
Remember me
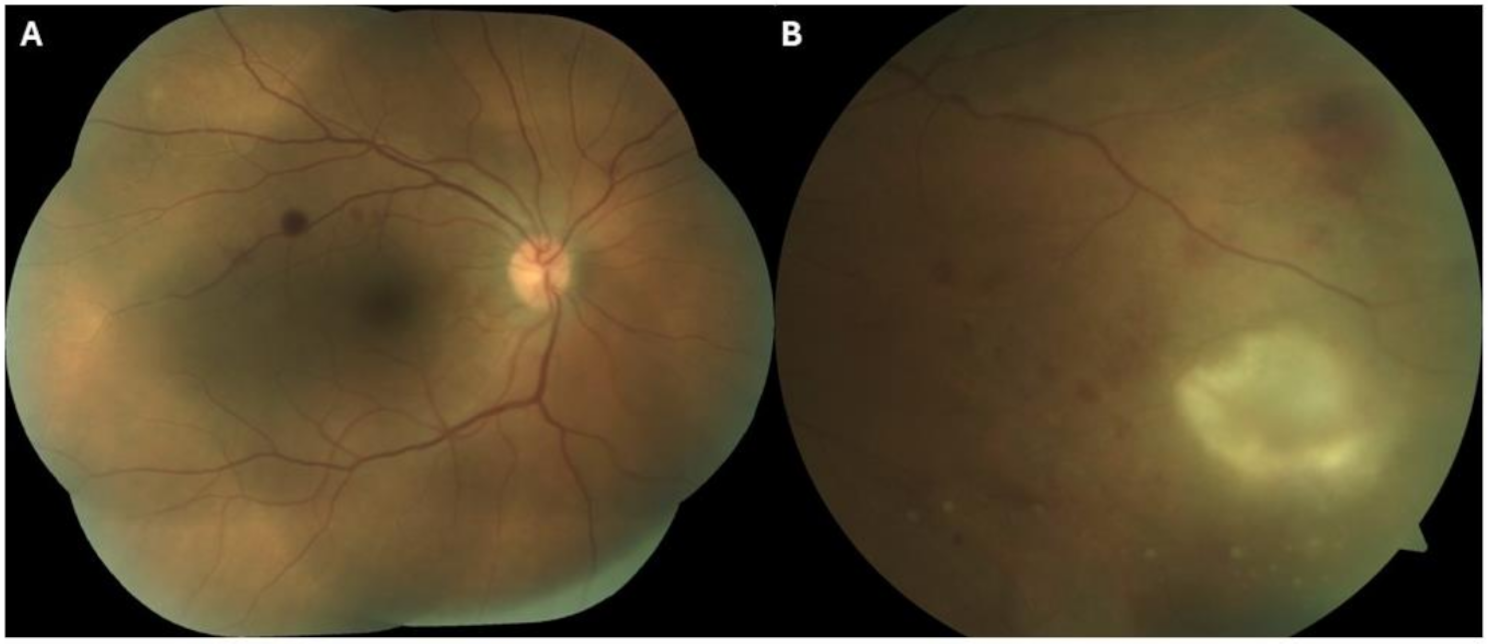




A 52-year-old female presented to the Eye Casualty complaining of a 4-week history of blurred vision in her left eye and a 2-week history of bilateral photosensitivity. On examination, best corrected visual acuity (BCVA) was 6/12 in the right eye and 6/24 in the left eye. Corneal exam was normal with no keratic precipitates. There was bilateral anterior uveitis with + 2 cells in the right eye and + 0.5 cells in the left eye. Intra-ocular pressure (IOP) was raised in the right eye at 40 mmHg and borderline at 19 mmHg in the left eye. There was no vitritis. Dilated fundoscopy revealed a large mottled area of chorioretinal pigmentation in the right eye centred around the optic nerve and a left macular haemorrhagic lesion suspicious for a CNVM (Fig. 1A).
Fig. 1
A: Optos ultra-widefield pseudocolour fundus image of both eyes showing mottled chorioretinal circumpapillary pigmentation in the right eye and macular haemorrhage in the left eye (white arrow). B: Fundus auto-fluorescence (FAF) of both eyes on initial presentation. C: Optos ultra-widefield fluoroscein angiography showing areas of mottled hyper- and hypofluorescence in the right eye and a central macular area of leakage in the left eye (late shots)
She reported previous treatment in Romania (a high TB burden country, with the highest rates of TB in the European Union [5]) several years earlier of an infective condition affecting her right retina requiring systemic antibiotic and steroid therapy for a 6-month period. No further details were available and she had no other ophthalmic history. There were no self-reported ophthalmic issues since treatment completion and she stated her baseline visual acuity prior to this presentation was normal in both eyes. She had a significant medical history of malignant mucosal melanoma diagnosed six months prior to this ophthalmic presentation. Biopsy confirmed a primary vaginal melanoma, nodular histological subtype, Clarke’s level 3, mitotic index 5/mm2, Breslow thickness 12mm with extensive ulceration and no adjacent lympho-vascular or perineural invasion. A staging positron emission tomography-computed tomography (PET-CT) performed at the time of diagnosis revealed a 3.8cm fluorodeoxyglucose (FDG) avid vaginal mass with a standardised uptake value (SUV) of 5.9 suggesting a malignant lesion. A complete vaginectomy was performed followed by pelvic radiation. Deep margins were positive on histology and the decision was made to initiate adjuvant immunotherapy with ipilimumab and nivolumab. She had completed her third cycle 6 days prior to this presentation. She had no other medical history apart from mild hypertension not requiring medication. She was a non-smoker with no alcohol or illicit drug use. She was of Romanian ethnicity but had been living in Ireland for many years. She reported travelling to Romania occasionally during her time living in Ireland to visit relatives but no known TB contacts. She worked in a restaurant and was married with one son.
Fundus autofluorescence (FAF) revealed the right retinal lesion to be inactive in appearance with no hyper-autofluorescence (Fig. 1B). Fundus fluorescein angiogram (FFA) showed a subfoveal area of leakage in the left eye compatible with an active CNVM (Fig. 1C). There was no evidence of vasculitis. Indocyanine green angiography (ICGA) revealed multiple hypofluorescent spots in the left eye (Fig. 2). No choroidal granulomas were visualised. Optical coherence tomography (OCT) images of her right eye showed peripapillary disruption of the outer retinal layers without fluid or secondary macular disturbance (Fig. 3A). OCT images of her left eye showed central intraretinal and subretinal fluid with loss of the normal foveal contour (Fig. 3B). She underwent a full uveitis blood investigation panel including Treponema Pallidum, Toxoplasma gondii, Toxocara canis, Herpes Simplex Virus, Varicella Zoster Virus, Cytomegalovirus and other autoimmune inflammatory conditions associated with posterior uveitis which were all negative. Aqueous and vitreous sampling was not performed.
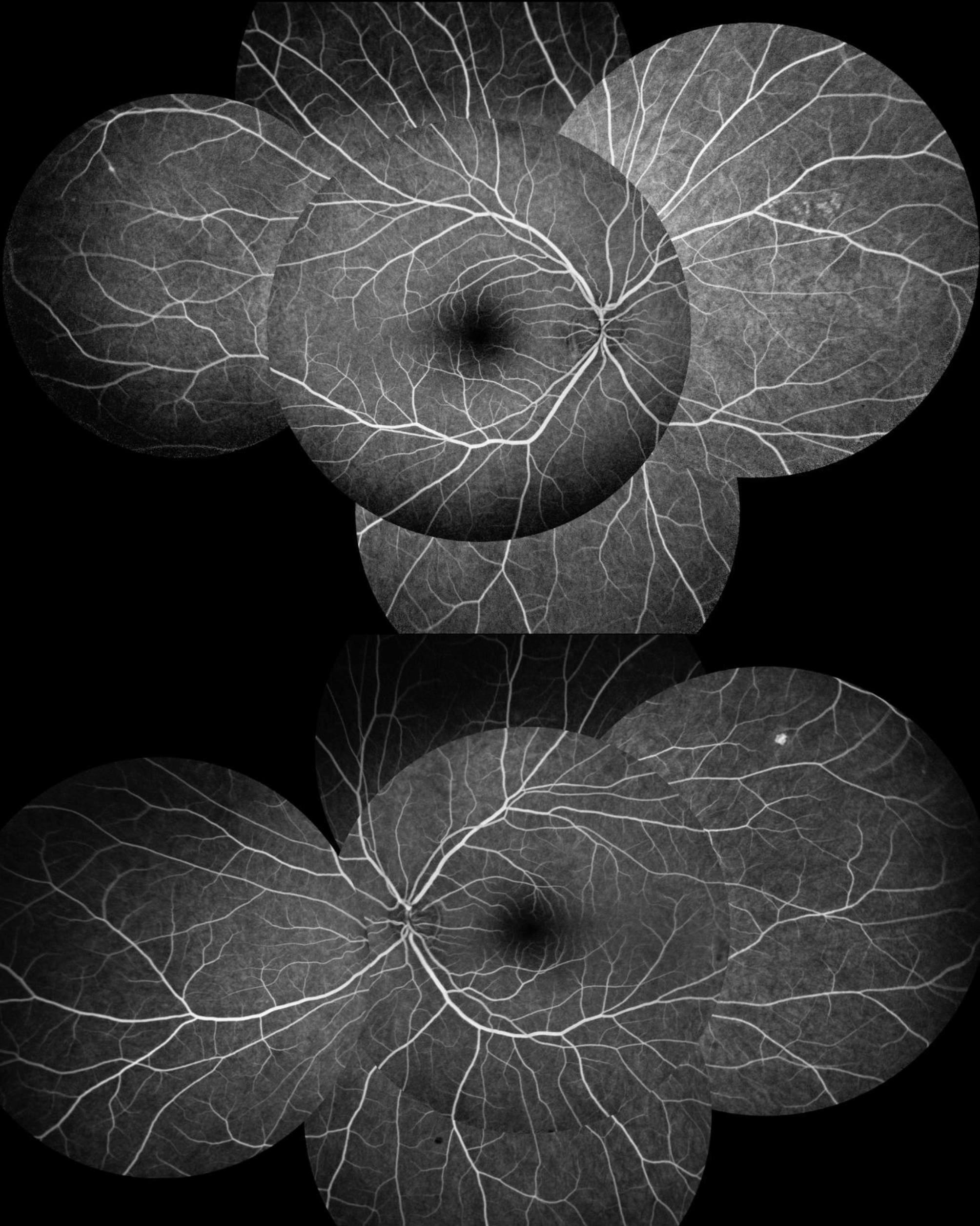
Fig. 2
Indocyanine green angiography (ICGA) images with multiple hypofluorescent dark dots (white triangles) in the left eye (late shots)
Fig. 3
A: Optical coherence tomography (OCT) image of right macula at presentation showing peripapillary disruption of all outer retinal layers with no associated fluid. B: OCT image of left macula at presentation showing intraretinal and subretinal foveal fluid with loss of normal foveal contour. C: OCT image of left macula six weeks post second intravitreal Bevacizumab showing resolution of fluid
Due to the quiescent serpiginous-like choroiditis (SLC) appearance of the right fundus, previously reported systemic treatment of a right eye infectious condition, growing up in a country with endemic TB, the presence of multiple choroidal lesions and an active CNVM, reactivation of latent TB in her left eye was suspected. She underwent a left eye intravitreal anti-VEGF Bevacizumab injection on the day of her presentation to target the CNVM. She was given a stat dose of Acetazolamide 250mg and was initiated on G Brinzolamide/Timolol and G Apraclonidine to her right eye to reduce IOP.
On discussion with her oncologist her fourth cycle of immunotherapy was postponed due to the development of ocular IRAEs and she was initiated on a tapering systemic regime of Prednisolone 1mg/kg over 8 weeks by the treating oncologist, on the assumption that this was likely an ICPI-induced uveitis. This was in conjunction with a topical steroid taper of G Pred Forte over a 6-week period to target the anterior chamber activity. Mediastinoscopy revealed a non-caseating granulomatous lymphadenitis, possible aetiologies including TB and sarcoidosis. Ancillary tests including Ziehl–Neelsen stain was negative, washout Auramine stain was negative and TB culture was negative. PCR testing with the GeneXpert MTB/RIF assay was positive for TB on endobronchial washout. A QuantiFERON-TB Gold blood test had been performed prior to ICPI initiation and again following this ophthalmic presentation and was reported as negative in both instances. It was deemed to have reduced sensitivity due to prior systemic immunosuppression with ICPI. On consultation with infectious disease specialists, she was initiated on systemic ATT within 1 week of her ocular presentation using rifampicin, isoniazid, pyrazinamide and moxifloxacin to cover for potential multi-drug-resistant tuberculosis given her ethnic background.
She underwent a second left eye intravitreal Bevacizumab 2-months later with an excellent response. On all subsequent eye examinations BCVA was maintained at 6/5 in both eyes, OCT remained dry (Fig. 3C) and she had no evidence of uveitis. Her right fundal lesion remained unchanged (Fig. 4). She was recommenced on a fourth cycle of immunotherapy two months after the development of her uveitis without ocular sequelae.
Fig. 4
Optos wide-field pseudocolour image of both eyes following completion of anti-VEGF and systemic anti-TB therapy with resolution of left macular haemorrhage
Unfortunately, a repeat staging PET-CT scan performed three months after her presentation to the Eye Casualty revealed disseminated metastatic disease. The ATT was tolerated well initially, however, four months into treatment she developed jaundice with grossly deranged liver function tests (ALT 1569, GGT 105, ALP 126, bilirubin 70). A liver ultrasound confirmed multiple large liver metastasis with central necrosis. ATT was discontinued prematurely due to the potential risk of fulminant hepatitis with isoniazid. She was discharged to community palliative care and passed away within one year of her diagnosis.
Comments (0)