
記住我






A community-based cross-sectional study was conducted in Mettu town, Ilubabour, southwest Ethiopia. It is located 600 km away from Addis Ababa, the capital city of Ethiopia. The town has been divided into six administrative kebeles with an estimated total population of 49,538 and 10,321 households. The estimated number of women in the reproductive age group was 9,214. Under-five and under-two age groups were estimated to be 8,139 and 2,828, respectively. The study was conducted from February 2 to April 21, 2022.
Study population and sampling techniquesAll mothers with index children aged 6–23 months old and living in Mettu town for at least six months were selected by a simple random sampling technique from the sampling frame. Mothers unable to respond due to illness were excluded.
The sample size was determined by using the single population proportion formula for a cross-sectional study, n = Z2pq/d2, considering a two-sided confidence level of 95%, a power of 80%, and a margin of error of 5%. The prevalence of CCF feeding among mothers of children aged 6–23 months old was taken as 50% because there is no published data from the previous study in the area. Accordingly, the calculated sample size was 384, and a total of 403 participants were selected by considering a 5% non-response rate.
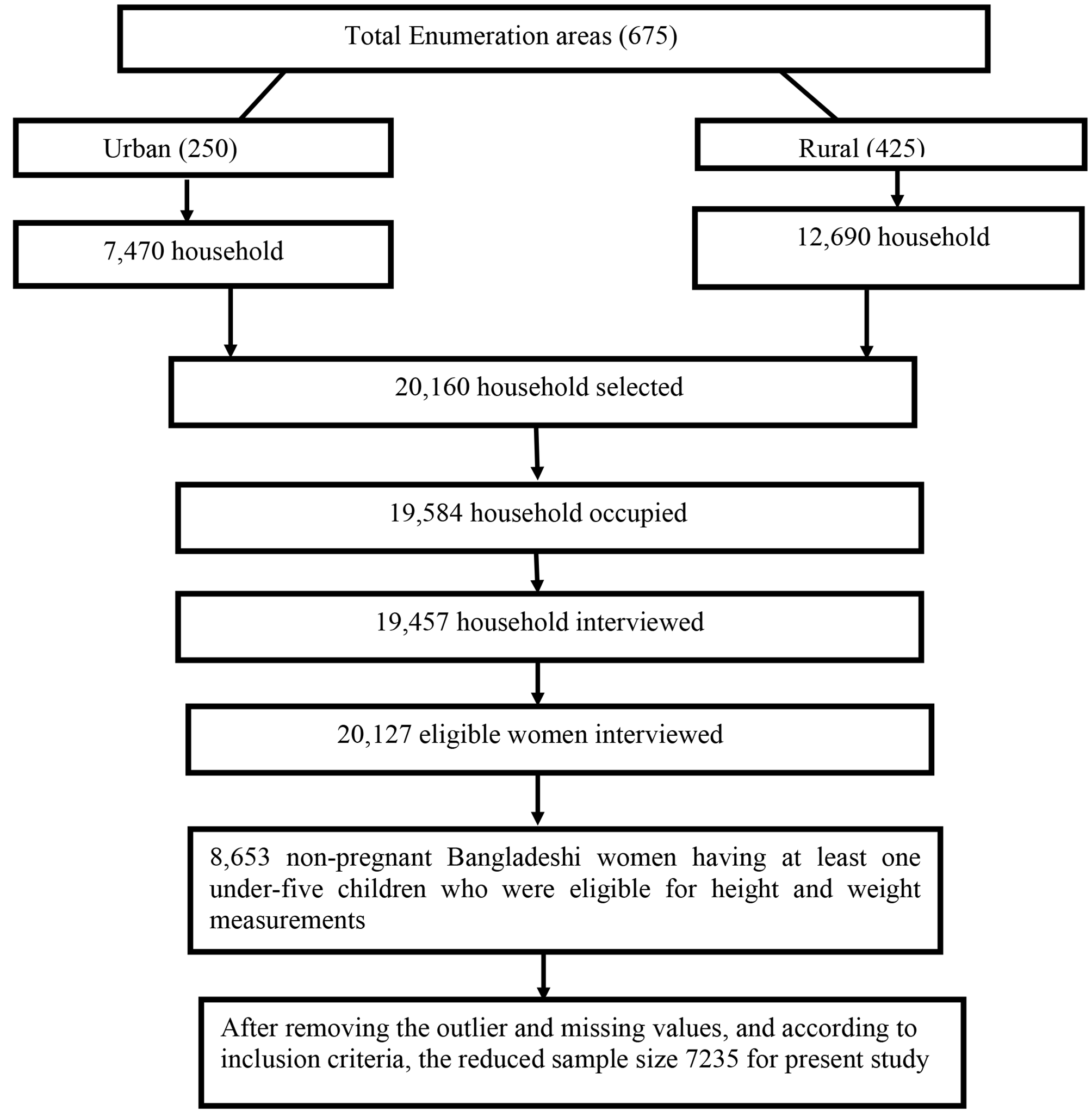
Before data collection, a list of mothers of children aged 6–23 months was collected from each kebeles in Mettu town. Accordingly, a sampling frame was prepared, and the required number of participants from each kebeles was determined based on proportion to population size allocation. Finally, a simple random sampling technique was employed to select 403 study participants from the six kebeles (Fig. 1).
Fig. 1
Schematic presentation of sampling procedure
Data collection tools and procedureA structured, pretested, and interviewer-administered questionnaire was used to collect the data. The questionnaire was adapted from the World Health Organization (WHO), the Food and Agriculture Organization (FAO), and UNICEF guidelines and questionnaires [21,22,23]. The questionnaires consist of socio-demographic characteristics (age, sex, marital status, religion, educational status, wealth status, and occupation), maternal health service-related characteristics, child characteristics, early child feeding practices, and CCF practices.
The knowledge was measured using seven dichotomous questions aimed at gathering information regarding the impact of CCF feeding on a child’s overall health, its influence on their food preferences, the potential for contamination, and their understanding of its higher sugar content, added preservatives, and additives. The answer to each question was analyzed as know and don’t know. The mean score was calculated to report the knowledge level of the study participants. Participants who scored mean and above were categorized as having good knowledge, and those who scored less than the mean score were categorized as having poor knowledge.
To assess the attitude, participants were asked questions consisting of eight items centered around their views on whether CCF aids child growth, the convenience of using CCF, their contentment with feeding CCF to their child, and their endorsement of the notion that CCF enhances the child’s cognitive abilities. Each question was measured on a five-point Likert scale, which ranges from strongly agree to strongly disagree. Each scale was summated to evaluate the overall score, which represents the respondent’s position on the continuum of favorableness towards CCF feeding. Accordingly, 8 items have a potential minimum sum score of 8 to a maximum sum score of 40. When the total score of the participant is close to 40, it shows the most favorable attitude, and when the score is close to 8, it shows the most unfavorable attitude towards CCF feeding. Thus, based on this continuum of favorableness, it was categorized as negative if they scored between 8 and 23, neutral for those who scored 24, and positive for those who scored above 24.
Data were collected by six trained health extension workers and two experienced BSc Nurse supervisors who supervised the overall process of data collection. Data was collected by a house-to-house visit of mothers with an index child aged 6–23 months old. In the event that the eligible mother was absent from the home at the time of data collection, a revisit was done, and the mother who was absent at the third re-visit was considered a non-respondent.
Operational definitionsComplementary feeding: is the process of starting additional foods and liquids along with breast milk.
Commercial complementary foods: foods marketed as suitable for feeding young children if they met at least one of the following criteria: (1) Marketed for introduction at an age of below three years; (2) labeled with the words “baby,” “toddler,” “young child,” or synonym; or (3) in any other way were presented as being suitable for children under the age of three years [24].
Commercial complementary food feeding: feeding the child any CCF products on the day before the interview.
Data quality assuranceData were collected using pre-tested and properly designed questionnaires. To assure data quality, the questionnaires were prepared in English and translated into Afan Oromo and Amharic, then translated back to English by another person to check for consistency. Pre-testing of the questionnaires was performed using 5% of the sample size on mothers with similar socio-demographic characteristics living in Hurumu town, which was not the actual data collection area. Based on the pre-test, modifications were made to the questionnaire. The training was given to data collectors and supervisors on the aim of the study, data collection tools, data collection techniques, approach to the interviews, and maintaining the privacy and confidentiality of the respondents. Every day after data collection, questionnaires were reviewed and checked for completeness by the supervisors and principal investigator, and the necessary feedback was given to the data collectors each morning.
Data processing and analysisAll data were checked visually, coded, and entered into Epi-data version 4.6 and exported to SPSS version 25 software packages for analysis. Descriptive statistics were calculated for variables. The results were presented in the form of tables, charts, and text using frequencies and summary statistics such as mean, standard deviation, and percentage to describe the study population with relevant variables. The degree of association between dependent and independent variables was assessed using an odds ratio with a 95% confidence interval. A simple binary logistic regression analysis was performed to select candidate variables for multivariable analysis. Variables with a P-value < 0.25 were taken as a cut-off point to select eligible variables for the multivariable logistic regression analysis, and variables with a p-value < 0.05 were declared as statistically significant in the final model. Pseudo-regression was performed to check the multi-collinearity between independent variables. For the final multivariable logistic regression model, the adequacy of the model to predict the outcome variables was checked by the Hosmer-Lemeshow goodness-of-fit test.
留言 (0)