Subject selection
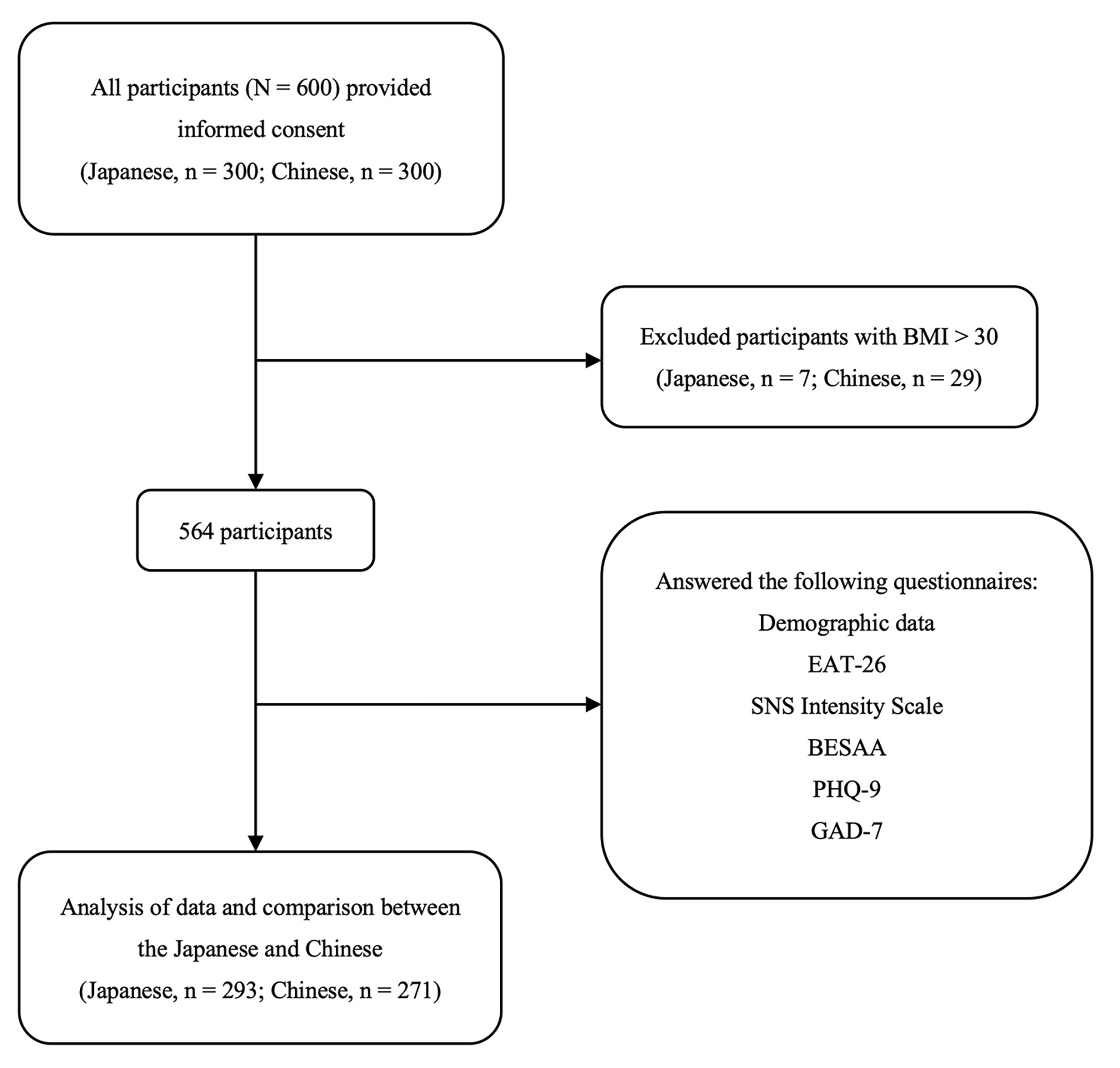
This retrospective chart audit examined the case notes of all patients below the age of 18, who presented for evaluation for an eating disorder in both the inpatient or outpatient settings at KK Women’s and Children’s Hospital between January 2010 and October 2020. Patients with Bulimia Nervosa, Avoidant/Restrictive Food Intake Disorder and other unspecified conditions were excluded from the review. Data for this study was used in accordance with guidelines from SingHealth Institutional Review Board.
Eating disorder diagnoses
At the time of presentation, all patients participated in a multidisciplinary intake evaluation led by an adolescent medicine physician with eating disorder expertise. Prior to 2014, DSM IV criteria were used at the time of assessment to assign eating disorder diagnoses [22]. From 2014 onwards, DSM-5 criteria were used to assign eating disorder diagnoses.
At the time of the case audit, case notes and diagnoses were reviewed by an adolescent medicine physician and a psychologist with expertise in EDs to retrospectively assign a diagnosis using DSM-5 criteria for patients who were initially assessed using DSM-IV criteria [4] and to ensure the application of consistent BMI and weight loss criteria across all cases.
Low weight for AN was defined as a percent median Body Mass Index (mBMI%) of less than 87%. The preceding criterion has been applied in other studies on adolescent ED [23,24,25]. Patients who met all criteria for AN, but who had normal or above-normal BMI at presentation (defined as %mBMI of greater than 87%) despite significant weight loss were classified as AAN. Published criteria for severe malnutrition were used to establish the definition of significant weight loss [26].
Patient variables at presentation
Ethnicity (Chinese, Malay, Indian, and Others including Caucasian and Filipino), highest historical weight and corresponding height, menstrual status, duration of weight loss, presence of purging, and use of weight loss medications were self-reported by patients and parents at first presentation. Measurements for height, weight, and an orthostatic measurement of heart rate and blood pressure (lying and standing) were abstracted from the clinical record. Duration of admission and reasons for it were recorded.
Weight variables and menstrual history
Percent median BMI (%mBMI) was calculated using the BMI of the patient divided by the 50th percentile BMI corrected for age and gender, and multiplied by 100. Fiftieth percentile BMI (%mBMI) for exact age was determined using the BMI-for-age growth charts for Singaporean children and adolescents aged 4 to 18 years [27]. Weight loss was defined as the change in %mBMI from highest %mBMI to the %mBMI at presentation. Duration of weight loss (months) was defined as the time interval between the date of highest weight and the presentation date. Rate of weight loss was the change in %mBMI divided by the duration of weight loss [14]. Secondary amenorrhea was defined as the disruption of previously regular menstruation cycles for 3 months or more [28].
Admission criteria
Criteria for admission included physiologic instability such as bradycardia and hypotension as well as acute medical complications of malnutrition including syncope as per published international guidelines [29]. Syncope is defined by transient loss of consciousness and postural tone with spontaneous recovery [30]. Admission criteria also included the presence of significant safety concerns such as attempted self-harm or suicide requiring medical or safety monitoring. Patients admitted for medical instability were placed on ED care protocols for medical stabilization [24].
Psychological measures
The Eating Disorder Examination Questionnaire (EDE-Q) [31] is a self-administered questionnaire with scores ranging from 1 to 9. Higher scores indicate greater severity of ED psychopathology. In our service, routine administration of the EDE-Q started in 2016 as part of the multidisciplinary assessment.. Psychologists or psychiatrists from the ED team evaluated for psychiatric comorbidities including symptoms of anxiety and depression, suicidal ideation, and self-harm. Only diagnoses assigned by the treating psychologist or psychiatrist were abstracted from the case notes.
Statistical analysis
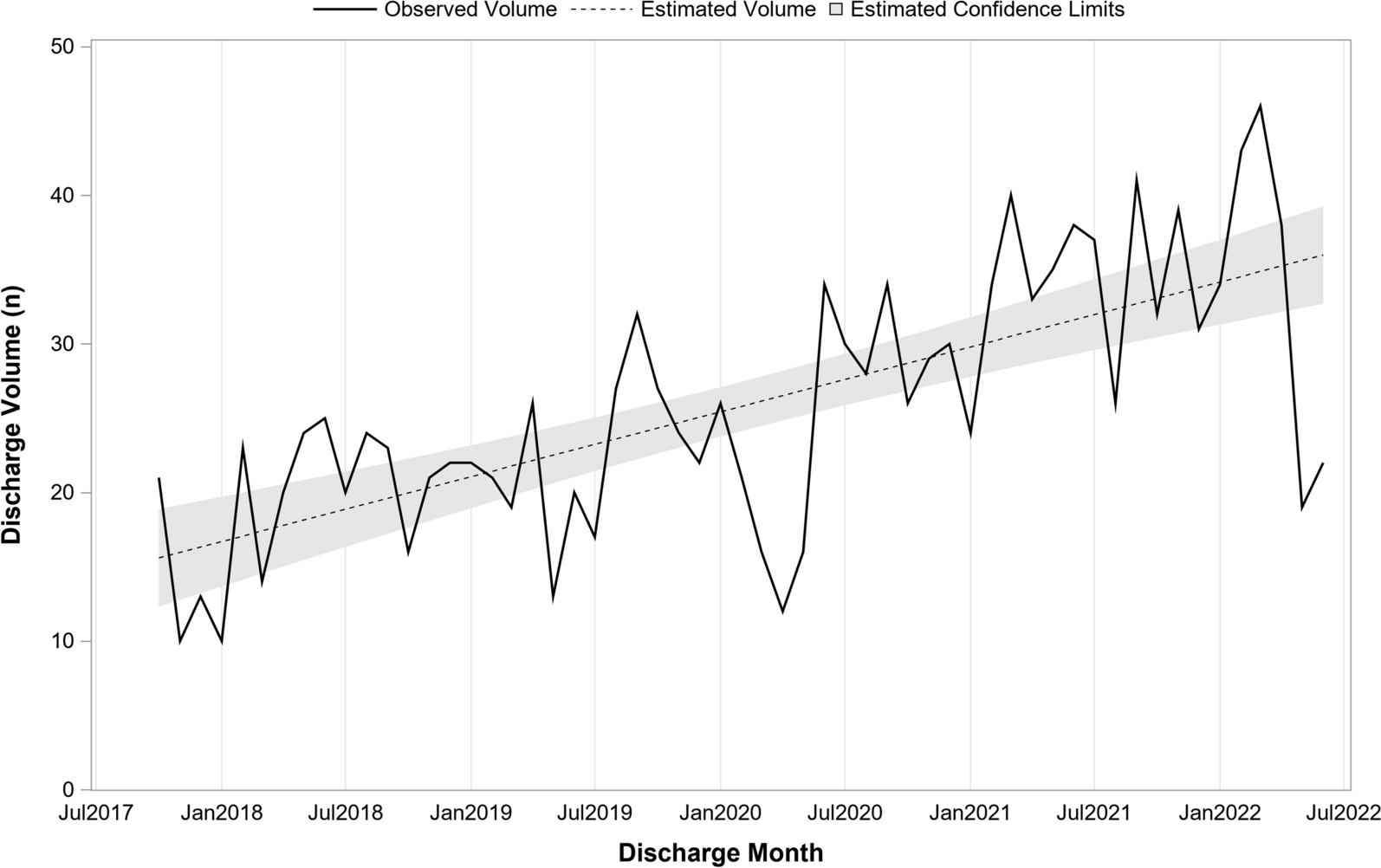
Data was analysed using SPSS software version 19 for Windows (SPSS Inc., Chicago, IL). Baseline demographic and anthropometric measurements of study participants were compared between patients with AN and AAN using two independent samples t tests (or Wilcoxon rank sum, depending on normality) and chi-square tests (or Fisher exact test, where appropriate) for continuous and categorical variables respectively. Data were presented as mean ± standard deviation for continuous variables, and frequencies and percentages for categorical variables. The number of adolescents with AAN was presented as a proportion of the total AN and AAN cases along with a line of best fit. Associations between four weight history variables (independent variables) and markers of illness severity were examined with multiple regression models. The four independent weight variables were: (1) %mBMI (2) Change in %mBMI (3) Rate of weight loss (4) Duration of weight loss. Models were adjusted for gender, age and race. Multivariable linear regression, followed by stepwise backward selection, was used to examine the contribution of the weight variables on illness severity outcomes measures. Measures of illness severity were vital signs at presentation (heart rate and systolic blood pressure), duration of admission, and ED psychopathology (global EDE-Q scores).

Comments (0)