
記住我
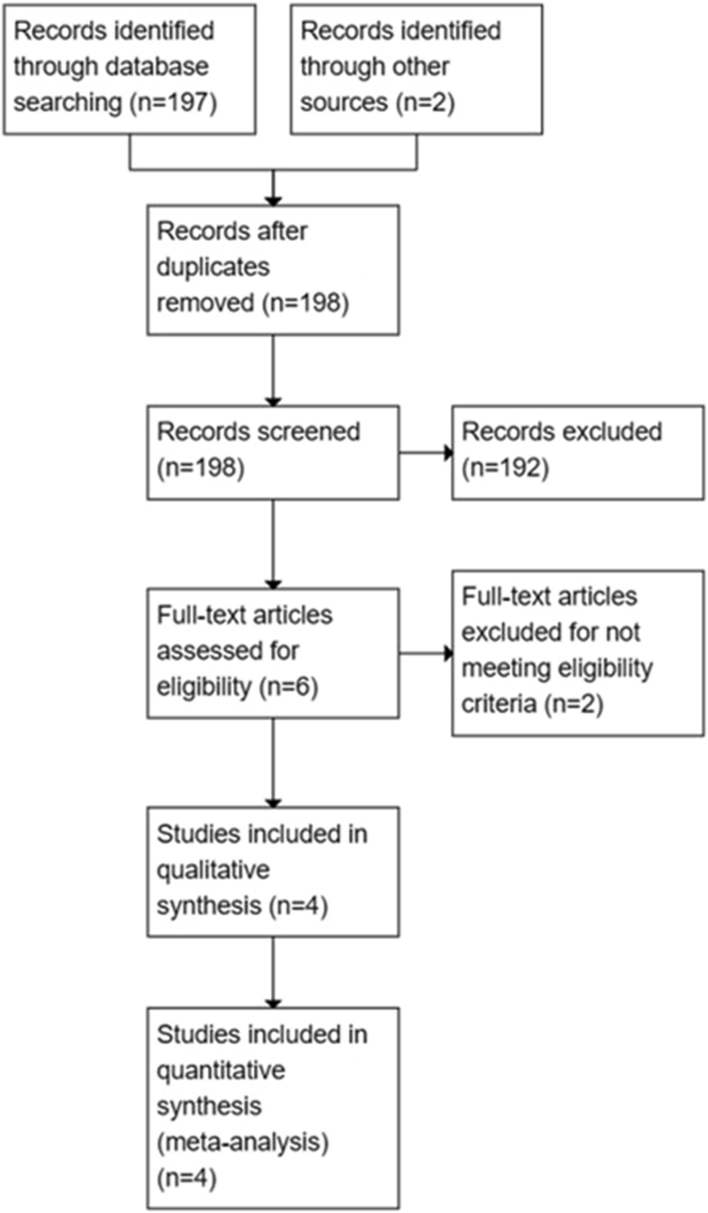
Bleeding complications and non-adherence remain a concern, especially in elderly patients who may be at even higher risk of thromboembolic events associated with AF. In fact, as a result of concern for high bleeding risk, approximately 40–50% of patients do not receive anticoagulation despite of its proven benefit to prevent thromboembolic events [16, 17]. Therefore, mechanical preventive interventions, including the surgical exclusion of the LAA and percutaneous LAAC, have been introduced in clinical practice as a potential valuable alternative to medical management in preventing thromboembolic events in patients with AF. Most LAAC trials do not explicitly include patients with AF who have experienced major bleeding events after receiving NOAC. Consequently, the existing guidelines, primarily derived from clinical trials, assign a Class IIb recommendation for both surgical LAA resection and percutaneous LAAC procedures in patients with contraindications to anticoagulation (Fig. 1).
Fig. 1
Recommendation for percutaneous and surgical LAA occlusion. ACC American College of Cardiology, AHA American Heart Association, ESC European Society of Cardiology, HRS Heart Rhythm Society, LAA left atrial appendage, OAC oral anticoagulation. COR-IIb is defined as usefulness/efficacy is less established by evidence/opinion (European guidelines), benefit ≥ risk (American guidelines)
Surgical LAACSurgical exclusion of the LAA has been used in patients undergoing concomitant procedures, such as coronary revascularization or valve repair. The left atrial appendage occlusion (LAAOS) study was the first randomized study on surgical LAA exclusion. The results of the LAAOS study demonstrated the safety of surgical LAA exclusion during coronary artery bypass surgery [18]. However, complete closure of the LAA was observed in only 45% (5/11) of the cases using sutures and in 72% (24/33) of cases using a stapler. Other studies have also shown that incomplete closure is associated with thromboembolic events [19]. Novel surgical techniques for surgical LAAC have been introduced over time [20,21,22,23]. The AtriClip (Atricure, Dayton, Ohio, US) is a useful device for the management of epicardial LAA, contributing not only to complete exclusion of the LAA but also its electrical isolation [24]. A recent multicenter randomized trial has shown that concomitant surgical LAAC performed during the surgery was associated with a lower risk of ischemic stroke or systemic embolism [25]. Although the trial demonstrated surgical LAAC as a concomitant procedure provided excellent outcome, there is still insufficient evidence for isolated surgical LAAC in patients with AF.
LAAC DeviceIn recent years, several LAAC devices have been developed and introduced as alternatives to anticoagulants for stroke prevention. The Percutaneous Left Atrial Appendage Transcatheter Occlusion (PLAATO) device (eV3, Inc., Plymouth, MA, USA) was the first percutaneous device to be implanted in humans [26]. The device consisted of a self-expandable nitinol frame coated with non-thrombogenic polytetrafluoroethylene, with anchors along three posts to secure the device to the LAA. Previous trials have shown that LAAC with the PLAATO device is safe and effective in patients with NVAF [27, 28]. However, the PLAATO device is no longer commercially available.
The Watchman device (Boston Scientific, Natick, Massachusetts) is a dedicated LAAC device, secondary to the PLAATO device, which received US Food and Drug Administration (FDA) approval after the pilot study [29] in March 2015. The Watchman device is parachute-shaped and self-expanding with a nitinol frame. The device is covered by a membrane cap made of polyethylene terephthalate fabric facing the left atrium body. This membrane prevents thrombus embolization from the LAA and promotes endothelialization. The device is available in five sizes, ranging from 21 to 33 mm, and is the most studied LAAC device. We summarized the previous studies comparing the clinical outcomes of LAAC to oral anticoagulation (OAC) in Table 2. PROTECT-AF trial was a multicenter randomized controlled trial conducted in the USA and Europe between 2005 and 2012. The 707 eligible patients with NVAF and CHADS2 scores of ≥ 1 were randomly assigned in a 2:1 ratio to either LAAC using the Watchman device or warfarin. Warfarin was continued for 45 days after device implantation. Clopidogrel treatment followed for 6 months, and aspirin was administered indefinitely. This trial revealed that LAAC was noninferior to warfarin therapy alone in preventing cardiovascular death, stroke, or systemic embolism in patients with NVAF [30]. PREVAIL (Evaluation of the Watchman LAA Closure Device in Patients with Atrial Fibrillation Versus Long-Term Warfarin Therapy) was another major prospective randomized trial [31] that enrolled 407 patients with AF and CHADS2 scores of ≥ 2 and randomly assigned them to either Watchman LAA closure or warfarin groups in a 2:1 ratio, using a similar primary endpoint to that of PROTECT-AF. In this trial, LAA occlusion was noninferior to warfarin for ischemic stroke prevention or systemic embolism at more than 7 days post procedure. Although noninferiority was not achieved for overall efficacy, event rates were low, and procedural safety significantly improved, compared with PROTECT-AF. A 5-year combined patient-level meta-analysis of PROTECT AF and PREVAIL has demonstrated that LAAC with Watchman is effective in preventing stroke in NVAF, offering comparable results to warfarin. Furthermore, LAAC with Watchman presents additional advantages, including reductions in major bleeding events, particularly hemorrhagic strokes, and decreased mortality rates [32]. In the recent era, NOACs have gained popularity due to their efficacy, which is similar or superior to VKAs in NVAF management, along with a lower rate of intracerebral bleeding [33, 34]. The Left Atrial Appendage Closure vs. Novel Anticoagulation Agents in Atrial Fibrillation (PRAGUE-17) trial, a multicenter randomized noninferiority trial comparing LAAC with NOACs, has provided valuable insights. PRAGUE-17 demonstrated that LAAC is noninferior to NOACs in preventing major AF-related cardiovascular, neurological, and bleeding events among high-risk patients for stroke with an increased risk of bleeding [35]. While PRAGUE-17 has started to explore the potential of transcatheter LAAO as an alternative for NOAC candidates, it is worth noting that the enrolled patients in this trial were already at a high risk for bleeding or had failed oral anticoagulant treatment. Moreover, efficacy and safety endpoints in this noninferiority design were combined in the study. Currently, several complication randomized trials with larger sample sizes and longer follow-up periods aim to provide more comprehensive data (Fig. 2). These trials intend to demonstrate individual ischemic and bleeding endpoints in patients who are optimal candidates for NOAC therapy. Larger sample sizes will enable more robust analyses and investigations into specific subgroups within the population.
Table 2 Randomized trials comparing left atrial closure devices versus oral anticoagulation in patients with nonvalvular atrial fibrillationFig. 2
Ongoing trials comparing clinical outcomes of LAAC to NOACs. LAAC left atrial appendage closure, NOACs novel oral anticoagulants
The CAP Registry was another study conducted on 566 patients that suggested that Watchman implantation is a favorable and safe alternative and that complications associated with Watchman implantation significantly decrease in frequency with operator experience [36]. In 2015, a meta-analysis of 2406 patients with NVAF reported that patients who underwent LAAC had significantly fewer hemorrhagic strokes (hazard ratio [HR] 0.22, p = 0.004), cardiovascular and all-cause deaths (HR 0.48, p = 0.006), and bleeding (HR 0.51, p = 0.006) than those who received warfarin, with a mean follow-up of 2.69 years [37]. The Initial US clinical experience has evaluated the procedural outcomes and complication rates of all patients with the Watchman device in the USA since FDA approval [38]. Among 3822 consecutive patients, the device was successfully implanted in 3653 (95.6%) patients, with a median procedure time of 50 min (range 10–210 min). Procedural complication rates included 39 pericardial tamponades (1.02%), 3 procedure-related strokes (0.078%), 9 device embolizations (0.24%), and 3 procedure-related deaths (0.078%). Additionally, 71% of implanting physicians performed these procedures for the first time. Nevertheless, the study showed a high clinical success rate for the procedures and a low complication rate. The clinical outcomes of the Watchman device for LAAC are summarized in Table 3. Watchman FLX (Boston Scientific) is a newer generation of LAAC devices that has been available since November 2015. The Watchman FLX devices are available in five sizes (20–35 mm) for ostia measuring 15–32 mm wide. The variety of device sizes allowed for the treatment of both smaller and larger LAA ostia, compared with the Watchman device. Additionally, a shorter Watchman FLX device enables implantation even in chicken-wing-shaped LAAs with shallow or broad LAAs. There are some key differences between the previous generation of Watchman and the Watchman FLX, such as the polyester fabric coverage, distal end design, number of anchors and struts, proximal face, and recommended compression. A fully rounded ball design is beneficial for safely advancing and maneuvering within the LAA. Partial and full device recaptures were performed during the procedure, if necessary, to achieve precise placement in the LAA. Some studies showed the high procedural success rate of LAAC with Watchman FLX and favorable outcomes [39,40,41]. Additionally, the SURPASS study of the National Cardiovascular Data Registry Left Atrial Appendage Occlusion (NCDR-LAAO) Registry was real-world data including the largest number of patients who underwent Watchman FLX. The results showed that safety and efficacy was similar to those of a previous study [42].
Table 3 Left atrial appendage closure outcomes with the Watchman deviceIndication for LAACIn a previous study using data from the NCDR LAAO Registry, the most frequently reported procedural indications at clinical sites were an elevated risk of thromboembolic stroke and a history of major bleeding [43]. Consequently, concerns related to a high risk of falls and patient preference were raised. A noteworthy finding from this analysis was that a significant majority of patients had documented histories of clinically significant bleeding, predominantly stemming from gastrointestinal sources, with intracranial bleeding reported in approximately 12% of the cohort. In parallel, the European Heart Rhythm Association Survey identified the most frequent applications of LAAO in patients with a CHA2DS2-VASC score ≥ 2 with a contraindication to OAC, a CHA2DS2-VASC score ≥ 2 combined with a HAS-BLED score ≥ 3, occurrences of embolic events despite OAC administration, and a CHA2DS2-VASC score ≥ 2 in the presence of end-stage renal failure [44]. Consequently, these findings highlighted a high risk for stroke and bleeding as primary indications for LAAO. Contrastingly, 13.3% of patients enrolled in the PROTECT-AF and PREVAIL randomized clinical trials had experienced prior bleeding events [30, 31]. The observed disparities in patient characteristics may stem from variations in the inclusion criteria of pivotal trials, which guided FDA approval of the device, and actual clinical practice. While pivotal trials enrolled patients boasting a CHA2DS2-VASC score ≥ 1, making them eligible for long-term OAC, real-world scenarios led to the consideration of short-term OAC therapy for patients with a CHA2DS2-VASC score ≥ 3, as they were deemed unsuitable for long-term OAC therapy. We summarized the indications and contraindications for LAAC procedure in Table 4.
Table 4 Indications and contraindications for left atrial appendage closure (LAAC)Antithrombotic Strategy After LAACPostimplantation anticoagulation and antiplatelet therapy management remain clinical concerns because most patients who undergo LAAC have a high risk of bleeding. In previous trials, warfarin and aspirin were administered 45 days after LAAC device implantation. If device-related thrombosis (DRT) was not detected on TEE at 45 days, warfarin was discontinued. Aspirin and clopidogrel were then administered for 6 months, followed by aspirin indefinitely. This is a standard and recommended regimen following LAAC device implantation. Current guidelines recommend oral anticoagulants for 45 days, followed by dual antiplatelet therapy (DAPT) for 6 months for DRT and potential stroke events [45]. However, controversy surrounds the use of antithrombotic therapy in patients with LAA occlusion. The ASA Plavix Feasibility Study with Watchman Left Atrial Appendage Closure Technology (ASAP) was conducted in patients with both high bleeding risks and absolute contraindications to warfarin [46]. This multicenter prospective nonrandomized study assessed the safety and efficacy of LAAC with the Watchman device in patients with NVAF and CHADS2 scores of ≥ 1 who were ineligible for OAC. DAPT was administered for 6 months after LAAC without warfarin. There were four cases of all-cause mortality or systemic embolism (2.3% per year), three cases of ischemic stroke (1.7% per year), and one case of hemorrhagic stroke (0.6% per year). The authors concluded that using the Watchman device with DAPT, instead of warfarin transition, as a postprocedure OAC is a reasonable option for patients at high risk for stroke with contraindications to systemic OAC. However, previous study reported that DAPT after LAAC is associated with a substantial incidence of bleeding events. The use of low-dose NOACs may provide an ideal balance between keeping the risk of thromboembolic events low and reducing the likelihood of bleeding events in patients with NVAF after LAAC. The ELDERCARE-AF (Edoxaban Low-Dose for Elder Care Atrial Fibrillation Patients) trial demonstrated a reduction in stroke or systemic embolism with once-daily 15 mg edoxaban in Japanese patients with AF aged 80 years or older ineligible for standard OACs [47]. Moreover, Della Rocca et al. reported that long-term half-dose NOAC significantly lowered the risk of the composite endpoint, including DRT, thromboembolic events, and major bleeding events, compared to a standard antithrombotic therapy based on antiplatelets [48]. We summarized antithrombotic treatment after LAAC in both previous and ongoing trials in Table 5. It should be noted that the evidence supporting reduced-dose anticoagulant regimens after LAAC is currently limited. Thus, further investigation in antithrombotic therapy for LAAC is required to determine the optimal regimen for patients with AF.
Table 5 Antithrombotic treatment after LAAC in trialsComplicationsSome data and evidence are available regarding the safety and efficacy of LAAC devices that have been developed over time. However, LAAC is not devoid of complications. LAAC is a prophylactic treatment and avoiding complications of the procedure is imperative. PROTECT-AF reported a relatively high rate of complications including cardiac tamponade (4.3%), procedure-related stroke (1.15%), and device embolization (0.6%) [30]. A meta-analysis that included 49 studies involving 12,415 patients showed that the pooled proportion of all-cause stroke was 0.31%, major bleeding requiring transfusion was 1.71%, and pericardial effusion was 3.25% [49].
Pericardial effusion is a common and serious complication of LAAC. Catheter and device manipulations within the thin-walled LAA cause pericardial effusion, especially in transseptal punctures. The anchors and outward radial force of the device can damage the LAA wall. Observational modalities, such as TEE, during the procedure, are essential to prevent pericardial effusion. If complications arise, percutaneous or surgical drainage may be considered to stabilize the hemodynamics. Air embolization is a rare but potentially fatal complication, and the use of large delivery sheaths for LAAC is a risk factor for air embolization. Periprocedural stroke due to thrombus and debris is also a rare but devastating complication.
Device embolization is an acknowledged complication of LAAC procedures, with an incidence rate of less than 2% reported in clinical practice [50]. Device embolization occurred more frequently postoperatively, requiring surgical retrieval, and had higher mortality rates than intraoperative embolization. Size mismatch and inexperienced operators may be the main reasons for device embolization [51].
Peridevice leaks remain a risk factor for stroke risk, due to the inherent anatomical complexity of the LAA, which presents a challenge to achieving complete conformity with the LAAC device and the LAA orifice. The Watchman FLX device offers advantages by enabling distal positioning during deployment, as well as the ability to recapture and redeploy the device, which proves beneficial in preventing postimplantation leaks. Nevertheless, it is important to highlight that in the PINNACLE FLX study, leaks measuring less than 5 mm occurred in 10.5% of patients at 1 year after LAAC with Watchman FLX devices [39]. Dukkipati et al. reported that leaks of less than 5 mm following percutaneous LAA closure with the Watchman device were associated with an increased risk of ischemic stroke or systemic embolism [52]. Hence, it is crucial for operators to carefully optimize device positioning to minimize peridevice leaks during implantation, with the assistance of TTE.
DRT after device implantation remains a major concern and is typically detected during routine follow-up after LAAC or after an ischemic event using TTE or CT. Recent studies have reported that DRT after LAAC is strongly associated with a higher risk of thromboembolic events, with an incidence ranging from 1.6% to 16% [53, 54]. The causative risk factors for DRT include patient characteristics, procedural factors, device specifications, and post-LAAC medical regimens. Although continued anticoagulation therapy is effective in resolving this problem and preventing DRT recurrence [55], long-term anticoagulation increases bleeding events in populations with high bleeding risk. Optimal diagnostic criteria and treatment regimens for DRT are warranted in the future.
Other New DevicesAmplatzer Amulet Left Atrial Appendage OccluderThe Amplatzer Cardiac Plug (ACP) (St. Jude Medical, Minneapolis, MN, USA) is one of the most commonly used devices for percutaneous LAAC and received Conformité Européenne (CE) mark approval in 2008. The ACP is constructed from a mesh of woven nitinol, with the lobe and disk connected by a flexible waist. The lobe is held in the neck of the LAA and stabilized by retention wires, and the disc seals the orifice of the LAA. The Amplatzer Amulet system (Abbott Vascular, Santa Clara, CA, USA) is a second-generation LAAC device commercially available in Europe since 2013. The Amulet device has a larger disc diameter, a longer lobe and waist, and more retaining wires than the ACP device. The Amulet device is preloaded within the delivery system and available in eight different sizes (16–34 mm). The larger size of this device allows for the treatment of a wider range of anatomical variations. A multicenter prospective real-world registry with the second-generation Amulet device included 1088 patients (aged 75 ± 8.5 years, 64.5% male; CHA2DS2-VASc, 4.2 ± 1.6; HAS-BLED, 3.3 ± 1.1) with NVAF who showed high implant success rates (99%) and lower periprocedural complication rates (3.2%), compared with those of first-generation ACP registries [56]. Moreover, the Amulet IDE trial (Amplatzer Amulet Left Atrial Appendage Occluder IDE Trial) was conducted to assess the safety and efficacy of the Amulet device compared with the Watchman device [57]. The Amulet IDE trial was a large randomized, multicenter, controlled trial conducted on 1878 patients with high risks of stroke or systemic embolism. The Amulet group had a slightly higher success rate in the initial implantation procedure (98.4% vs. 96.4%). The Amulet device achieved comparable results to the Watchman device on the primary effectiveness endpoint (2.8% vs. 2.8%, p < 0.001 for noninferiority) and the composite of stroke, systemic embolism, and all-cause death (5.6% vs. 7.7%, p < 0.001 for noninferiority). Recently, a finding of the extended follow-up in the Amulet IDE trial was presented which showed that the Amulet device provided similar clinical outcomes to those of the Watchman device over 3 years.
WaveCrestThe Wavecrest LAA device (Biosense Webster, Inc., Irvine, CA) received CE Mark approval in 2013 but is not yet available for commercial distribution in the USA. WaveCrest consists of a self-expanding nitinol frame covered by expanded polytetrafluoroethylene with 20 anchoring points that allow repositioning. WaveCrest was available in three sizes: 22, 27, and 32 mm. One unique feature of this device is its ability to perform distal contrast injection, which is useful for the assessment of occlusion and stability. Currently, the WAVECREST 2 trial is ongoing in the USA. The randomized controlled trial was designed to ensure that the safety and effectiveness of the WaveCrest device are comparable to those of the Watchman device.
LAmbreThe LAmbre LAA Closure System (Lifetech Scientific, Shenzhen, China) is a new self-expanding occluder composed of a nitinol mesh and polyester membrane with an umbrella and a cover connected by a short central waist. The LAmbre implant is available in 15 different sizes ranging from 16 to 36 mm based on the umbrella diameter. The device is delivered in 8- to 10-French sheaths and allows for complete recapture and repositioning within the LAA. The unique feature of the device is that it consists of a U-shaped anchor and hook stabilization system targeting the LAA trabeculae and pectoralis muscles. LAmbre received the CE mark on June 15, 2016. Huang et al. [58] reported the safety and effectiveness of the LAmbre device in a multicenter prospective study of 153 patients with AF and CHADS2 scores of ≥ 1. The LAA occlusion was successfully performed in 152 patients, and serious complications occurred in five patients. Ischemic stroke occurred in two patients, with incomplete LAA sealing in one patient, and no device embolization during the 12-month follow-up.
UltraseptThe Ultrasept device (Cardia Inc., Eagan, MN, USA) is a novel, self-expandable, bulb-and-sail device intended to provide complete coverage of the LAA orifice. The device consists of a nitinol frame and distal cylindrical anchor, which are deployed and secured with a platinum/iridium collar and polyvinyl alcohol foam. The delivery sheath is currently available and ranges from 10 to 12 French. The Ultrasept device is fully retrievable, allowing it to be repositioned as many times as needed to ensure proper placement during deployment.
LARIATThe LARIAT suture delivery device (SentreHEART, Redwood, California, USA) occludes the LAA via an epicardial suture and eliminates the need for a permanent implant inside the LAA. The procedure requires that a guide wire tipped with a magnet be inserted into the epicardium and endocardium after percutaneous puncture to deliver sutures for snipping the LAA at the epicardium. The device consists of a clever combination of a magnet-tipped wire that is placed in the endocardium via transseptal access and a second magnet-tipped wire that is placed in the epicardial space via pericardial access. The LARIAT device received a CE mark in 2009 and 510(k)-class II clearance in the USA. The LAA is a recognized source of sustained AF, and the LARIAT device contributes not only to the prevention of thromboembolic events but also to the improvement of AF ablation success. The LAALA-AF Registry demonstrated that the addition of LARIAT closure to a conventional AF ablation was beneficial in maintaining sinus rhythm in patients with persistent AF [59]. A total of 138 patients, with 69 in each group (the LARIAT group and the ablation-only group), were enrolled in the study. After one ablation procedure followed by 12 months of antiarrhythmic therapy, the rate of freedom from AF was 65% in the LARIAT group, compared with 39% in the ablation-only group (p = 0.002). This study revealed that LAA ligation with the LARIAT device for conventional ablation improves the outcome of AF ablation.
留言 (0)