
Remember me




Patient data was acquired from research imaging studies investigating tumour hypoxia in non-small cell lung cancer (NSCLC) of adult patients using 4D \(^\hbox\)-fluoromisonidazole (\(^\hbox\)-FMISO) PET/CT (e.g. ATOM, [22]) at the Churchill Hospital Oxford. Patients were injected with an activity of 370 MBq ± 10% of \(^\hbox\)-FMISO (University of Cambridge, Cambridge, England, United Kingdom) prior to imaging. 4DCT images (six gates) were obtained in the studies to calculate the extent of respiratory motion.
In this study, patients are deemed evaluable via the R-value, used to determine whether to use PET respiratory gating [11]. Patients \(\text>12\) were included in this study (\(\text=18\)), details in Table 1.
Table 1 Table detailing R-value distributions throughout the patient cohortA lower R threshold was used (R > 15 is typically used clinically) to maximise the available dataset. The R-value of patients included varied from 12.1 to 25.8 with a mean value, \(\bar = 15.8\).
Image acquisition and reconstructionsThe image datasets were acquired using a Discovery D710 PET scanner (GE HealthCare). The field-of-view (FOV) comprised a single bed position from the superior thorax to the superior abdomen, imaging the lung, heart and liver. Patients were scanned using 10-minute PET acquisitions, two and four hours following \(^\hbox\)-FMISO injection [22]. The PET data in this study was corrected for motion using the manufacturer’s DDG-based MotionFree [4, 11].
The 4DCT images were generated using an external Real-time Position \(\hbox^}\) (RPM) device, secured on the patient’s abdomen. The 4DCTs were conducted under free-breathing conditions where patients were advised to maintain regular breathing, if possible. The static \(\hbox_}\) is automatically initiated 30 s after 4DCT acquisition, also under free-breathing conditions. The 4DCT data was acquired as a series of 4 cm axial-width cine CTs (across the PET axial FOV) then binned into six gates using MotionMatch (GE HealthCare) without any user-guided improvement from default to determine the gates. A single series over six phases or gates were saved, encompassing the entire regular patient respiratory cycle from end-of-inspiration (EI) of one cycle to EI of the next cycle, across the six gates. This binning ensured that the investigated EE phase was entirely acquired.
Motion match algorithmThe warped motion-matched PET/CT reconstructions were performed using an offline reconstruction package, Duetto (GE HealthCare toolbox in MATLAB), which is part of a research agreement and not an available product. To create the warped CT, the MM algorithm must first approximate the initial phase within the respiratory cycle that \(\hbox_}\) was acquired.
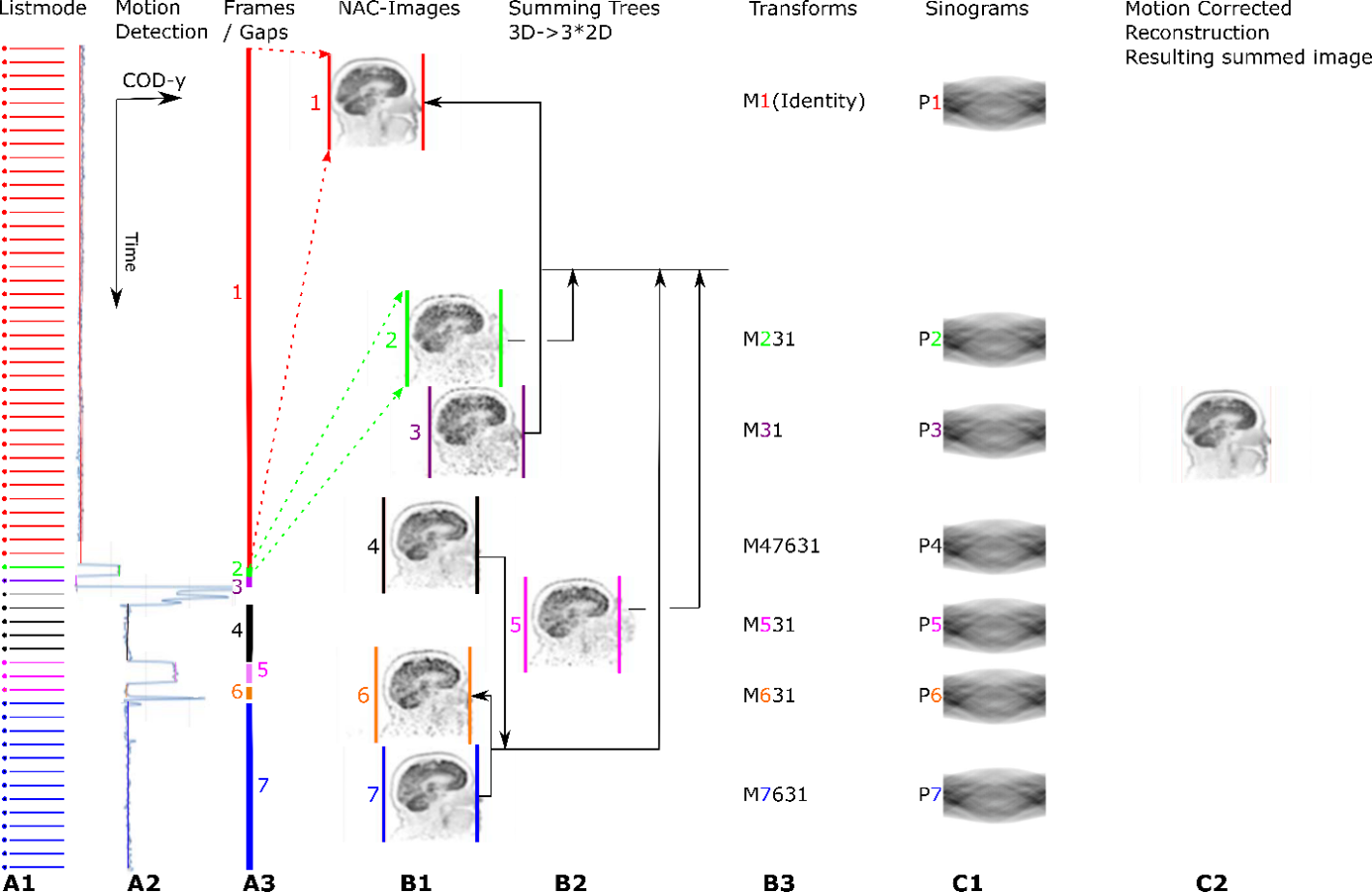
The MM algorithm uses an adaptation of the manufacturer’s Bayesian penalized likelihood (PL) reconstruction algorithm (\(\beta = 350\)), Q.Clear, a non-ToF BSREM algorithm without attenuation correction information for motion estimation (number of reconstruction voxels in the x–y dimension, \(\hbox = 64\), \(\hbox = 70\) cm) [23]. A ToF BSREM algorithm was used to reconsruct the final MM corrected images. The algorithm’s workflow is indicated in Fig. 1.
Fig. 1
Flowchart outlining MMCT algorithm workflow
The three-bin gated PET images and respiratory waveforms were extracted directly from the listmode and raw data files using principal component analysis (PCA) allowing for respiratory motion model generation.
Three bins are selected for comprehensive coverage of each phase of the respiratory cycle. An essential difference between the 4DCT and MMCT is the binning method; the 4DCT uses phase-based binning, whereas MMCT uses amplitude-based binning. Phase-based binning assigns the breathing cycle over \(2\pi\) radians [24]. Amplitude-based gating is based upon the division of the respiratory signal with respect to the magnitude of the patients’ respiratory motion [25]. EE and EI of each respiratory cycle are defined by amplitude-based gating scales as 0% amplitude and 100% amplitude, respectively. Amplitude-based gating of PET was used over phase-based gating due to improved determination of the quiescent phase in patients with irregular breathing patterns by using respiratory triggers and waveform geometry [26, 27].
The deformation fields across different gates of the PET data were estimated using the manufacturer’s Q.Freeze2 algorithm [12].
The motion model was established by assuming a linear relationship between respiratory phases and deformation amongst gates. This model allows generation of PET images at any target phase, where 28 PET images at equally sampled phases between 0 and 200% were generated. The phase range was extended to 200% to overcome the fact that patients can sometimes inhale deeper but rarely exhale deeper in CT acquisition compared to PET.
Using the deformation field amongst gates to warp PET images into any arbitrary phases enables the estimation of a CT phase by maximising mutual information between the warped PET and PET Image For Attenuation (PIFA) data, where PIFAs are 511 keV attenuation coefficient images converted from CT.
Following CT phase estimation, new warped PIFAs and subsequent CT DICOMs can be generated for any desired target phase of the respiratory cycle based on the motion model estimated from PET.
These warped images can then be used for the CTAC in PET reconstructions, reducing the extent of misregistration in PET/CT with scope for improvements in PET quantification.
Analysis of CT imagesThe end-of-expiration (EE) phase is subject to minimal motion compared to other parts of the respiratory cycle, as seen in Fig. 2.
Fig. 2
Schematic illustrating typical respiratory waveform, with EI and EE segments for the first waveform marked
In order to determine the differences between the CTs used for CTAC, multiple methods could be implemented to assess the respective differences. In this work, the EE phase of the 4DCT will be treated as the ground truth and compared to \(\hbox_}\) (an image acquired within an arbitrary phase of the respiratory cycle) and the EE phase of morphed MMCT (derived from \(\hbox_}\) using Duetto). Due to the differences in amplitude and phase-based gating, the EE phase is consistent between each gating method. In addition, it is the phase generally used when correcting for respiratory motion in reconstructing a quiescent phase PET/CT image.
Reconstructed CT images were analysed in Affinity (Hermes Medical Solutions) and measurements of different anatomical markers were taken to determine the differences between the CTACs. These measurements were taken for each exam of the liver and lesions, as these are key indicators of motion throughout the patient’s respiratory cycle. The relevant anatomical measurements to determine displacement are:
(a)Superior liver margin to bottom image boundary
(b)Superior lesion margin to top image boundary
(c)Inferior lesion margin to top image boundary
An example of these measurements is given in Fig. 3.
Fig. 3
CT image illustrating displacement measurement of the superior liver to inferior image boundary, representing measurement (a)
Statistical analysisThe raw data collected has a non-normal distribution due to inter-variability between patient’s unique disease burden and anatomy. To improve consistency across all patients, data for the various investigative parameters was collected as a percentage change relative to the result acquired for a particular group, i.e. 4DCT or \(\hbox_}\) for CTAC comparisons. This results in more normally distributed data. These corrections improve accuracy and validity in the statistical tests used during analysis, where parametric tests are used. Data normality is assessed by using the Shapiro-Wilk test, best suited due to the small sample size of respective datasets.
Given the normal data distribution upon transformation into percentage change, the parametric, repeated-measures, one-way, ANOVA is used to test for differences within the dataset due to comparison of three or more groups.
From the given results, the null hypothesis can be rejected for significance values of \(\it p \le 0.05\) and accepted for values \(\it p > 0.05\). For cases with a sphericity violation, as per the Mauchly test, a Greenhouse-Geisser correction was considered before concluding any significant results. Where results were deemed significant, post hoc analysis was completed using paired t-tests between groups.
For comparison of multiple groups, significance levels are adjusted using Bonferroni corrections, so any value \(p \le 0.05\) can be deemed statistically significant. Analysis was conducted using SPSS v29.
Comments (0)