
Remember me



This study was a 12-week non-randomised intervention of adults at increased risk of metabolic and cardiovascular disease (described as “index individuals”), enriched for Māori participants. The study population also included the household/whānau members living with the index individual. It was conducted at the Centre for Endocrine, Diabetes and Obesity Research (CEDOR) in Wellington, and at Kōkiri Marae in Lower Hutt, New Zealand. As part of supporting Māori research capability building, Tū Kotahi Māori Asthma and Research Trust was supported to lead the delivery of the intervention through Kōkiri Marae Health and Social Services. The trial was registered with the Australian New Zealand Clinical Trials Registry: ACTRN12621000856819p. The study was approved by the New Zealand Health and Disability Ethics Committee: 21/NTA/113.
ParticipantsThe study aimed to recruit 30 index individuals and their household/whānau. Index participants were recruited if they met the following inclusion criteria: Adults aged 18–70 years, metabolic syndrome (defined as MetSSS > 3.5), and at least one (and up to eight) household/whānau members agreeing to participate. A cut-off MetSSS of 3.5 was chosen as it reflected a point above which cardio-metabolic disease was more likely in the New Zealand population [14]. Individuals were not eligible to participate if they met any of the exclusion criteria: previous bariatric surgery; pre-existing Type 1 or Type 2 diabetes (two HbA1c results ≥ 50 mmol/mol minimum three months apart [22]); stage 4/5 renal disease; severe food allergy; current pregnancy or breastfeeding, or planning to conceive during the study; unstable body weight (active weight loss/gain > 5 kg in previous three months); gastrointestinal disorder that alters the digestion and absorption of nutrients (e.g. coeliac disease, ulcerative colitis, Crohn’s disease, an ileostomy or colostomy);; medications that modify blood sugar levels.
RecruitmentParticipants were recruited at two sites. Tū Kotahi, which delivers health and social services through Kōkiri Marae, aimed to recruit 10 Māori participants and their whānau through their existing networks. The other 20 participants were to be recruited through CEDOR by advertising to the general public through relevant email lists. All those who expressed interest in the study were assessed for eligibility using a two-step process. First, a telephone screening call including the calculation of the Australian Type 2 Diabetes Risk Assessment Tool (AUSDRISK) score, a screening tool that identifies people at risk of type 2 diabetes [23]. This was used to maximise the likelihood that those invited to the second part of screening would meet the study inclusion criteria. Individuals who had an AUSDRISK score ≥ 12 were then invited to attend the research centre in person for questionnaires and measurement of variables to calculate their MetSSS. Those who met all of the inclusion were enrolled in the study. The household/whānau members were then also invited to attend at visit 2. Informed consent was obtained from all the participants and their legal guardians, and assent from children under the age of 16 years, prior to any data collection.
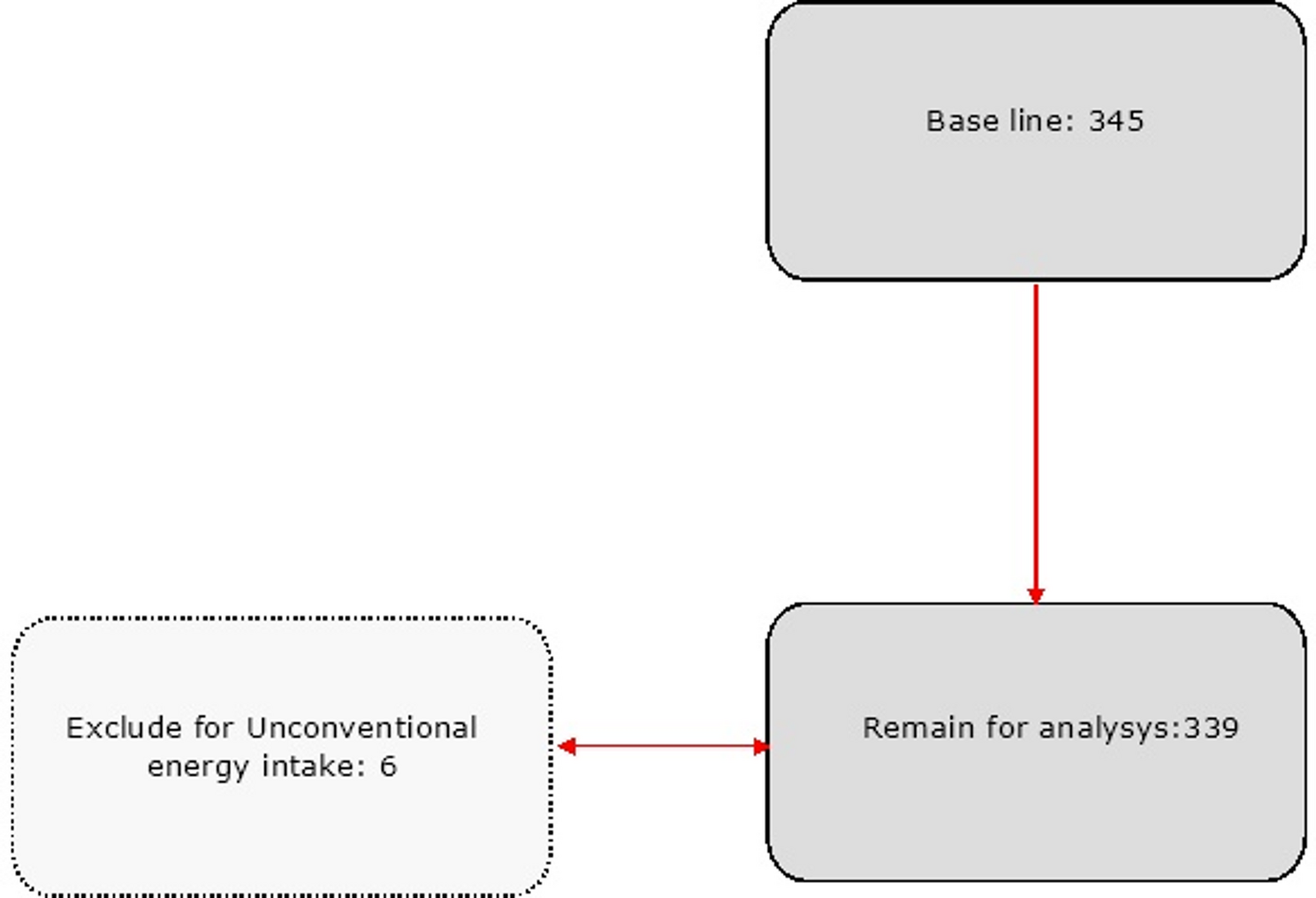
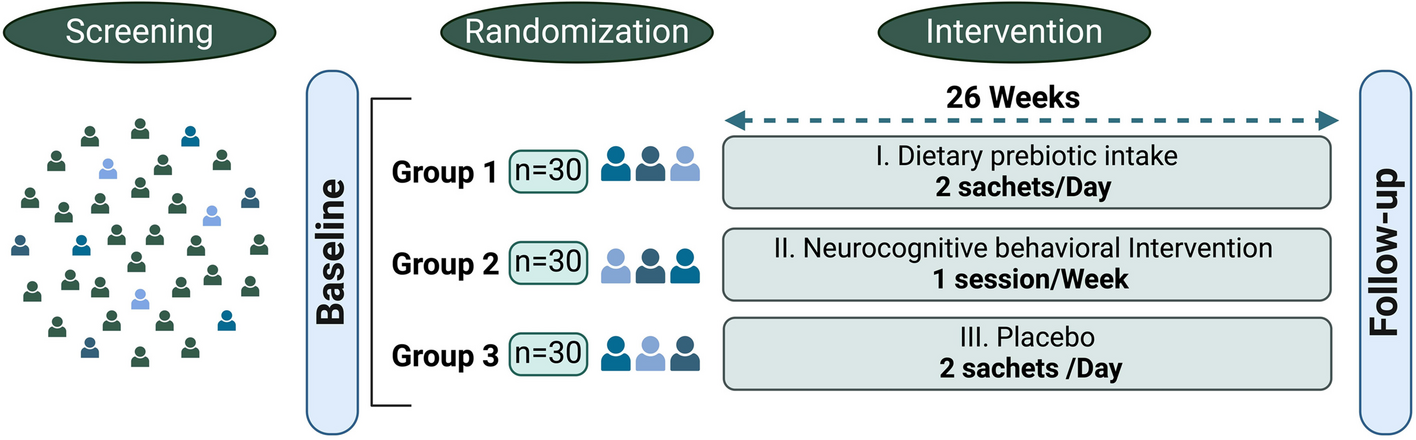
Study visitsParticipants attended study visits at baseline and 12 weeks (Fig. 1). Both visits comprised anthropometric measurements, fasting venous blood tests and a dietary intake questionnaire (Table 1). Medical conditions and history were recorded at baseline and current medications were recorded at baseline and 12 weeks.
Fig. 1 Table 1 Visit measures and questionnairesDietary intervention
Table 1 Visit measures and questionnairesDietary interventionParticipants were provided with a range of foods that are consistent with an adapted version of the Mediterranean dietary pattern and nuts were provided instead of olive oil [4]. Foods provided were assessed for their nutrient content and provided at a level that would meet the threshold for 75% of the nutrient reference values required for chronic disease risk reduction.
Dinner meal kits and a weekly grocery box containing foods that participants could use for lunch, breakfast and snacks were delivered by a commercial meal kit home delivery company specifically:
A box containing ingredients and recipes for 5 dinners. Participants had no choice in the meals that they received; these were selected by the meal kit company nutritionist as those meals that best met the Mediterranean Dietary pattern criteria. Participants were permitted to have some general dietary preferences that were taken into account, e.g. no pork. A fruit box containing approximately 15 pieces of seasonal fruit. A box containing foods for breakfast, lunch and snacks selected by the study nutritionists, namely cereal, yoghurt, eggs, wraps, rice, tuna, lentils, chickpeas, feta cheese, carrots, coleslaw, spinach, cucumber, tomatoes, muesli bars, nuts, pumpkin and sunflower seeds, and dried apricots, and included recipes and meal suggestions. Participants could not choose the contents of the box.
The diet was assessed against the PREDIMED diet criteria and met 11 out of 14 points [24]. The dietary pattern did not score points that would otherwise have been allocated for consumption of wine, sofrito (tomato sauce), four or more tablespoons of olive oil per day, and three serves of fish per week (two were provided in the weekly diet), but these were considered impractical in the context of the current study.
Participants were provided with dietary information that aligns with the NZ Ministry of Health Eating and Activity Guidelines [25], to guide their selection of non-provided foods that would make up their complete dietary intake. No other dietary counselling or behaviour change support was provided. Food was provided for the whole household regardless of how many participated in the study measurements.
Outcome measuresThe outcomes of this study were focused on feasibility questions for conducting a future trial.
1.Recruitment rates (time to recruit 30 participants, proportion of patients screened versus enrolled).
2.Proportion of household/whānau agreeing to enrol, average size of household/whānau.
3.MetSSS and other clinical parameters at baseline and 12 weeks. This included blood pressure, waist circumference, weight, height, body mass index (BMI), and body composition (bioimpedance), HbA1c and lipids.
Feasibility of the meal kit home delivery service; this included the utility of the distribution method and the acceptability of intervention for individuals and for household/whānau members. Fortnightly surveys were emailed to participants through the meal kit company using their Survey Monkey platform for the first 10 weeks of the study asking (i) if they had eaten all the food provided, (ii) what the reason was for not consuming items, and (iii) what changes would improve the meal kit for their household/whānau (supplementary file 1). The responses were compiled into a single document and inductive thematic analysis was carried out using NVivo (release 1.5.2 (946)). An informal exit interview was conducted at the 12 week visit where the participants were invited to reflect on the intervention and the food delivery. These comments were recorded and collated.
The relevant formulae used for calculating MetSSS were:
Male:
-5.4559 + (0.0125 × Waist Circumference (cm)) - (0.0251 × HDL (mmol/L) ×38.67) + (0.0047 × Systolic Blood Pressure) + (0.8244 × log(TAG (mmol/L) ×88.57)) + (0.0106 × Glucose (mmol/L) ×18)
Female:
-7.2591 + (0.0254 × Waist Circumference (cm)) - (0.0120 × HDL (mmol/L) ×38.67) + (0.0075 × Systolic Blood Pressure) + (0.5800 × log(TAG (mmol/L) ×88.57)) + (0.0203 × FPG1×18)
The multiplier preceding the clinical variable is the coefficient taken from the original publication for the MetSSS for non-Hispanic white and the multiplier after the clinical variable is the conversion factor from SI units to the units used in the original publication [26].
Sample size and analysisThe main determinant of the sample size in this feasibility study was to enable reasonably precise estimation of the SD for the proposed primary outcome variable; the MetSSS, for a sample size calculation in a definitive future trial. A sample size of between 20 and 30 gives between 19 and 28 degrees of freedom to estimate the SD giving reasonable precision. Therefore the aim was to recruit 30 index participants.
The analysis for MetSSS was by a paired t-test and estimation of the confidence interval for the SD by an F-test. SAS version 9.4 was used.
Comments (0)