Bechet’s disease is a multisystemic inflammatory disorder characterized by diverse manifestations including recurrent oral and genital ulcers, ocular inflammation, and skin lesions. TNF inhibitors have emerged as a therapeutic option for refractory BD, providing symptom relief and reducing disease activity [2,3,4,5,6,7]. Despite the benefits of TNF inhibitors in BD, the risk of TB is a most significant concern, especially in endemic country including Japan. TNF inhibitors suppress the immune response, potentially increasing the risk of reactivation of latent TB infection or new TB infection. Several case reports and observational studies have reported TB as an adverse drug reaction in patients receiving TNF inhibitors for BD treatment [8, 9]. On the other hand, restarting TNF inhibitors in patients who developed TB as a complication of previous TNF inhibitor use has been reported in fields other than ophthalmology [11, 12]. In one study, of 16 patients who resumed biological agents after development of TB under anti-TNF therapy, one patient with Behcet's disease resumed TNF inhibitors [13], but there are no reports detailing the clinical course of TNF inhibitor resumption after completion of TB treatment in patients with Behcet's disease or other refractory uveitis.
Compared to other immune suppressive therapy, TNF inhibitors have a higher risk of TB [14]. Details of the mechanism by which TNF inhibitors increase the risk of developing TB are not fully understood. Monocyte-derived macrophages (MDM) are activated by TNF-α secreted by TB-infected MDM [15]. The activated macrophages kill TB or isolate it by granuloma formation. TNF gene-deficient mice that do not form granulomas are highly susceptible to TB, [16] suggesting that TNF inhibitors are associated with a higher risk of developing TB. Moreover, membrane TNF expressed by activated macrophages and T lymphocytes is essential for protection against TB infection [17, 18], as a difference in the incidence of TB has been observed between infliximab (an anti-TNF monoclonal antibody) and etanercept (soluble TNF receptor fusion molecule) [19, 20]. Studies have reported that TNF inhibitors suppress the proliferation of TB-specific T cells and the production of IFN and IL-1, which in turn suppress TB-specific T cells and increase the risk of developing TB [18, 21, 22]. Therefore, TB screening before starting TNF inhibitor is necessary, using chest X-ray, TST or interferon-γ release assays (IGRAs) such as QuantiFERON-TB Gold In-Tube (QFT-GIT) and T-SPOT.TB [23, 24].
False negative result of TST may occur due to cutaneous allergy, recent TB infection, recent live virus vaccination (measles, mumps, polio), or improper test administration [25]. Advanced age and low number of lymphocytes are risk factors of false negative result of IGRAs [26]. While some reports indicate an association between steroid use and negative or indeterminate QFT-GIT, [27, 28] others show no statistically significant association between steroid use and negative or indeterminate T-SPOT.TB [28, 29]. Our patient was receiving PSL before being referred to our hospital. We cannot rule out the possibility that use of PSL in the present case may have resulted in false negative result in TST and T-SPOT.TB at presentation. On the other hand, the number of TB cases is high in the Asian and African regions. Unfortunately, the incidence of TB in Japan is not low [30]. Health care workers in contact with patients are at higher risk of TB infection than those with no patient contact [31]. Our patient was a radiologist. There is a possibility that our patient had frequent contact with TB-positive patients in the course of his work. It is unclear whether TB was not diagnosed at presentation to our facility because of false-negative results due to PSL, or whether he developed TB through contact with a TB patient after the initiation of ADA.
Patients with active TB that developed after TNF inhibitor therapy should stop all immunosuppressive medications and immediately receive appropriate treatment for TB [32, 33]. Resuming TNF inhibitor is recommended after 2 to 4 weeks of isoniazid if there are no signs or symptoms of active TB [12]. If active TB is present, restarting TNF inhibitors is recommended after 3–4 months of TB treatment [34]. Six of 13 patients who developed TB during TNF inhibitor therapy had no TB recurrence by resuming TNF inhibitor after TB treatment; four restarted TNF inhibitor within 2 months after TB treatment and two restarted after completion of TB treatment [11]. Therefore, resuming TNF inhibitors after completion of TB treatment is considered safe. While early resumption of TNF inhibitors has been shown to prevent worsening of inflammatory disease, there is a report of TB recurrence in 2 of 30 patients who resumed TNF inhibitors after TB treatment [35].
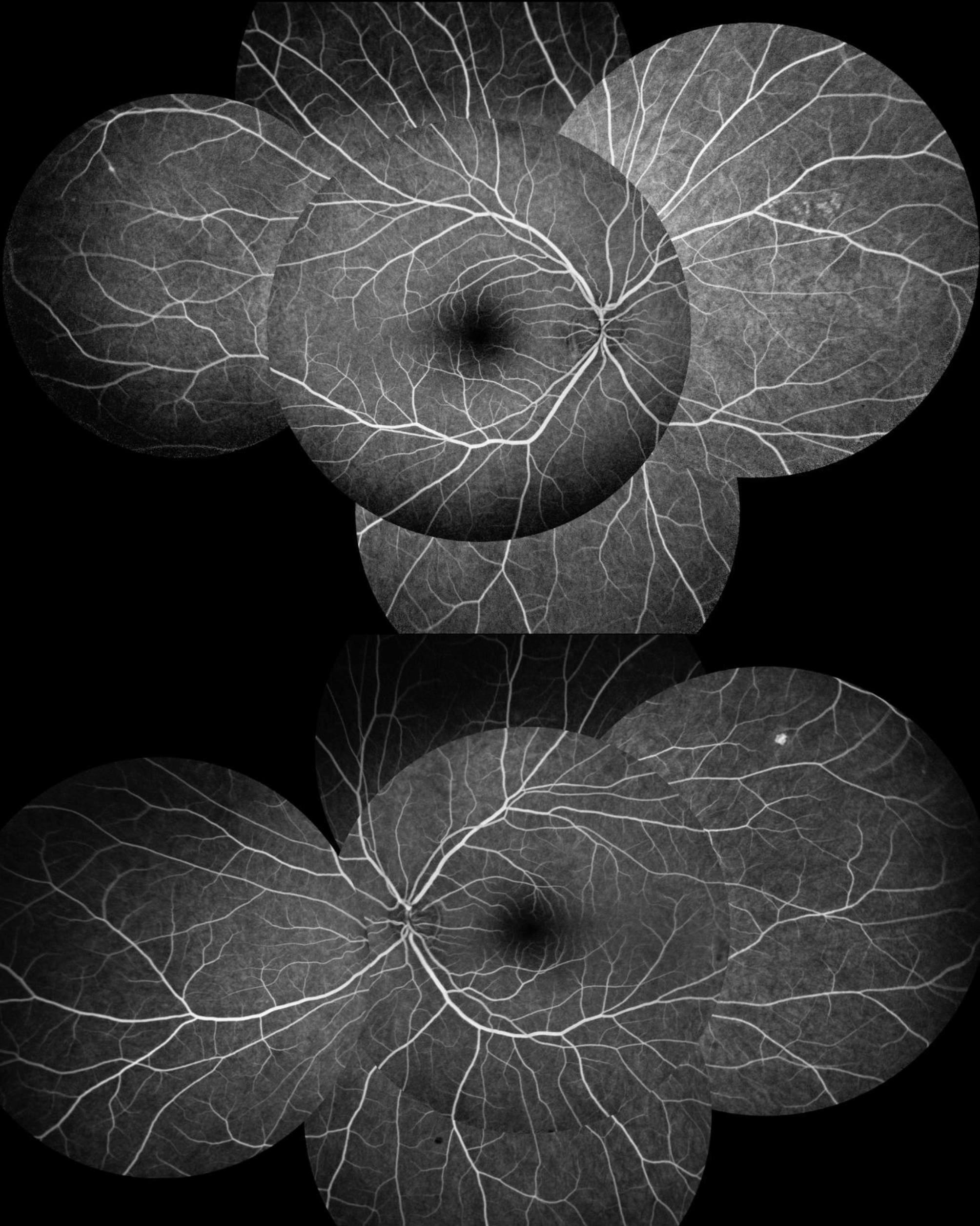
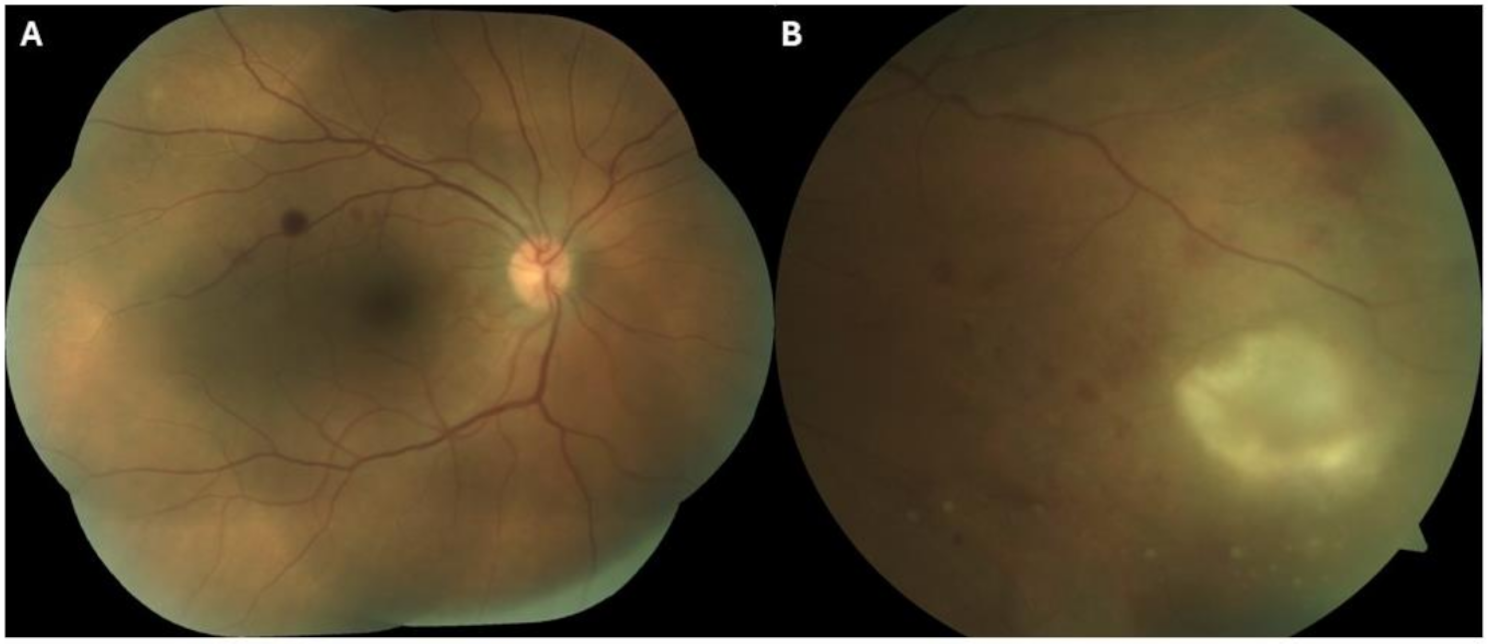
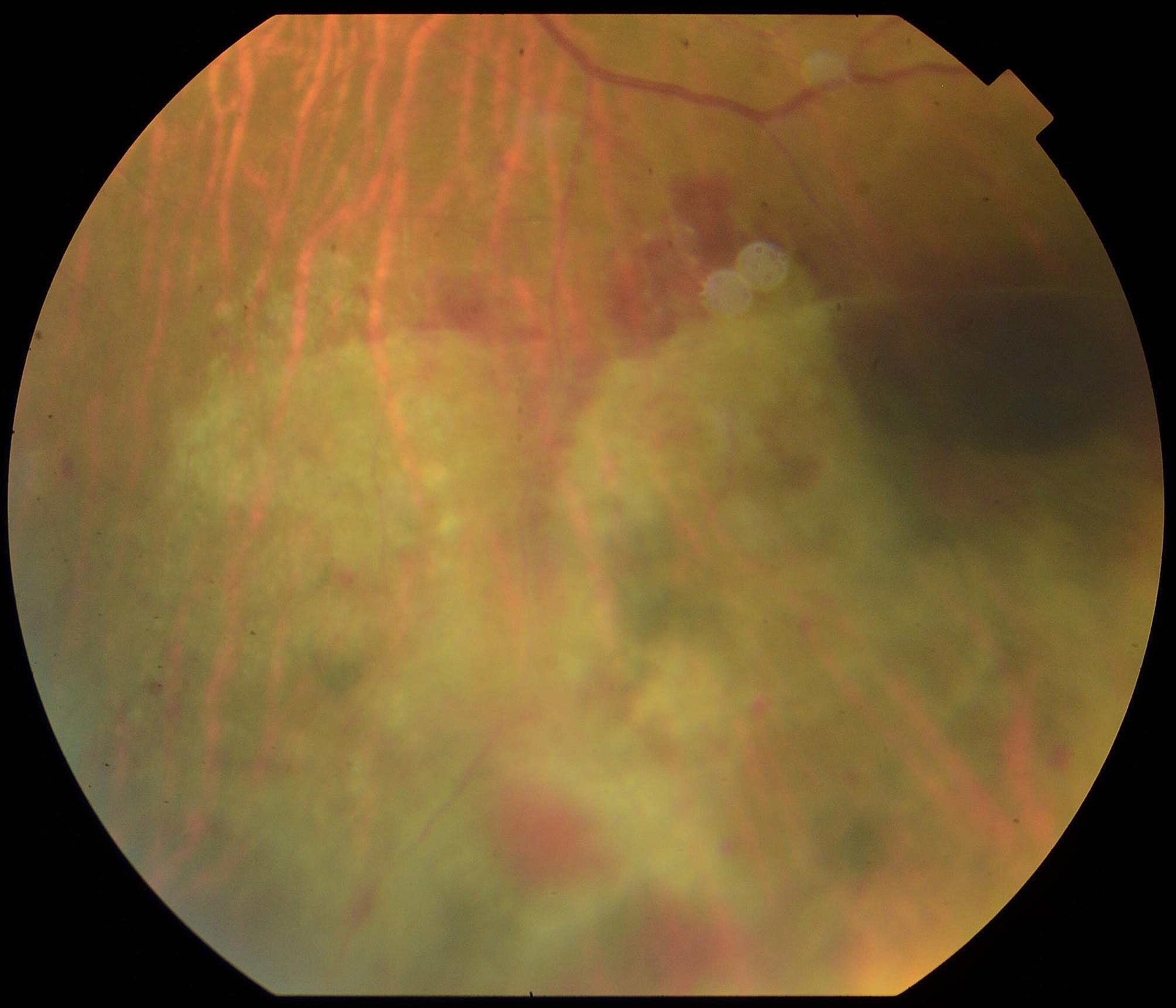
In the current case, during the period when ADA was discontinued, BCVA, vitreous opacity and ME in the left eye worsened and intraocular pressure increased despite sub-Tenon's injection of triamcinolone acetonide. Fluorescent leakage may have been mildly reduced by PSL at the time of presentation, but fluorescent funduscopic examination after discontinuing of TNF inhibitor showed a higher degree of fluorescent leakage than that at presentation. Worsening of fluorescent leakage compared to that at presentation is likely due to barrier damage in retinal vessels as a result of prolonged period of no TNF inhibitor treatment, or fluorescence leakage at the initial examination may have been slightly masked because the patient was on prednisolone at presentation. Nevertheless, additional anti-inflammatory treatment was essential in this case. Therefore, the clinical decision was to restart anti-TNF therapy using IFX because the patient needed immediate improvement of inflammation and oral PSL was not appropriate due to Behcet's disease. Among TNF inhibitors, etanercept has been reported to have the lowest risk of TB reactivation, [36] but there are reported cases of BD with TB relapsing while on etanercept [13]. In our patient, we selected infliximab to resume anti-TNF therapy because the patient needed immediate improvement. On the other hand, TB has high recurrence rate, and TB recurrence in 2 of 30 patients who resumed TNF inhibitors after TB treatment has been reported [35]. In our patient, isoniazid (300 mg/day) was given as prophylaxis for TB recurrence, because TSPOT.TB remained positive even after completion of TB treatment and the patient was likely to be exposed to TB patients due to his occupation as a radiologist. Isoniazid prophylaxis is scheduled to be continued at least until T-SPOT.TB is confirmed negative. After resuming TNF inhibitor, the patient had a good clinical course with improving BCVA, vitreous opacity, ME in the left eye and no recurrence of TB. Currently, there are no clear criteria for resuming TNF inhibitors, as it depends on the underlying disease, severity of TB, and availability of other alternative therapies. There is a need to accumulate case reports of patients who were able to resume TNF inhibitors, such as the present case, and to develop resumption criteria.





Comments (0)