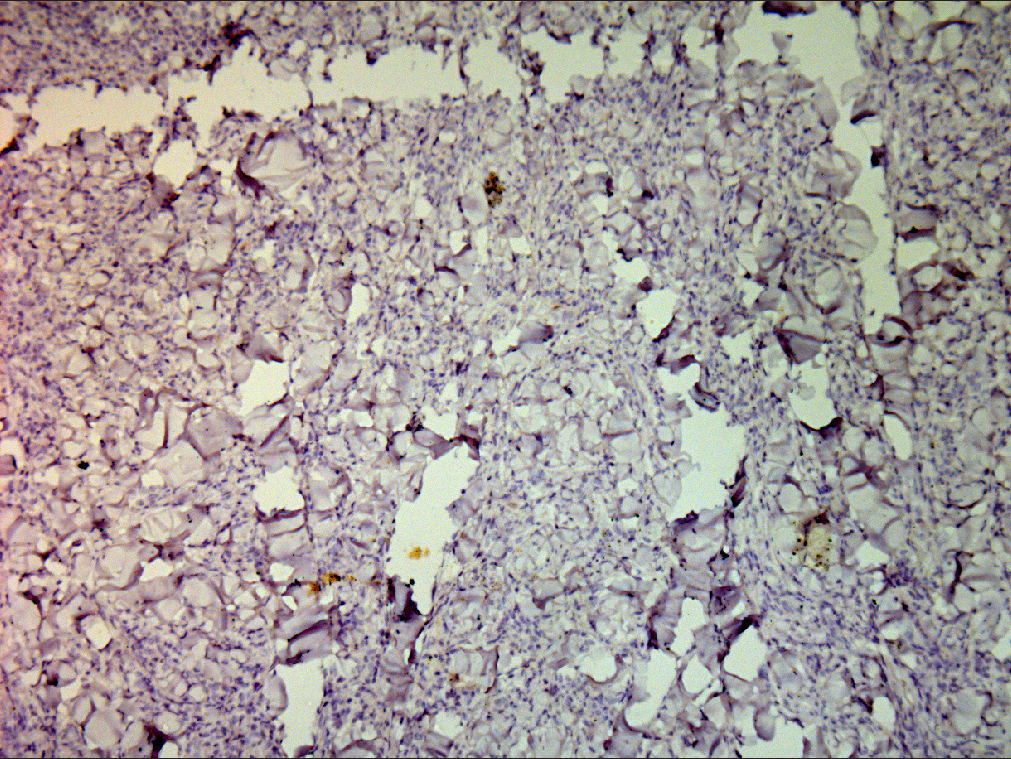
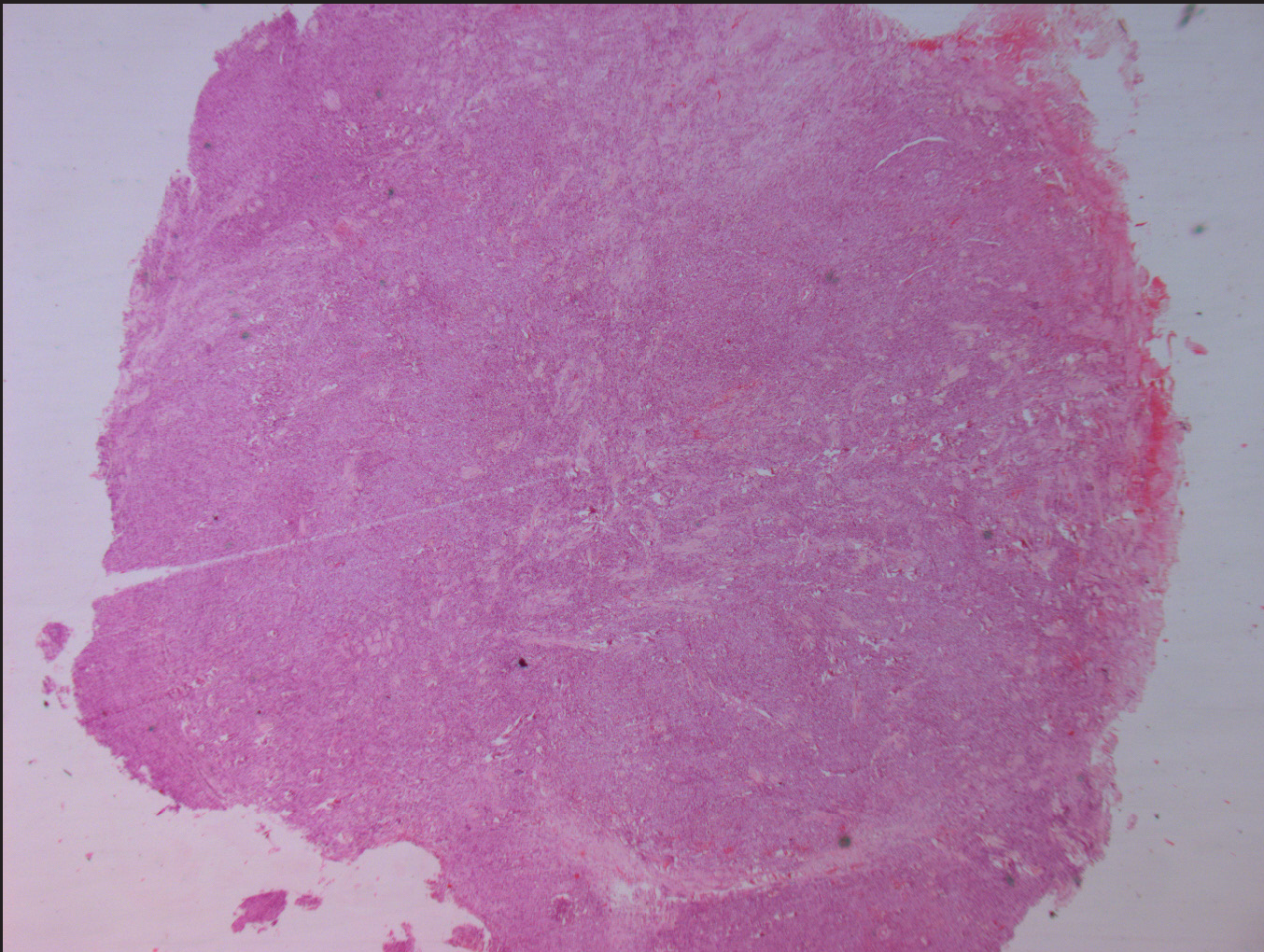
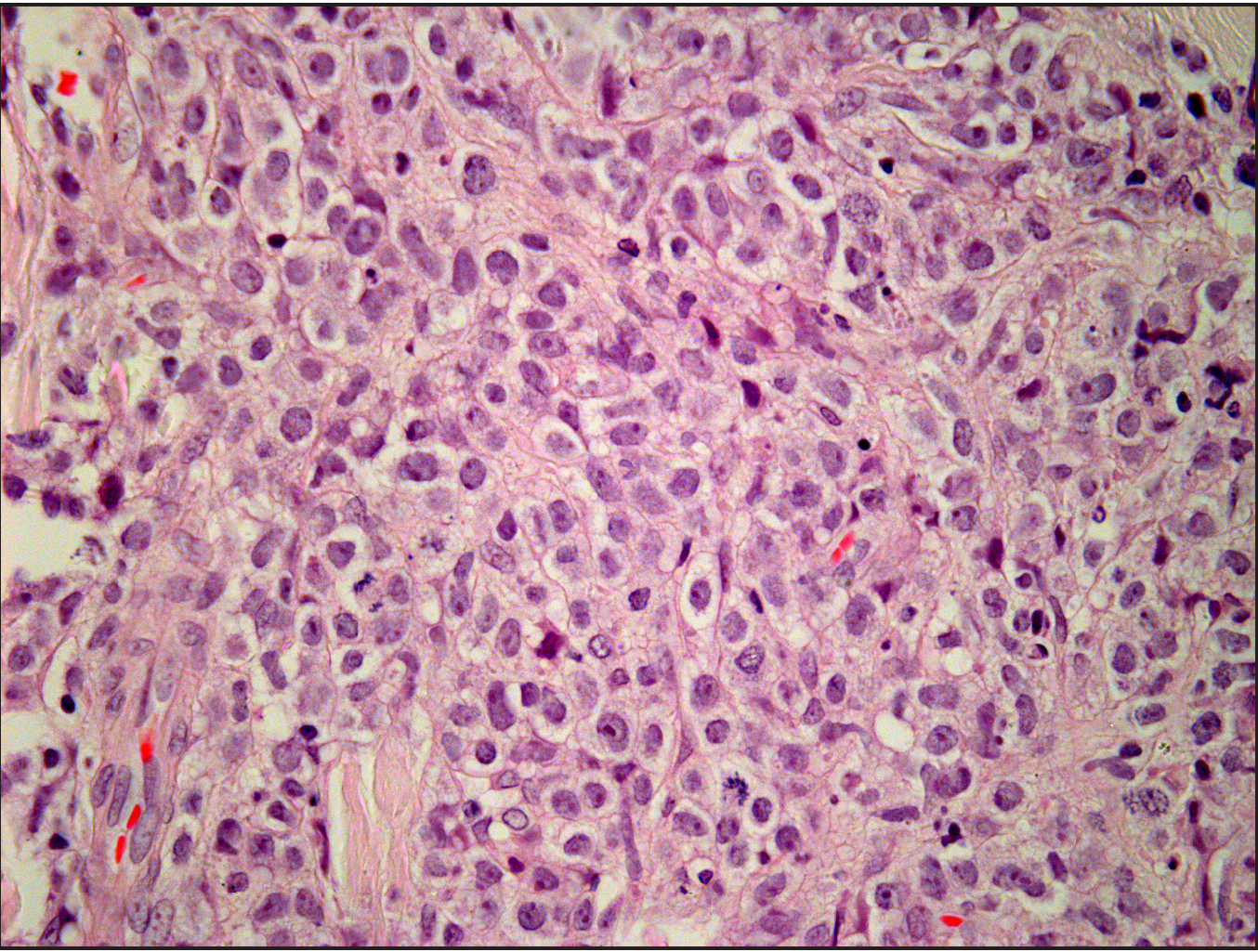
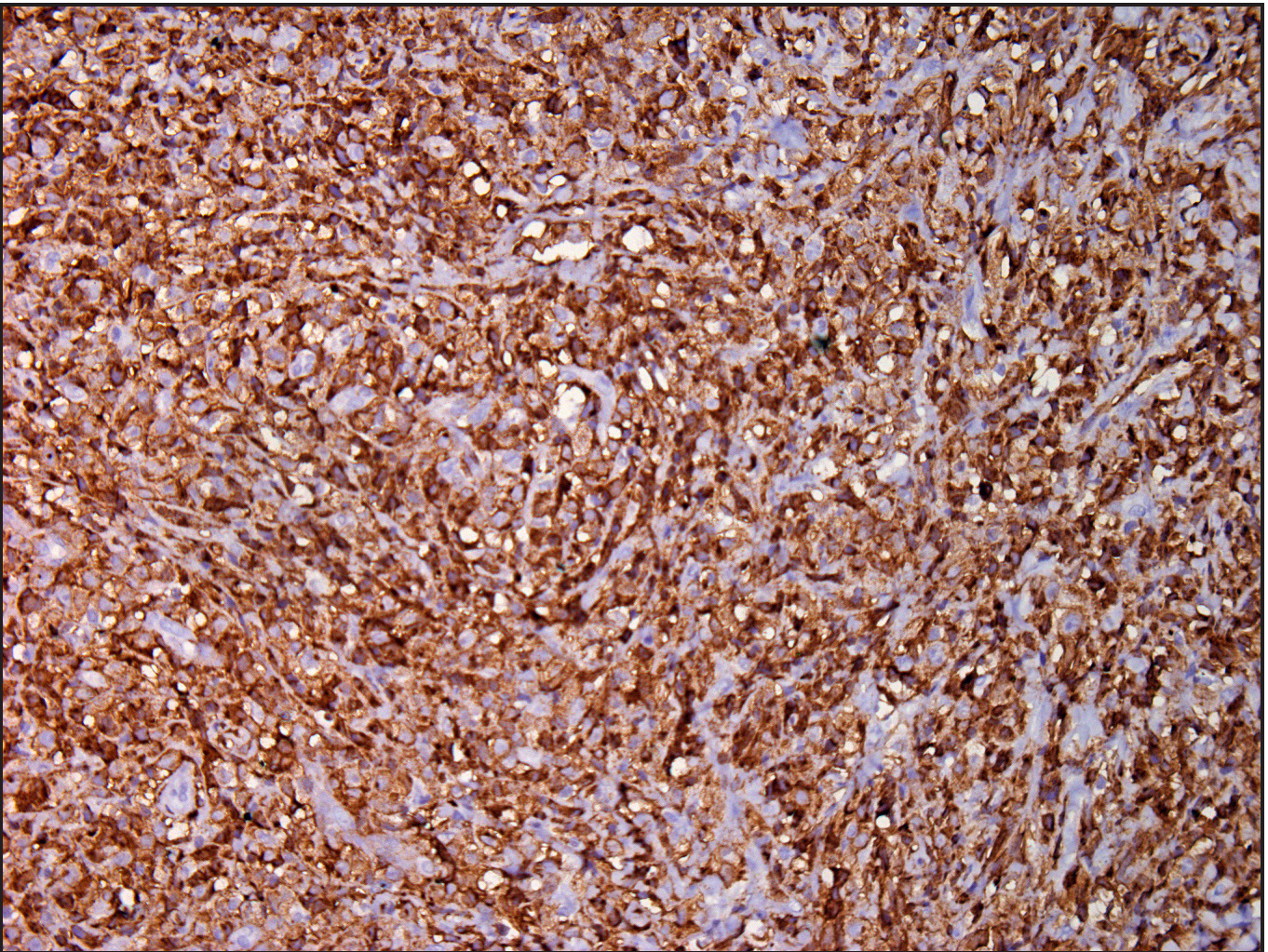
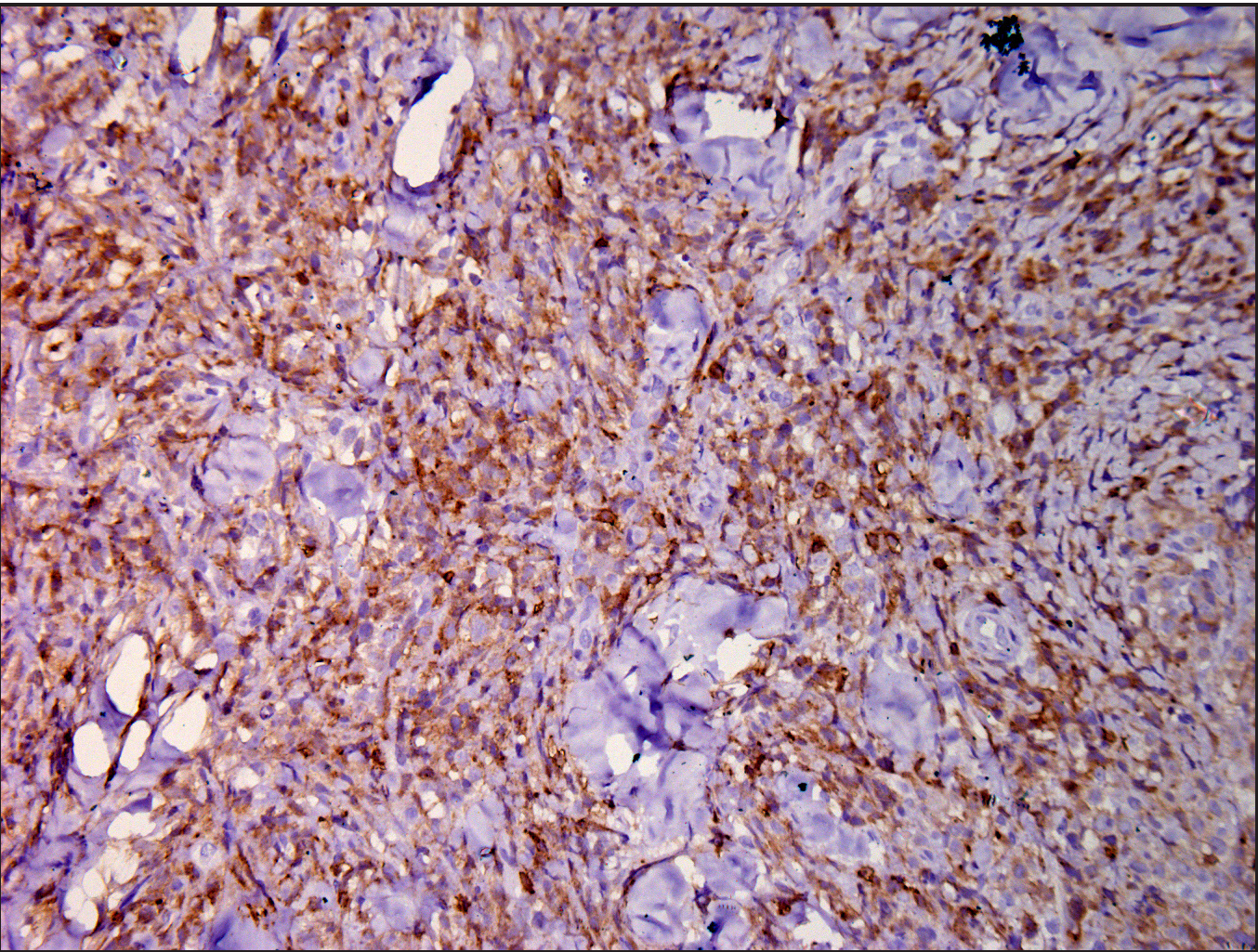
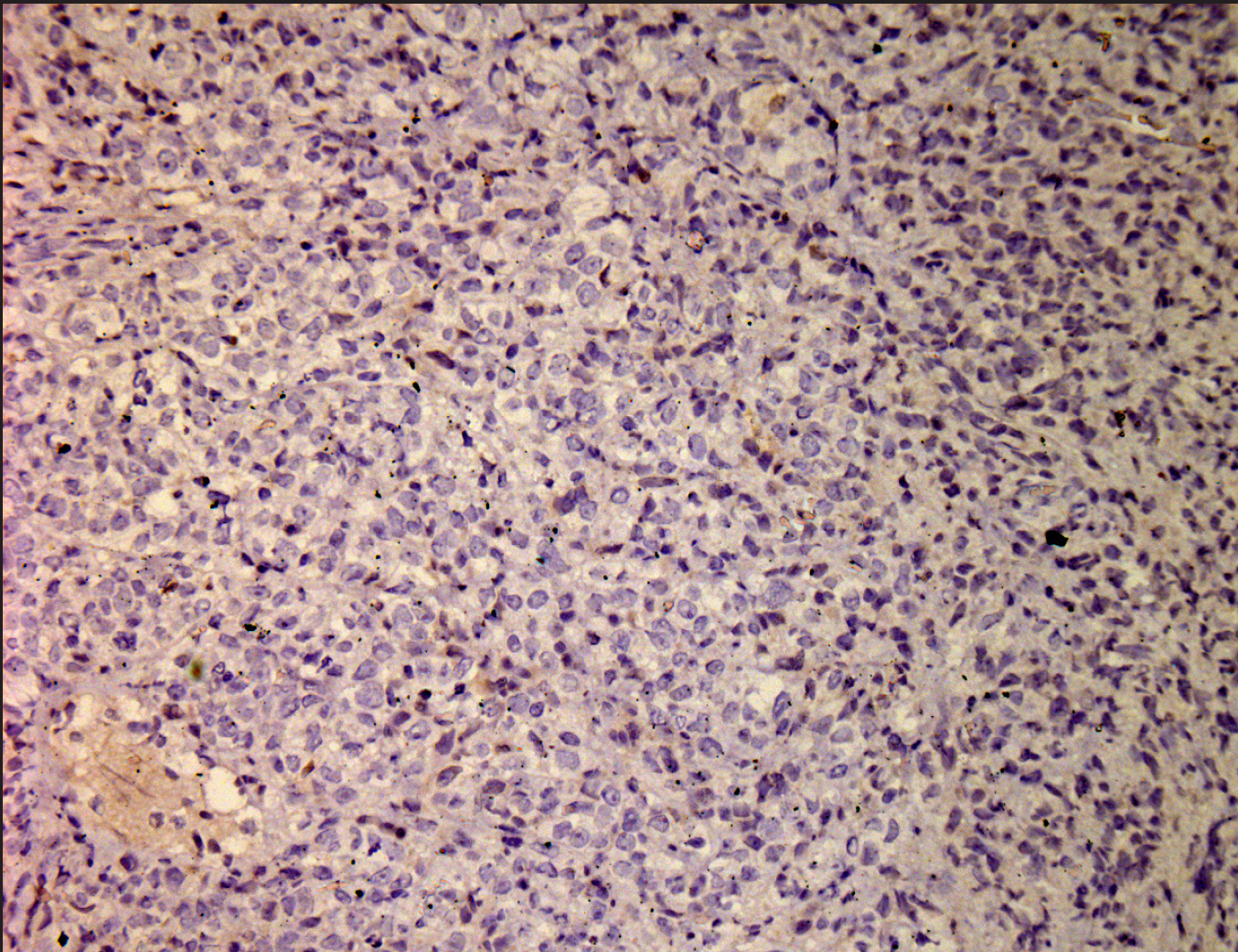
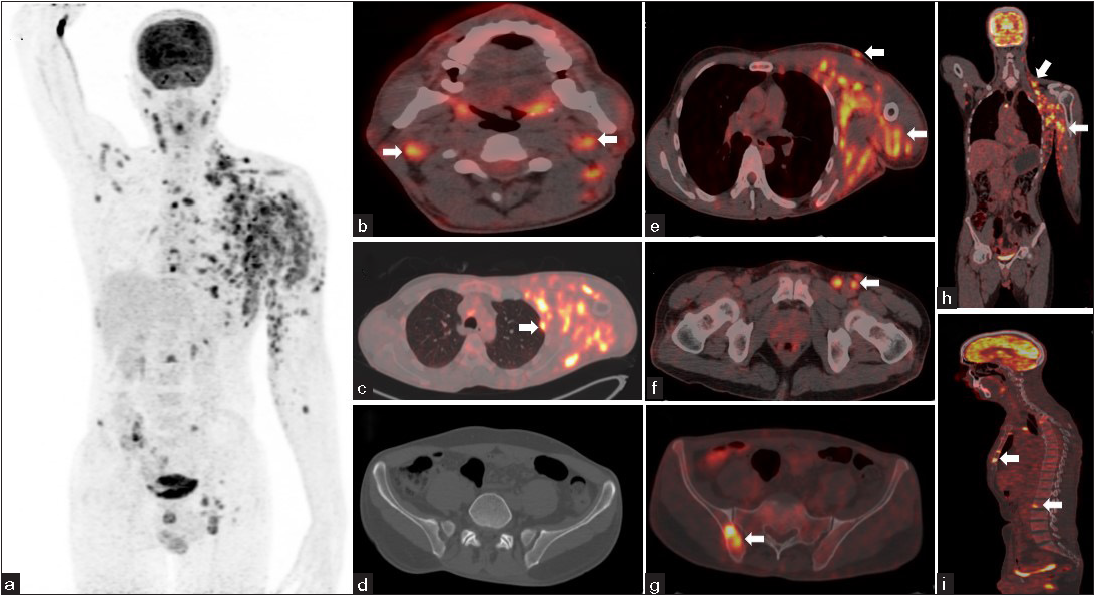
A 48-year-old, otherwise healthy, man presented to us with asymptomatic erythematous nodules on his left arm and chest of six months duration. He had been experiencing intermittent fever and malaise and had noticeable weight loss since the onset of skin lesions. On examination, there were multiple erythematous, mildly tender, firm-to-hard nodules and nodular plaques (size ranging from 0.5 × 0.5 cm to 2 × 1.5 cm) confined to the inner aspect of the left arm extending over the left chest wall in a dermatomal pattern [Figure 1a and 1b]. There were no other skin or mucosal lesions. General physical examination was significant for enlarged firm bilateral cervical, axillary, and left inguinal lymph nodes. Complete blood count, peripheral smear, and serum biochemistry were within normal limits except for a raised serum lactate dehydrogenase (582 IU/L; normal <220 IU/L). Skin biopsy from an erythematous nodule on the chest wall showed a dense diffuse dermal infiltrate of atypical intermediate-to-large sized lymphocytes with prominent nucleoli, frequent mitotic activity, and apoptosis admixed with mature lymphocytes [Figures 2a–2b]. The lymphocytes were strongly immunopositive for CD30 [Figure 2c] and CD4, focally for CD8, and negative for anaplastic lymphoma kinase (ALK) [Figure 2d], CD20, perforin, and Epstein-Barr virus, suggestive of ALK-negative anaplastic large cell lymphoma. Cervical lymph node biopsy showed complete effacement of the nodal architecture by large atypical lymphoid cells [Figures 3a–3b], immunohistochemistry was positive for CD30 [Figure 3c] and CD8 [Figure 3d] , and negative for pan-cytokeratin, CD79a, ALK [Figure 3e], CD3 and CD20. Bone marrow aspirate also revealed infiltration by similar atypical lymphoid cells. A positron emission tomography scan showed metabolically active lymph nodes on both sides of the diaphragm with cutaneous and subcutaneous nodules, ill-defined muscle infiltrates in the left hemithorax and upper limb, and multiple marrow lesions in the axial skeleton, indicating systemic involvement [Figure 4a-4i]. The patient was initiated on 3-weekly cycles of etoposide, cyclophosphamide, doxorubicin, vincristine, and prednisolone (E-CHOP) chemotherapy. The skin lesions and lymphadenopathy completely resolved after 3 chemotherapy cycles [Figure 5], and the patient is planned for 2 more cycles.

Export to PPT

Export to PPT

Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT
Export to PPT

Export to PPT
In a report from the International Peripheral T-cell lymphoma Project (n = 1314), anaplastic large cell lymphoma constituted 13.8% of all cases of T-cell lymphomas, with systemic and primary cutaneous anaplastic large cell lymphoma accounting for 88% and 12% of the cases respectively.1 Systemic anaplastic large cell lymphoma is an aggressive lymphoma and can be divided based on the expression of ALK protein, which is related to a non-random t (2;5) (p23;q35) chromosomal translocation fusing with the NPM gene resulting in the expression of chimeric ALK-NPM gene transcript. While primary cutaneous anaplastic large cell lymphoma is generally ALK-negative, the systemic variant is usually ALK-positive but can also be ALK-negative. ALK-negative systemic anaplastic large cell lymphoma constitutes 15-50% of all cases of systemic anaplastic large cell lymphoma and tends to have a poorer outcome.2 ALK-positive or negative systemic anaplastic large cell lymphoma are treated with a CHOP chemotherapeutic regimen; adding etoposide has enhanced the remission rates, but relapses remain frequent.2 The 5-year survival rate of ALK-negative systemic anaplastic large cell lymphoma (36–49%) is much lower than that of its positive counterpart (60-70%) and primary cutaneous variant (>90%).1,3
Extra-nodal involvement in ALK-negative systemic anaplastic large cell lymphoma has been reported lower than ALK-positive systemic anaplastic large cell lymphoma. However, one large study reported a similar incidence of extranodal involvement (around 20%), but the sites were different. The involvement of skin, liver, and gastrointestinal tract was more frequent in ALK-negative anaplastic large cell lymphoma. At the same time, bone, bone marrow, subcutaneous tissue, and spleen were involved more commonly in ALK-positive form.3 According to Ann-arbour staging, skin involvement is classified as stage IV and is a poor prognostic marker.4
Clinical presentation of primary cutaneous and systemic anaplastic large cell lymphoma with secondary skin involvement is similar and presents as erythematous papules and nodules.5 Primary cutaneous anaplastic large cell lymphoma typically has solitary to few skin lesions, but still can be multifocal in about 20% of cases, while skin lesions in systemic anaplastic large-cell lymphoma are usually disseminated papules and nodules.5 Rarely, systemic anaplastic large cell lymphoma can present with only skin lesions. Our patient presented with localized cutaneous nodules in a zosteriform pattern, but subsequent investigations revealed systemic anaplastic large-cell lymphoma. Such a pattern of cutaneous lesions has been reported in other cutaneous T and B-cell lymphomas but not in anaplastic large-cell lymphoma. In 29 cases of cutaneous malignancies mimicking herpes zoster, 6 (21%) were lymphomas.6 Interestingly, we found a report of herpes zoster-induced cutaneous pseudolymphoma that mimicked anaplastic large-cell lymphoma histologically.7
To sum up, we report this case for its unusual features. Skin lesions in a zosteriform pattern were the presenting feature of systemic anaplastic large-cell lymphoma. Despite the negative ALK expression, the patient had disseminated disease, which re-emphasizes the need for systemic evaluation in all patients of anaplastic large cell lymphoma with skin lesions irrespective of ALK expression.
留言 (0)