The present theoretical dosimetric study provides a first comprehensive analysis of replacing Lu-177 with Tb-161 for two commonly used, registered radiopharmaceuticals. Although the differences in individual properties are small between these two isotopes, the aggregate of these differences mean that a 27–29% lower activity of Tb-161 is required to achieve the same delivered dose to target- and non-target tissue compared to Lu-177.
These theoretical considerations are roughly in line with the results reported by Baum et al., although the dose we found was slightly lower (Baum et al. reported kidney absorbed doses of 0.8 and 1.5 Gy/GBq, respectively, in two patients using [161Tb]Tb-DOTATOC, whereas we found 0.73 Gy/GBq using [161Tb]Tb-DOTATATE)—this may be caused by kinetic differences between the somatostatin receptor targeting tracers DOTATATE analysed in the present report vs. DOTATOC as used by Baum et al. [1], but more likely the larger difference with one of the two patients reported by Baum et al. was caused by the renal impairment which the particular patient was suffering from.
The major weakness of the present study concerns its theoretical nature. As Tb-161 is yet to be used in larger scale prospective studies, direct measurements of [161Tb]Tb-DOTATATE and [161Tb]Tb-PSMA-617 kinetics are as yet not available. However, considering the similar half-life of both isotopes and very similar chemical properties, there is little reason to suspect that both the biological kinetics and the rates of radiolysis will be markedly different. Although of course future prospective patient studies will have to confirm the present calculations, we nonetheless believe that the present analysis is robust enough to at least serve as a starting point for possible future prospective activity-finding phase 1 studies of [161Tb]Tb-DOTATATE and [161Tb]Tb-PSMA-617. Certainly, the agreement between the results of the same radiometal substitution between two different tracers (DOTATATE and PSMA-617) is also a strong argument to assume that the calculations here will also be valid for such similar tracers.
In theory, differences in systemic physiologic uptake between Lutetium and Terbium could cause additional differences in non-target uptake. However, ionic Lutetium and Terbium follow comparable systemic distribution patterns; uptake in skeleton and liver, as the other lanthanides [8]. Therefore, marginal difference in absorbed dose is to be expected from Tb-161 or Lu-177 coming free from the chelator.
To the best of our knowledge, Lu-177 and Tb-161 labeled tracers have not yet been compared preclinically or clinically. The principle of comparison employed in this study has been routinely used for other radiotracers, such as for the substitution of [111In]In-octreotide by [177Lu]Lu-DOTATATE [5]. The same method of substitution assuming equality of distribution was previously already published for [177Lu]Lu-PSMA-617 and the same tracer labelled with other radionuclides such Y-90 or Ac-225 [2]. Furthermore, in work employing the very similar tracer DOTATOC as well as the functional somatostatin receptor antagonist, Borgna et al. were able to show employing simultaneous dual-isotope SPECT that in a xenograft animal model both isotopes were interchangeable without affecting chemical and pharmacokinetic properties of the labelled tracer [9].
The present work primarily explores the activities of Lu-177 and Tb-161 which yield an equivalent non-target exposure and illustrate the effect on tumour doses based on a hypothetical example. The effect of substitution of these isotopes on a microscopic intratumoural level is beyond the scope of the present brief report but has been explored before by Bernhardt et al. [2].
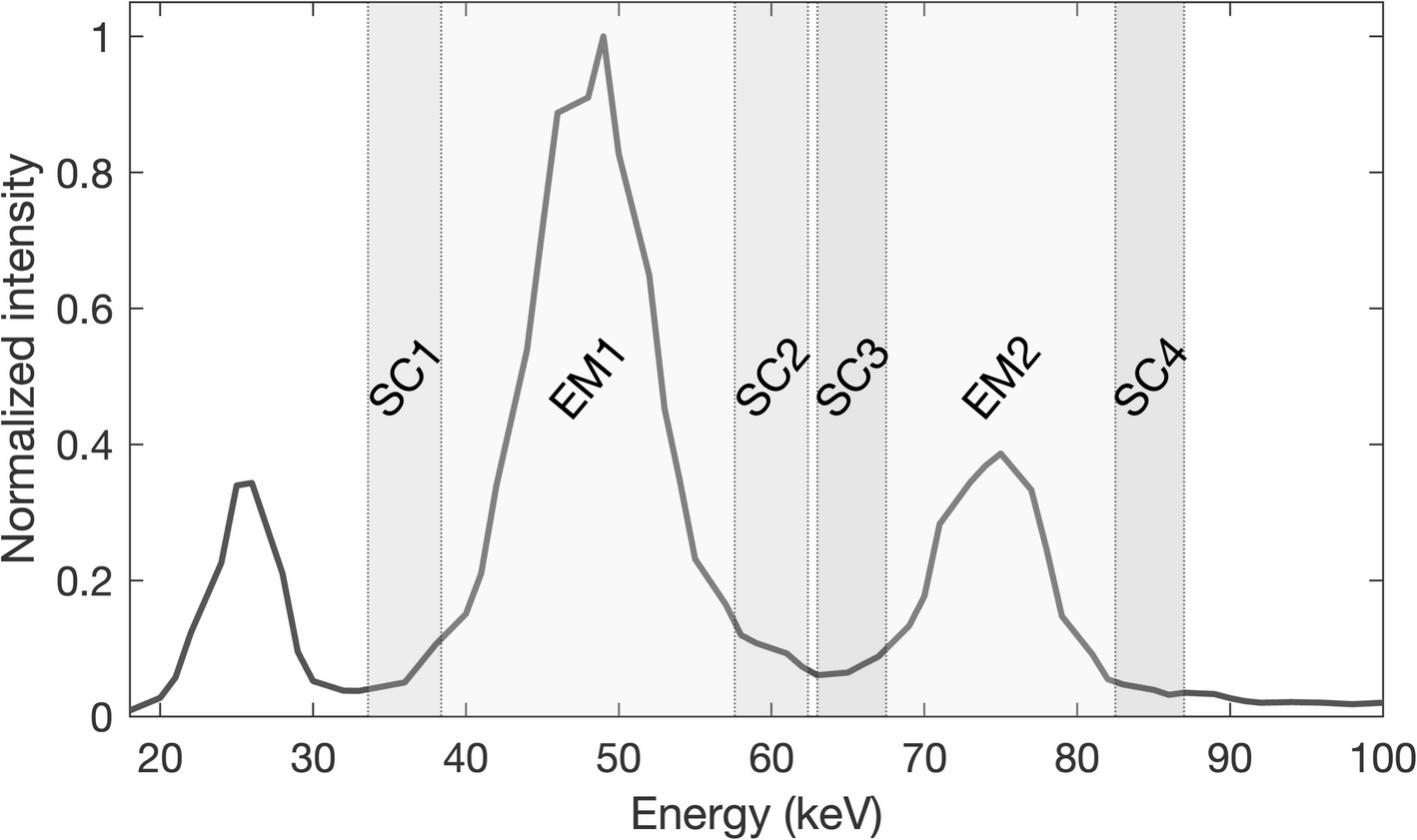
A major hurdle for TRT in many countries are aspects related to radiation protection. The use of Tb-161, of which the gamma-spectrum with peaks at 43.1 keV and 74.6 keV is much more favourable in terms of radiation protection than Lu-177 with peaks at 112.9 and 208.4 keV. The lower total activity necessary to achieve the same target absorbed dose will further increase the possibility of performing TRT as an outpatient procedure.
In radiochemical terms, a lower total activity is of distinct advantage as this will improve the radiochemical stability—generally speaking, the higher the activity, the higher the rate of radiolysis.
Furthermore, a lower activity in the presently studied substitution will also result in a lower total amount of radioactive atoms required for labelling, which in turn may lead to a reduction in the total amount of precursor used. Especially in the case of the tracer DOTATATE, where clinically relevant pharmacological effects of the tracer are occasionally observed [10], a reduction of the total dose of substance used may lower the incidence of side-effects of therapy and may thus further improve the radionuclide therapy experience for the patient.
Of course, although the present results look promising for Tb-161, the supply of Tb-161 as yet is still even more fragile than Lu-177. Production and supply quality of Tb-161 needs to be scaled up, standardized and in GMP-quality.
In summary, the above results show that from a dosimetrical point of view, substitution of Lu-177 by Tb-161 is feasible, although an activity conversion needs to be applied in order not to exceed dose limits to critical non-target organs—however, this conversion may be of both radiochemical and clinical advantage. Preclinical and clinical studies to confirm these results to establish the safety and effectiveness of Tb-161 TRT are urgently needed.





Comments (0)