
Remember me
Anti-fat bias and weight stigma are terms used interchangeably to refer to the social devaluation of individuals perceived to have excess bodyweight; they are pervasive and detrimental to the mental and physical health and wellbeing of their targets [44]. Negative effects include elevated rates of mood and anxiety disorders, inflammation, metabolic dysregulation, and an increased risk of death [19, 30, 41, 44]. Furthermore, a growing body of evidence suggests that experiencing weight stigma may actually lead to weight gain via activation of stress response systems (e.g., cortisol release), which signal to the body to store fat as protection against perceived threat [43]. Despite these harmful consequences, anti-fat bias and discrimination remain not only socially acceptable, but legally permissible and, in many cases, central to medical care practices. Given its omnipresence, it is critical to identify the primary factors underlying the development and perpetuation of anti-fat bias as a first step to eradicating it.
Anti-fat bias and beliefs about the selfThere is strong consensus among researchers that anti-fat attitudes directed toward the self are a consequence of internalizing the pervasive societal devaluing of the identities of individuals with stigmatized bodies [28, 34, 35]. This internalized weight bias and resulting self-stigma pose a substantial risk to the physical and mental health of the individual, as they have been shown to predict disordered eating and psychological distress [3, 16]. In addition to the elevated risks to the individual’s health and wellbeing, recent models of anti-fat bias have suggested that negative evaluations of others with excess bodyfat may originate from the same beliefs underlying negative evaluations of one’s own bodyfat (i.e., weight self-stigma or self-directed anti-fat bias; [8, 10, 12]). This duality, of internalized pressure to conform to a rigid standard and simultaneous judgment of those who do not, has been shown to exist in children as young as 8 and persist throughout adulthood, regardless of bodyweight [4, 37]. Himmelstein and Tomiyama [21] provide empirical support for this relationship, demonstrating that self-directed anti-fat biases influence individuals’ endorsements of negative attitudes and stereotypes directed toward others with excess bodyfat. Associations between anti-fat attitudes directed toward the self and others have been supported in multiple recent studies, though such studies are limited by cross-sectional designs [2, 29, 32]. Gender has also been shown to play a significant role in anti-fat bias, such that the relationship between self- and other-directed anti-fat attitudes is stronger among women than men [14, 25].
Anti-fat bias and implicit attitudesAnti-fat attitudes likely also stem from internalized implicit negative beliefs about bodyfat in general, encoded independently of assignment to the self or others. These implicit negative beliefs are associated with and may underlie explicit demonstrations of anti-fat bias directed towards others and the self. Research on the association between implicit versus explicit evaluative processes comes from a rich and complex theoretical tradition, but generally posits that implicit attitudes develop via cognitive processes that are distinct from the development of explicit attitudes [45].
Although research examining how implicit anti-fat attitudes relate to behavior has thus yielded mixed results, elevated implicit bias has been observed among individuals with low or no endorsement of explicit anti-fat bias on self-report measures [6, 36, 45]. This is consistent with the literature on bias in other domains (e.g., race, sexual orientation) and is believed to reflect persistent, internalized negative beliefs despite an awareness that overtly expressing negative attitudes toward members of marginalized groups is socially unacceptable. However, in contrast to implicit racial and sexuality biases, which have steadily declined since 2007, implicit anti-fat biases have remained static [7]. It is therefore critical to investigate the cognitive pathways underlying distinctly persistent implicit anti-fat attitudes to identify effective strategies to resolve them.
Associative-propositional evaluation modelGawronski and Bodenhausen’s [17] Associative-Propositional Evaluation (APE) Model may provide a useful framework for conceptualizing the complexities in the origins, relationships between, and perpetuation of self- and other-directed implicit and explicit anti-fat bias. The APE Model proposes two distinct, but co-occurring, internal mechanisms by which stimuli are evaluated according to pre-existing beliefs. The two processes, associative and propositional, functionally align with the development of implicit and explicit biases, respectively. The APE model distinguishes these two processes by the presence of a truth evaluation. More specifically, associative processes, which are posited to facilitate the development of implicit attitudes, are activated quickly, upon internalized beliefs which are not evaluated for truth or validity. By contrast, propositional processes, which are theorized to facilitate the formation of explicit attitudes, require the evaluation of the truth or validity of the belief upon which an attitude is based.
The APE model provides a particularly useful framework for conceptualizing the mechanisms underlying inconsistencies observed in explicit and implicit biases. For instance, an individual who holds an internalized belief that excess bodyweight is the direct result of laziness may react to someone they perceive as having overweight in the kickboxing class they attend several times per week with an automatic, negative associative evaluation. This evaluation is activated automatically as a result of consistent exposure to pairings of overweight with such negative qualities as laziness, thus it is not evaluated for truth or validity.
In contrast to the associative process, the propositional process is more controlled and used to develop explicit evaluations. Through this process, an individual is forced to develop and articulate an explicit evaluation of an individual with excess bodyfat. The individual is forced to reconcile their automatic negative response resulting from internalized beliefs with contradictory observations of their classmate working hard and succeeding in the high-intensity exercise sessions. Knowledge of the marginalization of people categorized as having overweight and the belief that it is wrong to discriminate against members of marginalized groups may further convince the individual to develop less negative explicit attitudes toward people perceived as having overweight and obesity. Given the validity evaluation, and subsequent rejection, of the initial core belief, it is also possible that the individual’s implicit anti-fat attitudes may shift to align with their explicit attitudes.
Dissonance and reconciling conflict between automatic and propositional evaluationsFestinger’s [15] theory of cognitive dissonance is primarily based on the tendency for individuals to experience discomfort when their automatic evaluations of a given stimulus are inconsistent with their propositional evaluations based on relevant information or their personal values. Festinger suggested that individuals will modify the flawed beliefs underlying their automatic evaluation to be consistent with their propositional evaluation in an effort to resolve this discomfort. This principle has been incorporated into interventions in several domains by strategically prompting individuals to generate and rationalize cognitions that directly oppose an undesirable attitude or behavior.
Although this approach has not yet been applied to reduce self- and other-directed anti-fat bias in tandem, prior research suggests that it may be effective for targeting attitudes and motivation around these biases [1, 5, 9, 26, 38, 39]. Therapeutic applications of cognitive dissonance principles have predominantly been studied for reducing self-directed anti-fat bias and related constructs (e.g., fear of fat), which, according to a recent meta-analysis, have the most empirical support for preventing eating disorders compared with other interventional approaches [38]. Among the most effective dissonance-based interventions for reducing self-directed anti-fat bias is the Body Project, which aims to induce dissonance surrounding the marketing of diet culture, idealized thinness, and other internalized beliefs and cognitions that precede disordered eating behavior using a series of structured meetings held in a group therapy setting [1, 38]. While the results of prior studies suggest that cognitive dissonance-based therapies may hold tremendous potential for reducing explicit self-directed anti-fat bias and preventing eating disorders, their effect on anti-fat biases directed toward others has been less extensively studied.
Although the use of cognitive dissonance principles to reduce anti-fat attitudes directed toward others is a relatively newer application, emerging evidence suggests that it could be a promising interventional approach [11, 23, 27]. In an initial test of this approach, participants randomized to a dissonance-inducing condition showed a significantly greater reduction in explicit anti-fat attitudes, compared with a control group [9]. Despite providing evidence which favors cognitive dissonance interventions for reducing explicit anti-fat bias, the aforementioned studies did not measure implicit bias. In a similar study examining the effects of a cognitive dissonance intervention vs. a no dissonance control condition on explicit and implicit anti-fat attitudes, researchers observed that the dissonance group reported a reduction in explicit anti-fat attitudes following treatment, but no significant effect was observed for implicit anti-fat attitudes [5].
It is important to note that, in each of the studies described above, the cognitive dissonance intervention for reducing other-directed anti-fat bias was not comparable to that of the Body Project or other interventions more closely modeled after Festinger’s principles. More specifically, Festinger emphasized the importance of an individual generating their own cognitions that are incongruent with existing beliefs in order to properly induce cognitive dissonance [15]. Many of the dissonance-based interventions designed to reduce self-directed anti-fat biases, including the Body Project, incorporate this principle by facilitating discussions in which participants are prompted with questions that are strategically designed to induce dissonance by eliciting logical responses that are incongruent with existing beliefs [40]. For instance, in one Body Project exercise, participants are instructed to write a letter to a younger girl who is struggling with her body image by explaining the costs associated with pursuing the idealized thin body. In another, participants must confront the irrational expected benefits (e.g., “I’ll be happy all the time if I’m thin” and “Everyone will like me”) they associate with reaching their idealized bodyweight.
In contrast to the dissonance-based interventions aimed to reduce self-directed anti-fat bias, many of the existing dissonance-based interventions for other-directed anti-fat bias reduction do not prompt participants to generate their own dissonant cognitions. Rather, dissonance is imposed upon participants via mild researcher deception. Aside from Meaney and Rieger [27], which included an additional reflective writing task, in which participants were instructed to react to the results they had just received regarding their values and attitudes, participants are not prompted to generate their own cognitions. This context is critical for interpreting the results of previous studies, as they may be more reflective of demand characteristics after being informed that their responses indicated unusually high levels of anti-fat bias than any actual changes in participant’s attitudes. The inclusion of implicit bias measures can be useful for making the distinction between demand and genuine attitudinal change.
The present studyThe aims of the present research study are two-fold: to first develop an understanding of the cognitive pathways, and relevant associations, underlying the relationship between self- and other-directed anti-fat bias, and test the effects of cognitive dissonance interventions specifically targeting anti-fat bias in each domain. The relationship between self- and other-directed anti-fat bias will be explored through the lens of the associative-propositional evaluation (APE) model framework [17], which is also used to inform predictions regarding the intervention effects. Following baseline assessment of implicit and explicit attitudes about bodyweight of the self and others, participants were randomly assigned to complete a brief, online intervention aimed to induce cognitive dissonance surrounding anti-fat bias directed toward the self, cognitive dissonance surrounding anti-fat bias directed toward others, or a bias-consistent control condition where they were simply asked to confirm their existing biases.
The overarching expectation is that effects of the cognitive dissonance interventions specific to either domain (self- or other-directed anti-fat bias) will effect change to both explicit and implicit attitudes via shared evaluative pathways. A fundamental component of the APE model suggests that an existing cognitive association between two stimuli presented simultaneously will be reinforced. In this case, because participants are expected to have pre-existing, internalized associations between excess bodyfat and negative outcomes (e.g., discrimination), any information they encounter that presents individuals with excess bodyfat being treated poorly is expected to reinforce their existing beliefs. Thus, regardless of the condition-specific intervention tasks, pre-existing implicit associations between excess bodyfat and adverse experiences are expected to be strengthened among participants who read descriptions of discriminatory anti-fat policies (i.e., cognitive dissonance for other-directed anti-fat bias and control conditions). Among participants randomized to the cognitive dissonance for other-directed anti-fat bias condition, the effect of this stronger, negative association may be offset by the nature of their intervention task. Because they will be instructed to generate logical arguments that oppose discriminatory anti-fat policies, participants randomized to this condition were expected to report significant decreases in explicit anti-fat bias. Although either cognitive dissonance intervention could theoretically reduce bias directed towards the self and others, the APE model predicts the cognitive dissonance intervention targeting self-directed anti-fat bias should confer the greatest reduction in bias across both domains. This prediction was based on the fundamental conceptualization of self- and other-directed anti-fat biases as stemming from a common set of encoded negative associations with bodyweight. Given that the bodyweight which individuals are most frequently exposed to is likely their own, it would be expected for self-directed negative associations with bodyfat to be more frequently reinforced, and thus more strongly conditioned, than the negative associations formed in relation to the bodyfat of others. Given that strengthening these negative associations in either domain is expected to increase bias against bodyfat of both the self and others, the cognitive dissonance intervention aimed to reduce the more strongly encoded beliefs (i.e., self-directed anti-fat bias), was expected to have the most profound effect on expressed bias overall. While participants randomized to the control condition may report post-intervention decreases in explicit anti-fat attitudes, they will likely be driven exclusively by social desirability bias, and thus are expected to be weaker than in the other conditions.
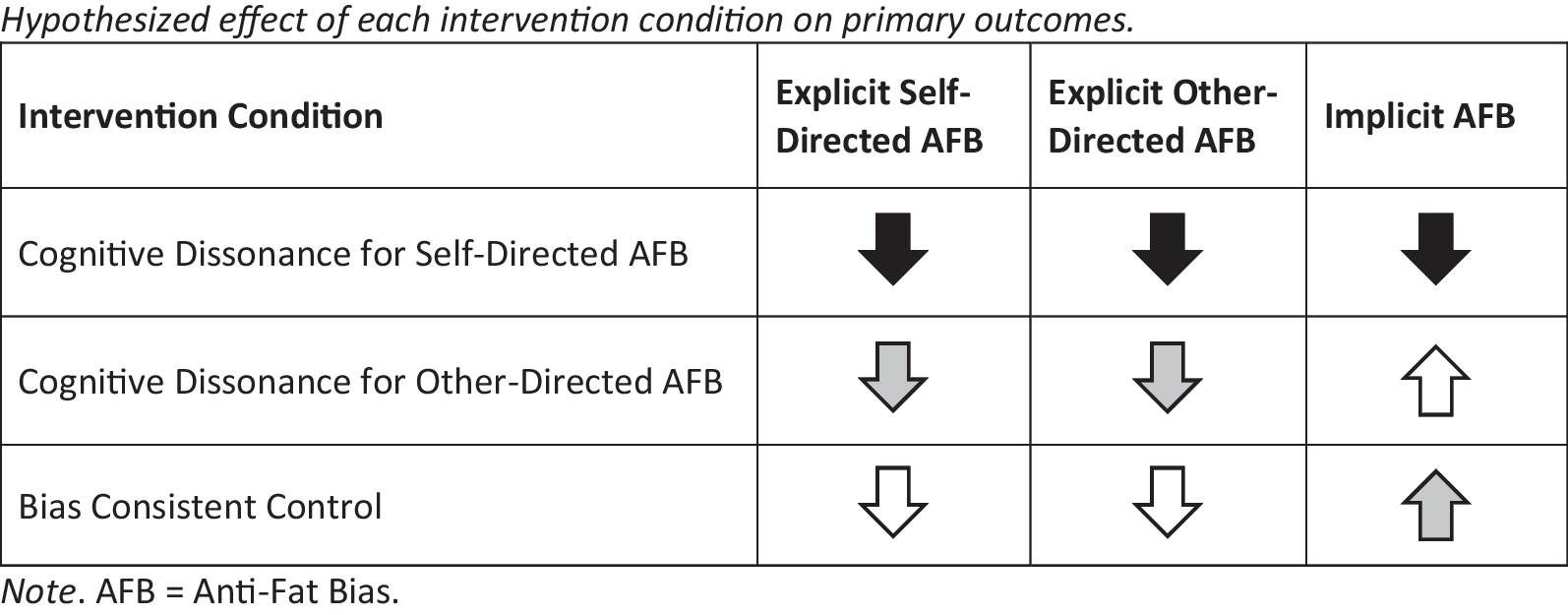
To summarize (see Fig. 1), it is expected that participants randomized to the cognitive dissonance for self-directed anti-fat bias condition will show the greatest reduction in explicit self-directed anti-fat bias from baseline to post-intervention, followed by participants in the other-directed anti-fat bias cognitive dissonance condition, with the smallest effect observed among participants in the control condition. Participants in all three conditions will report reductions in explicit other-directed anti-fat bias from baseline to post-intervention, however, this effect will be strongest among those in the self-directed anti-fat bias condition. Implicit anti-fat bias is expected to decrease only among participants randomized to the cognitive dissonance for self-directed anti-fat bias condition.
Fig. 1
Hypothesized effect of each intervention condition on primary outcomes. Note. AFB = Anti-Fat Bias. Arrows reflect predicted directed of effect. Shading reflects strength of predicted effect (i.e., black = strongest effect, grey = moderate effect, white = small to nonsignificant effect)
Comments (0)