Global demographic transformation
The challenge of the baby boomer generation with regards to ageing is vastly under-recognised, not just in the most industrialised countries. Globally, the proportion of elderly people is growing at a rapid pace. Currently, Europe has the highest percentage of population aged 60 or over (25%), surpassed in particular by Japan. However, rapid ageing will occur in other parts of the world as well. By 2050, people aged 60 years or over will account for about 25% or more of the population in all regions of the world, with the exception of Africa [6]. As a result, we will face major challenges in the healthcare and retirement sectors.
Ageing of baby boomers
Currently, the baby boomer generation, is at the height of its economic productivity and is still reasonably healthy. In Europe, it is a reasonable estimate that more than one third of baby boomers already have at least one chronic condition. For example, a survey in Germany found that 38% of respondents suffer from at least one chronic condition [7]. In the US, where baby boomers are 5–10 years older than in Europe, the proportion is likely much higher. It is quite probable that some of them are not yet suffering from the complications of their chronic condition and that they do not yet have multiple chronic conditions. However, 10 to 15 years from now, this group of people will largely no longer be economically productive and will be almost certain to have a high morbidity. So as far as the health system is concerned, this group will basically switch sides. While currently often still being important providers of medical care and contributors to medical insurance, soon they will largely only be recipients of medical care. While now often the most economically productive members of society, in future they will be the recipients of retirement benefits. That change has to be noted. Germany and the US face additional problems, since their life expectancy has developed at a slower pace than northern or southern European countries, even more so in comparison to Japan. Very high expenses, mediocre outcomes and a lack of medical staff even now are a very poor baseline for addressing the ageing of the baby boomer generation indeed.
The world is ageing each country at its own pace
Population ageing can also be expected in other countries, but different countries and regions of the world are ageing at their own pace.
By 2040, the United States is expected to have 22.4% of its population aged 65 and older, which corresponds to the same age group’s current proportion within the German population [8]. Thus, to some extent, the health impact of ageing on the socioeconomic system currently seen in Germany could also be expected in the US. What does that mean in practice? Well, in Germany we already spend around 40% of wages on social security and, on top of that, taxes. German society has thus far been fairly willing to support such costs through redistribution. However, not all countries are prepared to do this – which will also include Germany, if costs were to continue to spiral.
To this day, it has been one of my greatest challenges as Minister of Health to prevent the biggest ever deficit of the German health insurance funds. Without reform, the German health insurance funds were expected to run a 6% deficit of 17 billion euros in 2023. Painful cuts were demanded to balance the budget. How will we solve such problems in 10 years from now? We may have to decide: do we cut services or benefits, do we underprovide, should there be more co-payments or will there be more money from tax revenue or social security contributions? Germany ultimately decided against cuts and in favour of higher social security contribution rates. But how many times will that be possible? As of writing, another increase in the social security rates is next to unavoidable. Cutting services is unwise, because the benefit package is already based on proven needs in Germany. Hospital, primary care and drug pricing laws are on the way to make the system more efficient. Some of these laws are known to have been needed for 10 years. But these laws will only work in the future. Cutting benefits, simply because politics delayed clearly needed reforms, would appear ethically indefensible and politically unwise.
In Germany, population ageing will continue to proceed. By 2040, Germany is expected to have close to 30% of the population aged 65 and older [8]. This is comparable to the current proportion in Japan [8], where the situation is even more grave, with Japanese productivity already suffering because of the major challenges to its social security system. Since many highly developed countries are ageing at the same time, the global economic and social consequences are very difficult to predict.
Socio-economic inequalities in longevity
Additionally, we often under-recognise the large inequality in longevity. The longevity distribution between countries does not reflect the inequity in terms of quality of life and life expectancy differences between the rich and the poor within countries. As an example, when comparing lowest and highest income groups in Germany, the mean life expectancy at birth shows a difference of almost 9 years for men and more than 4 years for women [9]. This trend can be seen in many other countries as well. In the US, the disparities are even greater, with a difference in life expectancy when comparing the richest and poorest 1% of individuals of almost 15 years for men and 10 years for women [10]. Similarly, in Norway, a difference in life expectancy between the richest and poorest 1% of individuals of almost 14 years for men and more than 8 years for women was reported [11]. So we have to face not only the ageing of the baby boomer generation, but also the unsolved problem of inequalities in life expectancy due to socio-economic status [12]. Lifestyle differences, a lack of preventive behaviour and worse access to high-quality medical care have proven to be much more entrenched than expected. Germany has made very little progress in addressing these inequalities, despite a number of laws targeted at improving equality of care, including comprehensive primary prevention interventions by the health insurance funds, disease management programmes, public hospital quality records and minimum volume requirements for public hospitals.
Ageing-associated trends in burden of disease
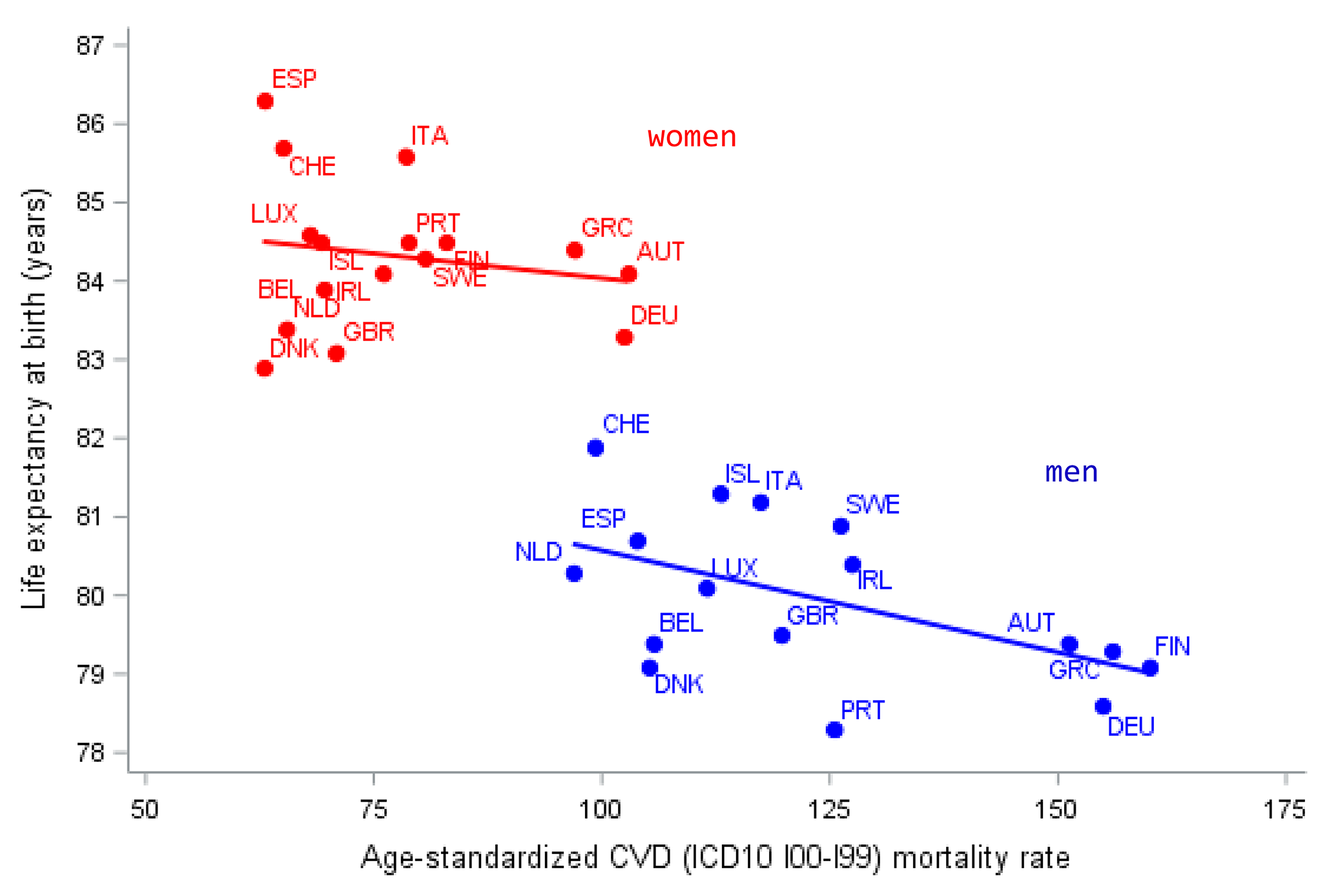
On the topic of burden of disease, it is important to consider which diseases will become more important and which diseases become less important in terms of quality of life and survival as societies age [13]. With today’s knowledge, more than 80% of cardiovascular diseases are preventable under ideal conditions [14]. That may imply that other competing diseases will fill the gap when cardiovascular diseases wane. Indeed, cardiovascular diseases are gradually on the retreat. Unfortunately, it is a different issue when it comes to cancer and dementia, where currently we can at best prevent about 40% of cases of each [15, 16]. What does this mean for policy-making? When infectious diseases and cardiovascular diseases are outcompeted, it means that the majority of the baby boomers are, at some point in their lives, likely to suffer from cancer or from cognitive decline or dementia.
This may make medical care even more expensive. Let us take a look at the costs, for cancer treatment, for example: we are currently only using CAR-T-Cell therapy in a small number of lymphoma and leukaemia types, rarely for common solid tumours. However, it is likely that in the near future, we will be able to use CAR-T-Cell or other forms of personalised medicine for most if not almost all solid end-stage tumours. According to some estimates, this would entail enormous costs of 320,000 euros per treatment. If people survive the cancer, the likelihood of them getting dementia often even increases. In addition to the absolute numbers increasing due to higher survival rates, cancer and its treatment constitute another risk factor for later dementia [17].
A recent study in Germany further highlights the importance of specialised treatment facilities [18]. For ten out of eleven types of cancers analysed, there was a clear-cut advantage in terms of mortality for patients treated in certified cancer centres, compared to non-certified hospitals. Nevertheless, this knowledge is not yet adequately put into practice. For example, this could be addressed by having more certified centres for cancer treatment or by developing pathways to organise treatment outside the centres in the same way. Both goals are part of the hospital reform in Germany mentioned above.
Impact of the COVID pandemic on life expectancy
Socio-economic background was a major driver of COVID mortality in Germany, echoing what is known for chronic diseases. And again, evidence-based treatment and specialisation were linked to better outcomes. For example, in Europe we can see a difference in terms of mortality if we compare ECMO treatment for interstitial lung disease for COVID at specialised centres and non-specialised centres. The mortality rates in specialised centres were much lower. For instance, a French study [19] reported a strong association of improved 90-day survival with increased experience of medical centres in performing ECMO, thus highlighting the relevance of evidence-based analyses and the implementation of evidence-based policies.

留言 (0)