
記住我


A 38-year-old female patient presented to the ophthalmologist on 16 January 2022 with complaints of blurred vision and redness in her left eye for one day. She had suffered sudden visual loss in her right eye 10 years prior, and was diagnosed with ARN in her right eye according to the standard diagnostic criteria for acute retinal necrosis syndrome [4]. No molecular, biological or immunological detection method was applied due to technical limitations at that time. Vitrectomy and silicone oil injections were performed due to rhegmatogenous retinal detachment.
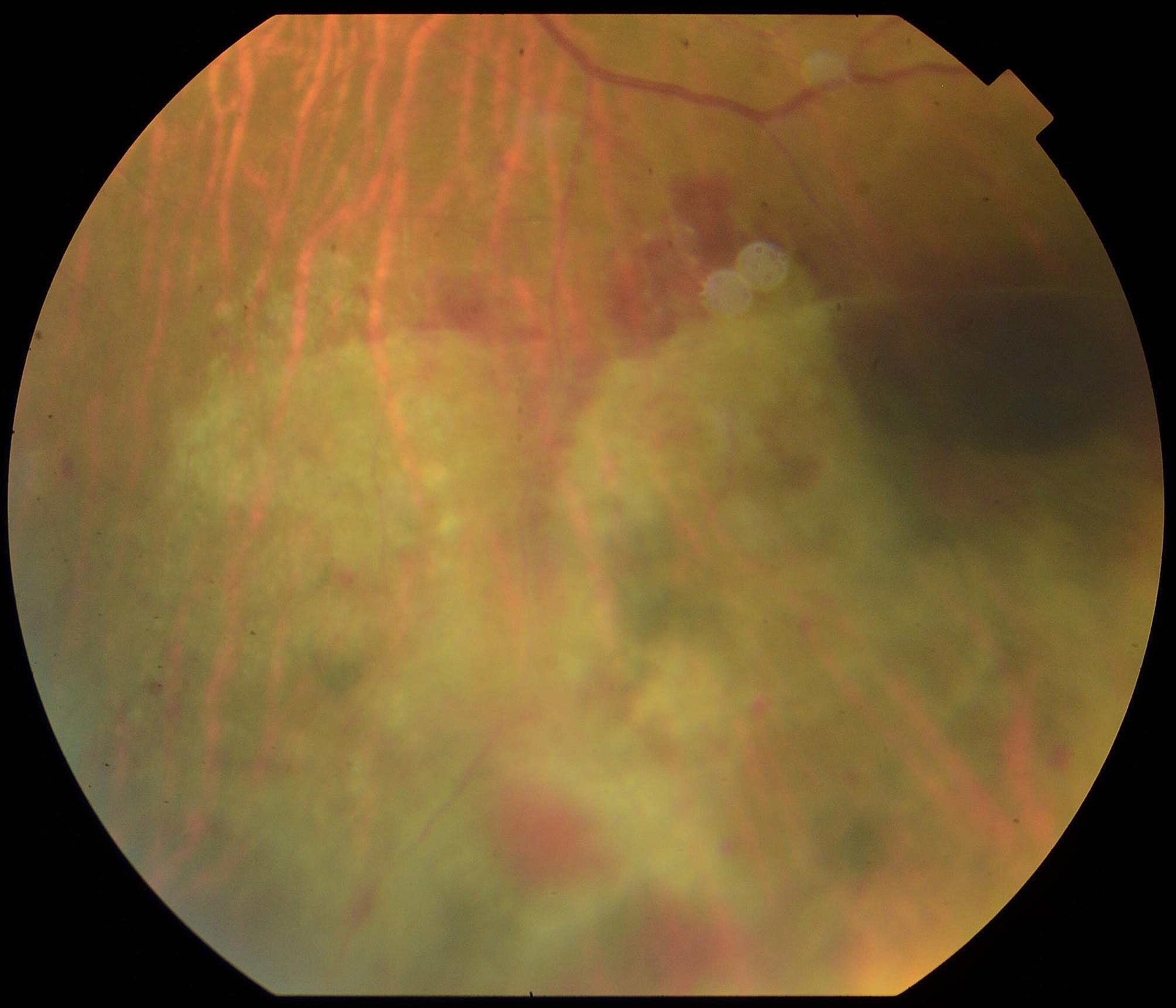
On initial examination, best-corrected visual acuity (BCVA) was 20/70 (Snellen visual acuity chart) in the left eye and light perception (LP) in the right eye. The intraocular pressure (IOP) was 38 mmHg in the left eye and 17 mmHg in the right eye. Slit-lamp examination revealed conjunctival hyperaemia, mutton-fat keratic precipitates in the middle and below the corneal endothelium, and 3 + flare in the anterior chamber in the left eye. The anterior segment of the right eye was quiet. Dilated fundus examination of the left eye showed mild vitritis, peripheral retinal whitening and mild retinal vasculitis. An exam of the right eye showed silicone tamponade in the vitreous cavity and extensive pre-retinal proliferation (Fig. 1). ARN in the left eye was presumed, and treatments including intravenous acyclovir (1500 mg/day), intravitreal injections of ganciclovir (3 mg) every four days and oral prednisolone were given.
Fig. 1
Bilateral ultra-wide field fundus photography taken at the onset of ARN in the left eye. A Silicone tamponade in the vitreous cavity, extensive pre-retinal proliferation and retinal scarring could be observed in the right eye. B Mild vitritis and peripheral retinal whitening could be observed in the left eye
To confirm the diagnosis of ARN and determine the causative virus, about 100μL aqueous humour was obtained through an aqueous tap. Real-time quantitative PCR (qPCR) of four common human herpes viruses (HSV, VZV, CMV, EBV) were performed. For qPCR, a mixture of about 20 μL intraocular fluid and 20 μL nucleic acid extraction liquid (NaCl + EDTA-Na2) was incubated at 99 °C for 10 min, then centrifuged at 13,000 rpm for 10 min. The recovered supernatant was used for qPCR assay using HSV (Z-SD-0017–02), VZV (Z-OD-0024–02), CMV (Z-OD-0022–02), and EBV (Z-OD-0023–02-25) real-time PCR kits (Liferiver, Shanghai, China), according to the manufacturer’s instructions. Immunoglobulin G (IgG) measurements of these four viruses were also conducted via enzyme-linked immunosorbent assay (ELISA). Four antibody detection kits, including ESR-105G (HSV1&2-IgG), ESR-104G (VZV-IgG), ESR-109G (CMV-IgG) and ESR-1361G (EB-VCA-IgG) (Institute Virion/Serion GmbH, Würzburg, Germany) were used according to the manufacturer’s instructions.
It was surprising that the results of qPCR for all four viruses were negative. We also did not find any increase in aqueous viral antibody levels. Fundus examination showed an apparent enlargement and integration of retinal lesions towards the posterior pole (Fig. 2). Taking the typical clinical characteristics into consideration, we insisted on the diagnosis of ARN in the left eye and postulated a false negative result from the qPCR. Antiviral treatment was continued. Another aqueous tap was performed on 24 January 2022, about one week after the first sampling, which showed positive HSV DNA load in the aqueous humour (7.25 × 103 copies/mL). Meanwhile, aqueous HSV-IgG was 1.93 U/mL. Despite initial enlargement, the necrotic retinal lesions diminished after intensive antiviral and anti-inflammation treatments (Fig. 2). The HSV DNA load in the aqueous humour was 2.49 × 105 copies/mL on 6 February 2022 and finally turned negative on 17 February 2022, about five weeks after the onset of disease. The level of HSV-IgG in the aqueous humour increased to 276.08 U/mL and 222.64 U/mL at these two time points. BCVA in the left eye was maintained at 20/30. The changes in BCVA, the HSV DNA load and the level of HSV-IgG in the aqueous humour are listed in Table 1.
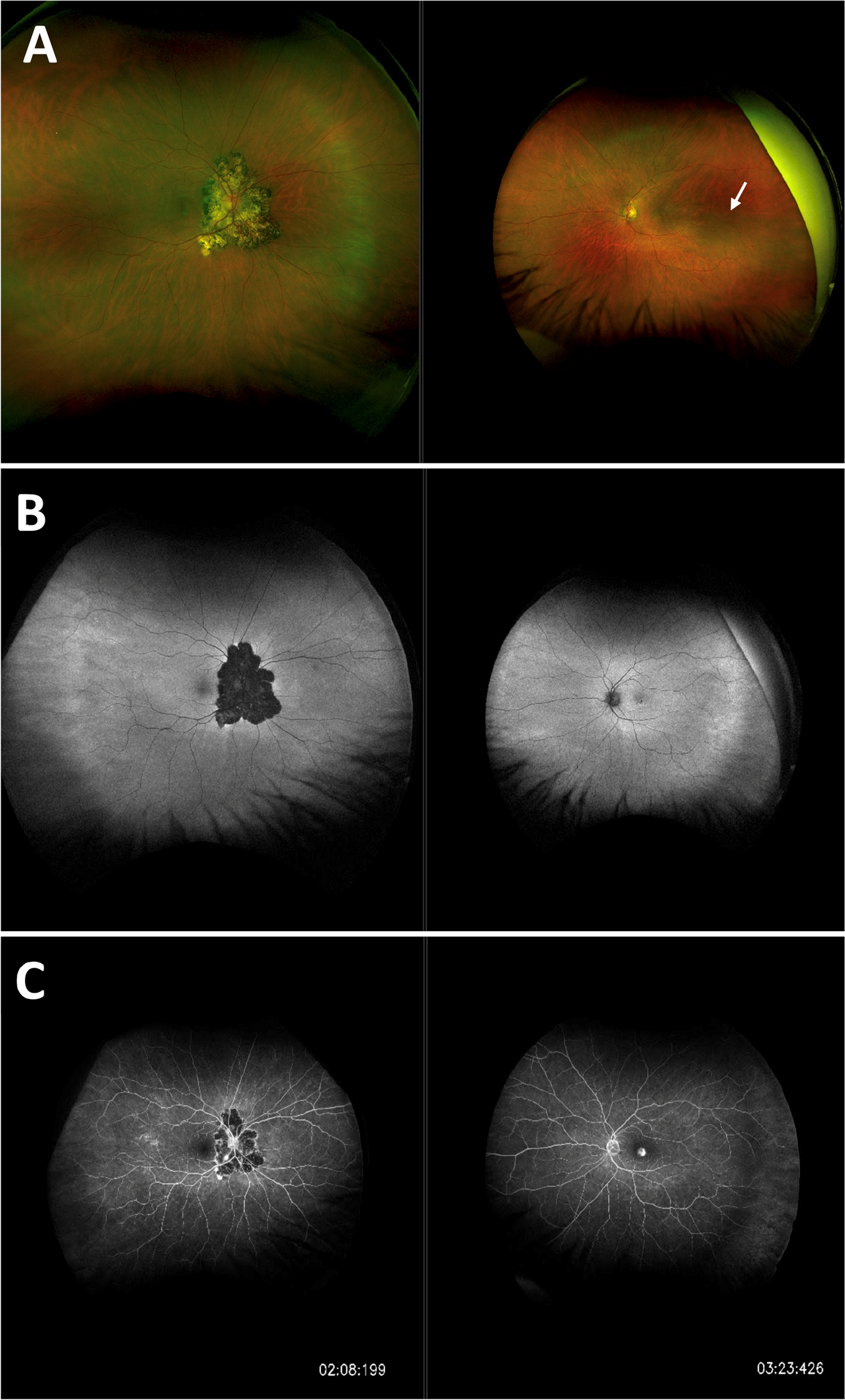
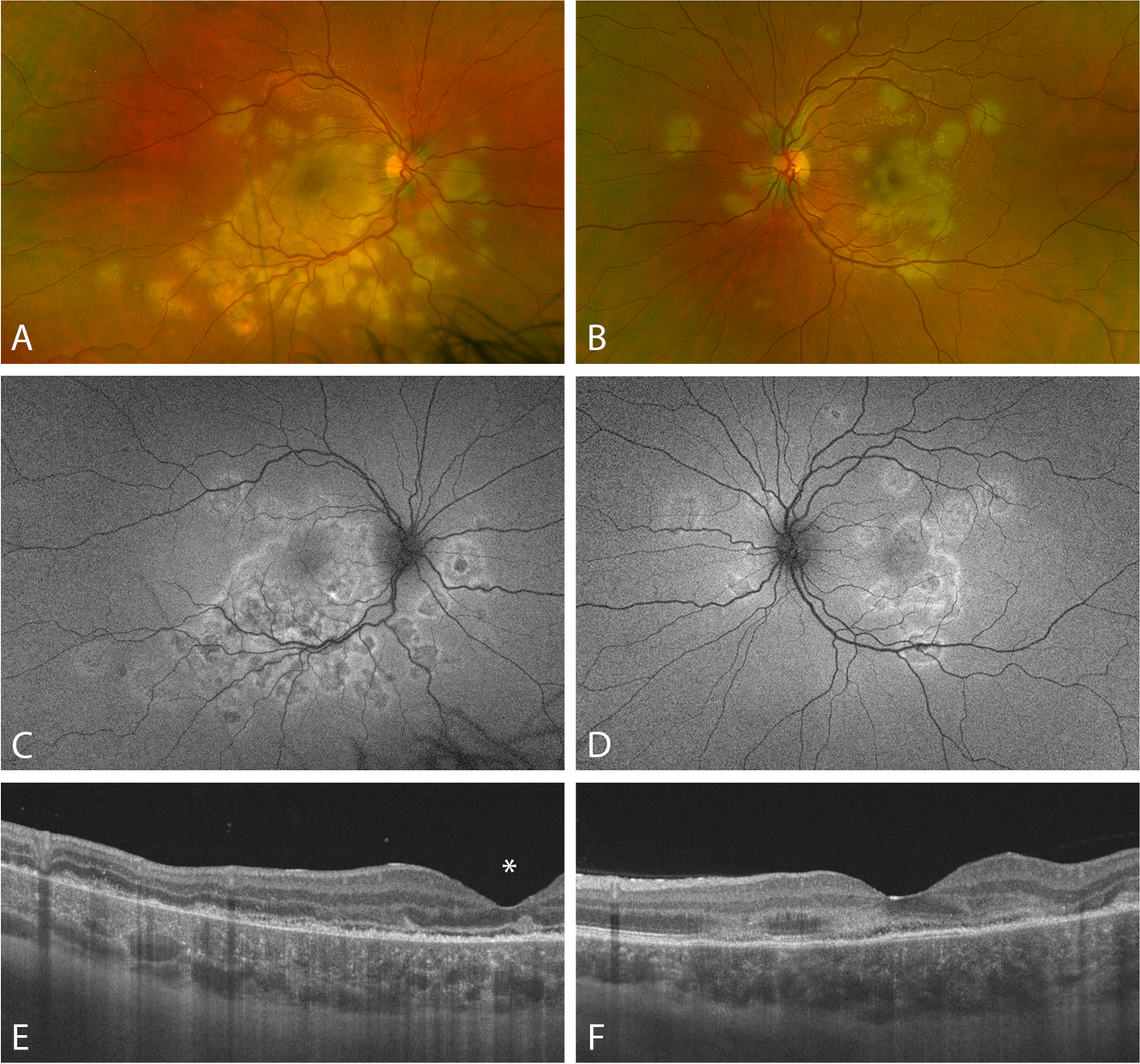
Fig. 2
Changes in retinal lesions in the process of ARN. First, the peripheral yellowish-white lesions enlarged quickly towards the posterior pole and then diminished gradually with intensive antiviral and anti-inflammation treatments. A Three days after the onset of ARN in the left eye. B Ten days after the onset of ARN in the left eye. HSV DNA load in the aqueous humour was 7.25 × 103 copies/mL at this time point. C Thirteen days after the onset of ARN in the left eye. D About 3 weeks after the onset of ARN in the left eye. HSV DNA load in the aqueous humour was 2.49 × 105 copies/mL at this time point. E About 5 weeks after the onset of ARN in the left eye. HSV DNA load in the aqueous humour turned negative at this time point. F Thirty-seven days after the onset of ARN in the left eye, which showed nearly complete disappearance of retinal lesions in fundus photography
Table 1 The variation of BCVA and the viral load of HSV in the aqueous humour
留言 (0)