Selection of sources of evidence
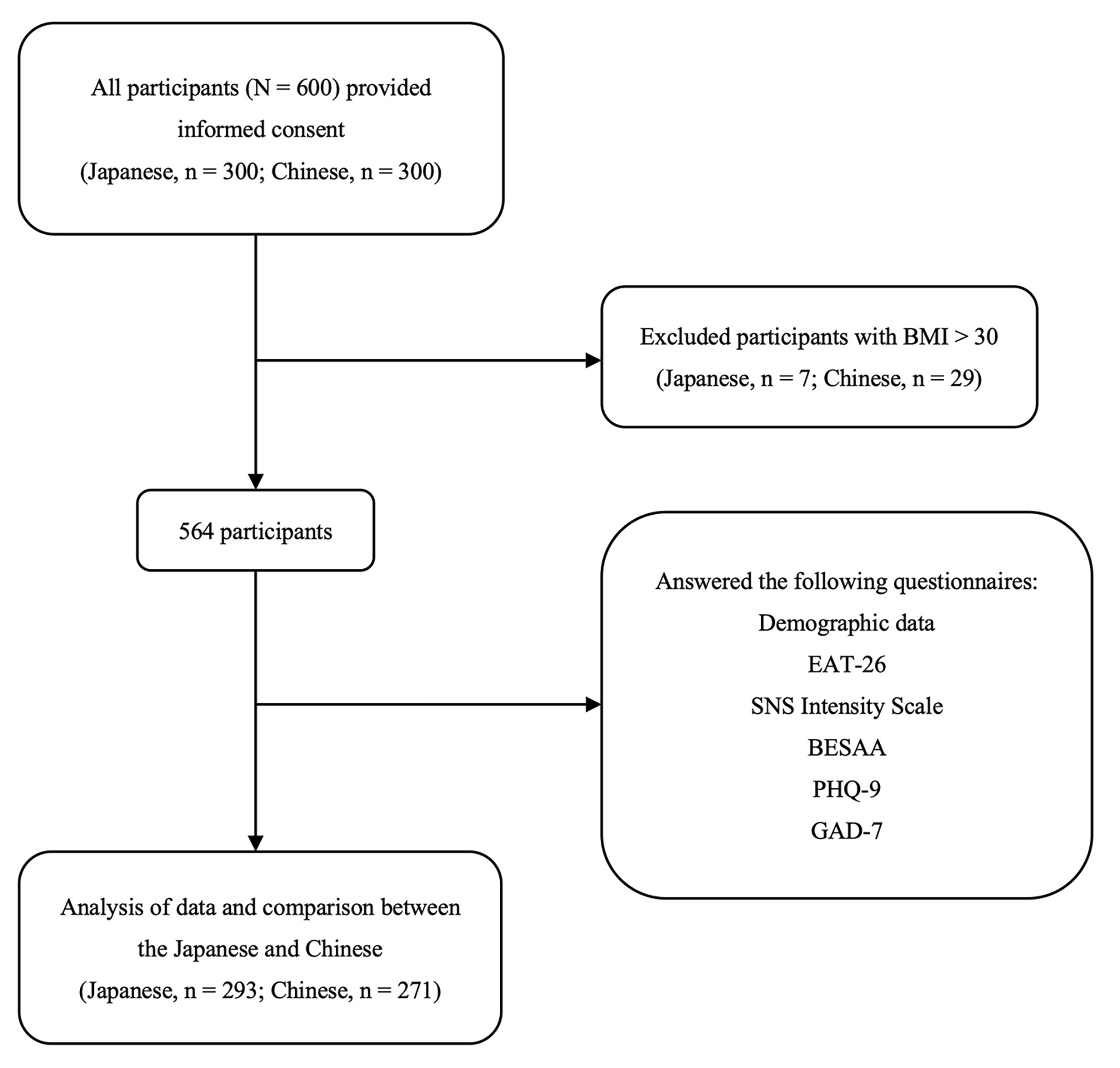
The source search in the electronic bibliographic databases retrieved 2596 records (2130 on PubMed/Medline and 466 on PsycINFO) (see Fig. 2). After removing 301 duplicate records, 2295 records were screened in the first screening step. During this first screening step, for each of the 2295 articles, the inclusion criteria described in the Eligibility criteria section of the Methods section were applied to both titles and abstracts, resulting in 110 records to be assessed for eligibility in the next step. Thus, in the second screening step (eligibility), for each of the 110 articles, the same inclusion criteria were applied to the entire article (i.e., a complete reading of the article). At the end of this second stage, 32 studies were selected to be included in the review. Table 1 shows the main characteristics of the 32 studies included in the scoping review, according to the variables described in Sect. "Data charting process and data items".
Regarding the types of populations (cf. PICOS criteria), 9 studies out of 32 focused on emotional eating (EE), 21 studies out of 32 focused on binge-eating disorder (BED), and 2 out of 32 focused on overeating (OE). Regarding the types of intervention/exposure (cf. PICOS criteria), namely, ER and inhibition/impulsivity, 19 studies out of 32 focused on emotion regulation (ER), 18 studies out of 32 focused on inhibition/impulsivity, and 5 out of 32 focused on both ER and inhibition/impulsivity. More than a third of the included studies (11 studies out of 32, ≈ 34%) were conducted in Germany. Moreover, more than half of the studies (17 studies out of 32, ≈ 53%) were conducted in Germany or in countries bordering Germany (i.e., France, Switzerland, Belgium and Poland).
Summary of findingsEmotional eating and emotion regulation
Studies confirm the existence of a link between ER and EE, including the fact that ER difficulties predict EE. For example, Stapleton and Whitehead [18] highlighted that “Emotion regulation difficulties was the greatest predictor of emotional eating, suggesting that individuals who have difficulty regulating their emotions are more likely to engage in emotional eating behavior”. Similarly, Crockett et al. [3] concluded that “In every model we tested, difficulties in emotion regulation predicted emotional eating”. Sultson and Akkermann [19] concluded that "Higher level of ER difficulties among obese and normal weight individuals with EE also lend further support for the assumption that emotion dysregulation might underlie EE". Kornacka et al. [20] highlighted the “[…] crucial role of ruminative thinking in the occurrence of emotional eating […]”. Regarding avoidance, Deroost and Cserjési [21] showed “[…] that people with a high degree of EM use avoidance as a primary coping strategy" and added that "avoidance coping also significantly predicted the level of EM” (EM = emotional eating).
Future studies focusing on EE and ER should separately test other specific types of emotional eating (e.g., EE in response to depression, to anxiety…). Indeed, Braden et al. [22] explained that “exploratory analyses suggest possible unique relationships between types of emotional eating and specific facets of emotion regulation”. The authors added that “[…] findings suggest that certain emotion regulation strategies may be more closely linked to various types of emotional eating”.
Emotional eating and inhibition
The studies included in this scoping review dealing with EE and inhibition/impulsivity confirmed the existence of an association between EE and some inhibition difficulties and impulsivity. For example, Wolz et al. [23] showed that “[…] emotional eating was not related to general inhibitory control deficits, but was associated with higher behavioral inhibitory control difficulties only while suppressing negative emotions. They added that “[…] the difficulty to inhibit behavioral responses while regulating negative emotions may contribute to disinhibited food intake while experiencing negative emotions”. Stapleton and Whitehead [18] revealed that emotional eating was related to high impulsivity and that impulsivity was the second greatest predictor of EE after emotion regulation difficulties. Regarding self-control, Wood et al. [24] showed “[…] an increase in activation across brain regions related to self-control and urges in response to high-calorie food associated with both emotional eating and routine restraint". Taken together, these findings confirm that emotional eaters are prone to inhibition impairments. Moreover, Wolz et al. [23] suggest that deficits in inhibition only appear when participants are regulating their emotions, highlighting an interesting link between ER and inhibition in EE.
BED and emotion regulation
Concerning BED and emotion regulation, most of the studies confirm the ER difficulties in BED. Leehr et al. [25] showed that individuals with BED have lower ER capacities. Limited access to ER strategies is also one of the ER difficulties met in BED [26, 27], as well as nonacceptance of emotional responses [27] and lack of emotional clarity [26, 27].
BED and inhibition
Overall, studies focusing on BED indicated a deficit in inhibition and increased impulsivity. Leehr et al. [25] concluded that “Overall, results support the assumption of inhibitory control deficiencies in BED on a behavioral level”. Grant and Chamberlain [28] underlined that “Binge-eating disorder was associated with impaired response inhibition and executive planning”. Schag et al. [29] said that “[…] BED represents a neurobehavioural phenotype of obesity that is characterized by increased impulsivity”, and Leehr et al. [30] showed that “the BED + sample showed higher trait and behavioural impulsivity”. Moreover, according to Aloi et al. [31], “[…] impaired self-monitoring metacognition and difficulties in impulse control are the central nodes in the psychopathological network of BED […]”.
Overeating and emotion regulation
One of the objectives of this scoping review was to clarify the ill-defined concept of overeating. In the eating disorders literature, overeating sometimes refers to a symptom of an eating disorder or as an eating behavior or is sometimes used as a synonym for emotional eating or binge eating.
Unfortunately, only two of the studies included in this scoping review focused on overeating [32, 33], so we could not address this specific question. Nevertheless, similar to EE and BED, those studies highlighted the links between overeating and emotion regulation.
Positive emotions and emotional eating
We questioned the possibility of positive emotions causing emotional eating episodes associated with emotion regulation and/or inhibition difficulties (in the same way as negative emotions). Based on the studies included in our review, opinions differ regarding this point. Indeed, while an article highlights that “[…] positive EE was associated with elevated levels of ER difficulties, suggesting that overeating in response to positive emotions might also include some features of emotion dysregulation” [19], another article concludes, on the contrary, that “[…] eating in response to positive emotions was not significantly related to poorer psychological well-being, greater eating disorder symptoms, or emotion dysregulation” [22]. Since there is yet no consensus on the subject, further research on emotional eating needs to be conducted to separately test and dissociate positive and negative emotions.
Positive emotions and BED
We wondered about positive emotions as a possible cause of emotional eating episodes associated with emotion regulation and/or inhibition difficulties. We checked whether the BED studies included in this scoping review addressed the question of positive emotions/affect/mood. Loeber et al. [34] showed that “[…] restrained eating and mood are factors that moderate response inhibition to food-associated stimuli in obese patients with BED” and that “[…] apart from negative mood, positive mood might as well be a trigger for loss of control over eating behaviour”.
Finally, it is worth mentioning that one study showed that negative and positive mood levels are different during binge days, with an increasing negative mood and a decreasing positive mood at the first binge-eating episode (see Munsch et al. [35]).
Emotional eating and weight profiles
Studies included in this scoping review tended to show that the relationships between EE and emotion dysregulation (and anxiety, depression, and rumination) might be different according to the weight profile (i.e., normal weight, overweight, and with moderate or severe obesity) (see, for example, Willem et al. [36] or Kornacka et al. [20]). Willem et al. [36] highlighted that “emotion dysregulation, anxiety and depression have different impacts on emotional eating (EE) depending on obesity severity", while Kornacka et al. [20] underlined that “the role of emotional eating in the link between rumination and uncontrolled eating is different in overweight vs. healthy individuals”.
Emotional eating, BED and rumination
According to three of the studies included in this scoping review, rumination, a maladaptive emotion regulation strategy, is encountered in both EE and BED. Indeed, in EE, Kornacka et al. [20] highlight that rumination is a predictor of EE (“[…] the results of the two studies confirm the crucial role of ruminative thinking in the occurrence of emotional eating […]”. Similarly, people with BED are more inclined than healthy people to use rumination as a negative emotion regulation strategy [27]. Wang et al. [37] also highlighted that “[…] rumination is an important cognitive process associated with severity of eating-disorder psychopathology”.
The idea of a possible continuum
We hypothesized that there would be a continuum between EE (nonpathological eating behavior) and BED (pathological eating behavior). Three studies focusing on BED mentioned this idea of a continuum in the severity of eating disorders. Leehr et al. [25] stated that “From a clinical perspective eating behavior of the three groups can be seen on a continuum from normal eating behavior, to overeating, to binge eating”. Mobbs et al. [38] highlighted that “[…] these cognitive deficits are more severe in obese patients with binge eating disorder, which indicates that there is a continuum of increasing inhibition and cognitive problems with increasingly disordered eating”. Moreover, Svaldi et al. [39] underlined that “[…] the magnitude of the inhibitory deficit was found to be related to the reported severity of eating pathology”, which is compatible with the idea of a continuum.
However, none of the reviewed studies directly compared EE to BED regarding ER or inhibition performances, neither in a longitudinal nor cross-sectional design. Thus, a gap can clearly be identified in this specific field since there is a complete lack of experimental data about an increased severity in ER and inhibition deficit between EE and BED.

Comments (0)