To our knowledge, our study was the first to explore the perceived causes of EDs via large-scale social media data from Chinese social media users with self-reported EDs. In our study, data from Zhihu were analyzed to understand self-perceived causes of EDs among users. Based on Blodgett Salafia and colleagues [28], we manually coded 2079 posts, out of an initial 5199 posts, for specific causes for subsequent statistical analysis. Results showed that “psychological and emotional problems” and “body image and eating” were the two most commonly self-perceived causes. Chi-square independence tests revealed that individuals with self-reported AN reported more causes of “social and cultural factors” than those with self-reported BN and self-reported BED. Additionally, individuals with self-reported BN were more likely to claim causes of “media and cultural ideals” and “body image and eating” than those with self-reported AN and self-reported BED. The study highlighted the importance of investigating the self-perceived etiology of different EDs and demonstrated the value of social media data in identifying perceived risk factors among Chinese users with self-reported EDs.
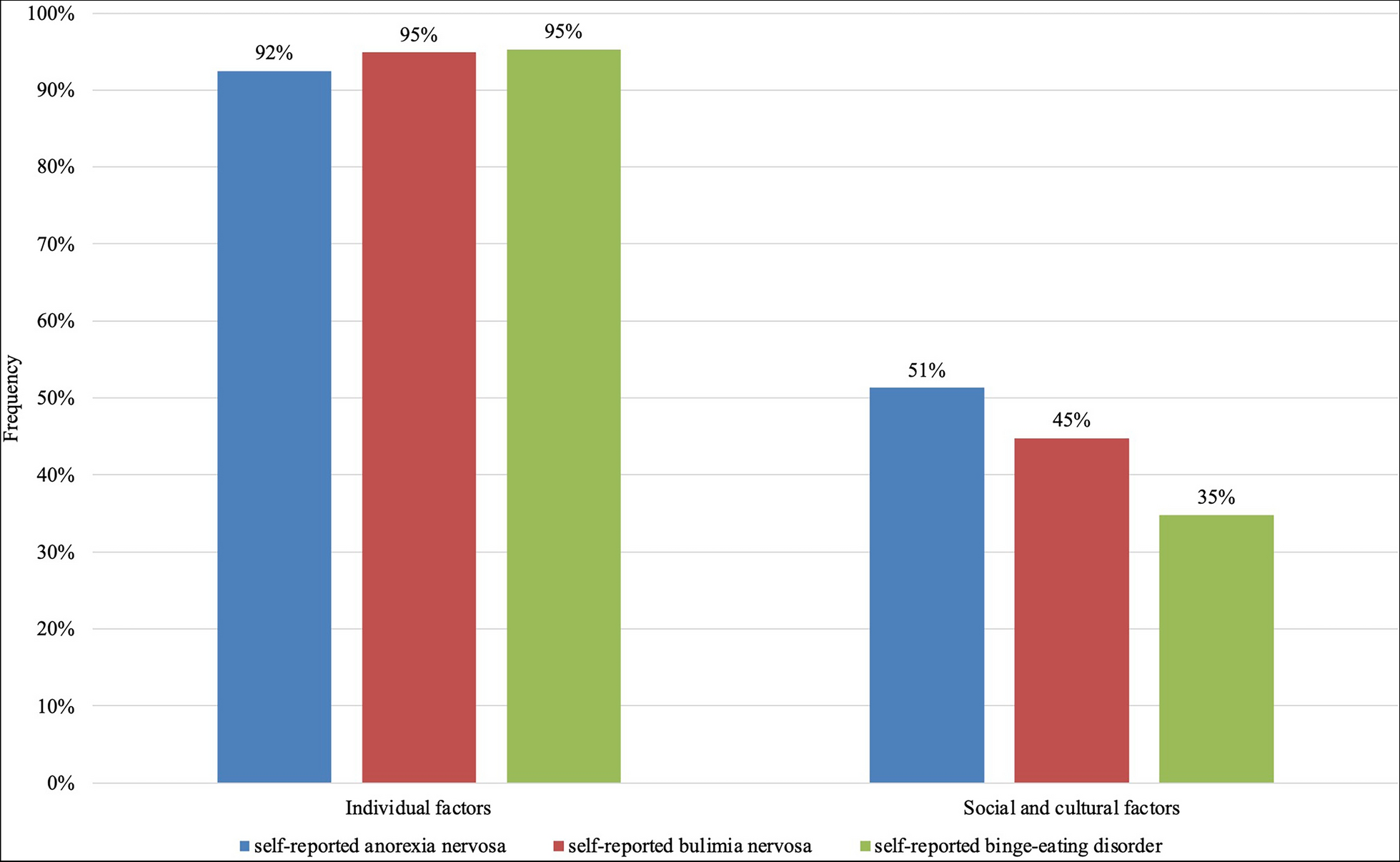
Frequencies of self-perceived causes of eating disorders
In the current study, individual factors (e.g., “psychological and emotional problems” and “body image and eating”) were more likely to be identified as perceived causes than social and cultural factors (e.g., “social problems” and “media and cultural ideals”) across all self-reported EDs. This pattern aligns with the findings of research conducted by Blodgett Salafia and colleagues [28]. The sociocultural theories of body image and disordered eating (e.g., the tripartite influence model [30]) might shed light on potential explanations. Specifically, as proposed by the tripartite influence model [30], both social and cultural factors and individual factors serve as mechanisms of disordered eating. However, these two kinds of factors differ in order, with sociocultural factors (e.g., appearance pressures from peers, family, and media) being more distal than proximal individual factors (e.g., internalizing societal appearance standards, engaging in appearance comparison, and being dissatisfied with one’s own body). Similar findings have been reported in research on the attribution of obesity [31], with individual factors (e.g., less physical activity, over-eating, and comfort eating) being perceived as proximal causes of obesity and family problems being perceived as distal causes. Thus, users may be more likely to claim “closely” related, proximal causes to their EDs. Also, based on Weiner’s attribution theory [32], when individuals attempt to identify the causes behind their behaviors, they tend to consider the controllability of the behaviors (i.e., the extent to which the individual can influence them). Considering disordered eating behaviors are performed by individuals themselves, they may tend to perceive the behaviors as controllable, which may lead them to be more likely to attribute their EDs to internal factors (i.e., individual factors). Thus, our findings may disproportionately reflect individuals’ attribution bias, and it does not mean social and cultural factors are not as important as individual factors, especially considering that recent studies showed that social and cultural factors (e.g., appearance pressures from family, peers, significant others, and media) had strong and consistent direct links with eating disorder symptomatology in both Chinese men and women [33, 34].
Our study also lends evidence to the connections between both individual and social/cultural factors and self-reported ED types. Particularly, our results showed that users with self-reported BED were more likely to report individual factors; in contrast, users with self-reported AN or self-reported BN were more likely to report social and cultural factors. Unlike self-reported AN and BN, individuals with self-reported BED typically do not engage in compensatory behaviors (e.g., dieting, purging) but instead may use binge eating as a coping mechanism for stress and emotional distress related to body image pressures. Striegel-Moore and Bulik [35] claimed that individuals with AN and BN were vulnerable to environmental factors (i.e., sociocultural pressures to attain thin ideals). Indeed, a study involving Croatian high school girls supported that those with higher body mass index (BMI) who embraced social standards of thinness were more likely to perceive social pressures to be thin, often manifested through direct and persuasive comments emphasizing the importance of dieting, which might contribute to the development of AN or BN [36]. These findings speak to the complex interplay of individual and societal factors in the development of EDs and underscore the importance of addressing both in treatment and prevention strategies.
Notably, our findings regarding the most frequently self-perceived causes (e.g., “psychological and emotional problems,” “body image and eating,” and “media and cultural ideals”) of EDs align with those reported by empirical studies of patients with EDs in China, in which psychological distress, body image disturbances, and sociocultural changes were identified as key risk factors of EDs (e.g., [37,38,39]). However, although these empirical studies are valuable, the factors investigated in prior studies using clinical samples might not be comprehensive, and the generalizability of related findings might be questionable due to the small sample sizes (e.g., a few cases with EDs [39]). Thus, our study expands on prior literature in China by comprehensively investigating the self-perceived causes from a much larger and more diverse sample, findings that contribute to our understanding of the etiology of EDs and related health literacy of individuals with self-reported EDs in the Chinese context.
Frequency differences of self-perceived causes for all types of eating disorders
In our study, the causes of “psychological and emotional problems” and “body image and eating” were the two most frequently perceived causes. These findings were consistent with the well-documented literature that psychological and emotional problems (e.g., difficulties in emotion regulation and psychological distress) are core, transdiagnostic risk factors of EDs [28, 40,41,42,43]. Also, body image concerns (e.g., weight/shape dissatisfaction) and eating concerns (e.g., restrictive eating) are core risk factors and/or major manifestations of EDs [42, 44], including in Chinese adults [45]. Following the two most perceived causes are “social problems,” “family problems,” and “media and cultural ideals.” Based on the tripartite influence model [30], sociocultural factors are important sources contributing to the development of EDs. Indeed, empirical research conducted in China consistently suggests that socially promoted body ideals (e.g., thin ideal [46]) and related pressures are important risk factors of EDs [33, 34, 47].
Relationships between self-perceived causes and types of eating disorders
In our present study, interestingly, we found a statistically significant relationship between self-reported ED types and the preference for anonymity, especially users with BN being more likely to opt for anonymity compared to those with self-reported AN and self-reported BED. One potential explanation is that, unlike individuals with AN and BED who may show significant signs of appearance changes (e.g., becoming underweight or overweight) to be observed by others, individuals with BN often have less significant appearance changes (e.g., maintaining a relatively normal weight), which makes their symptoms less likely to be detected by others [48]. Also, individuals with BN might feel ashamed of their binge eating and compensatory behaviors, especially purging or self-induced vomitting, and do these secretly [49]. Thus, it might be preferred by individuals with BN to choose anonymity as compared to those with AN and BED.
Additionally, our study found that users with self-reported BN were more likely to claim “body image and eating” causes compared to those with self-reported AN or self-reported BED. Indeed, abundant research has uncovered differences in eating and body image disturbance among AN, BN, and BED (e.g., [50, 51]). For example, Lydecker and colleagues [50] reported that patients with AN and BN exhibited higher levels of preoccupation with both shape/weight and food/eating than those with BED. Therefore, it is crucial to refine and differentiate the specific eating and body image disturbances across various EDs in the future to enhance the diagnosis of different ED types and tailor case conceptualization and treatment planning more effectively.
In addition to “body image and eating,” the frequencies of “media and cultural ideals” were also significantly different across self-reported ED types, with self-reported BN being the highest. The empirical literature has demonstrated that media use (e.g., social media use), as well as body ideals (e.g., thin ideals), are associated with body image concerns and eating disturbance among Chinese samples (e.g., [52,53,54]). However, to our knowledge, limited research evidence is available on how media and cultural ideals may contribute differently to developing various types of EDs. Thus, our finding of individuals with self-reported BN endorsing more perceived influence from media and cultural ideals may suggest a stronger connection between media and cultural ideals and BN compared to that between media/cultural ideals and AN/BED. Thus, media-based interventions for EDs might be more effective for Chinese individuals with BN. However, this postulation should be examined in future studies with validated samples of EDs.
Notably, the rates of self-perceived “genetics and biology” causes varied significantly across different self-reported ED types as well, with self-reported AN having a lower rate compared to self-reported BN and self-reported BED. Studies involving twins and families have provided compelling evidence regarding the heritability of various ED types and have linked specific genes and their variants to these EDs (e.g., [55,56,57]). For instance, genetic factors are responsible for approximately 33–84% of AN cases, 28–83% of BN cases, and 41–57% of BED cases [57]. Thus, one plausible explanation is that different from BN and BED, AN does not involve binge eating or loss of control eating, which are closely related to obesity [58]. Given that Chinese media frequently identifies genes as a risk factor for obesity [59], individuals exposed to Chinese media may be more likely to perceive BN and BED, as opposed to AN, as more influenced by genes and one's biological profile.
Clinical implications
The findings of the present study have clinical implications. First, the perceived differences in causes across different self-reported EDs shed light on ED intervention and treatment in the Chinese context. Specifically, findings from the present study may be relevant to the early stages of clinical intervention of EDs in which patients and providers discuss, through psychoeducation, the reasons/causes of EDs. Some patients may arrive in the clinic with ideas of what causes their EDs (e.g., individual factors), as identified by this study, and others may underestimate other relevant factors (e.g., biological/genetic factors). Providers may target such gaps to enrich patients’ understanding of their EDs and support the development of a comprehensive treatment plan. Recognizing these differences may allow for more effective and personalized strategies in the treatment and prevention of different EDs.
Furthermore, given China’s large population base, this study underscored the importance of prioritizing initial screening, detection, and prediction of EDs for further prevention and intervention. The findings draw attention to developing more effective approaches to address the rising concerns of EDs in the general population and could help inform public health strategies and healthcare policies. Indeed, findings from this study also have implications for educating lay people in China, including caregivers, about EDs to increase their literacy of the numerous and complex etiological factors of EDs. This is important considering that many Chinese people suffering from EDs and their caregivers may have low literacy of EDs, including etiological factors [9].
Limitations and future research directions
This study has limitations that should be acknowledged. First, our sample was a relatively homogeneous group in terms of sex, which may impact the generalizability of our findings. Our study did not find a statistically significant relationship between sex and self-reported ED types; the lack of significance in sex differences might be attributed to missing sex information during data wrangling, which resulted in a relatively small sample size of males. However, ample research evidence has suggested that sex differences were observed in the prevalence of ED symptoms (e.g., [60, 61]). Therefore, future research should consider the sex-balanced sampling of participants, as well as additional social identities (i.e., gender identity, ethnicity, socioeconomic status, and sexual orientation [62, 63]). This expansion would enable a better understanding of the impact of sex and other demographic factors on self-perceived ED etiology, enhancing the generalizability of the results.
Second, the representativeness of our results might be restricted, as Zhihu, despite its large user base in China, may not fully represent all Chinese social media users. Moreover, due to the nature of Zhihu’s user base, we recognize that it may not represent the more interactive and emotion-driven discussions found on other platforms, such as Xiaohongshu (Little Red Book), a Chinese equivalent of Instagram. Therefore, future research could broaden the scope to include other platforms, collecting comparable data from social media sites such as Xiaohongshu to validate and expand on our findings.
Finally, these data regarding perceived causes of EDs were collected indirectly from social media users who self-reported EDs by using content analysis of their social media posts. The perceived causes in the present study may be different from the perceived causes that are directly collected from patients with EDs via clinical interviews. Thus, future research should consider gathering data from social media and direct interviews with patients with EDs to examine whether and to what extent the perceived causes may differ.

Comments (0)