
Remember me





Because multisystem inflammatory syndrome in children (MIS-C) was first described among pediatric patients in April and May of 2020,1,2 treatment regimens and guidelines for MIS-C have evolved. After the recognition of these first cases, the Centers for Disease Control and Prevention (CDC) released a health advisory about MIS-C and shared an initial case definition.3 As details about MIS-C were still limited, public health organizations such as the American College of Rheumatology,4 American Academy of Pediatrics5 and others recommended a treatment regimen closely after that for Kawasaki disease (KD).6 Increased clinician experience and differing presentations in clinical manifestations or severity influenced when and what treatments MIS-C patients received, resulting in different treatments provided across institutions.
This article describes treatments administered to patients with MIS-C at 4 children’s hospitals in the United States during the first 12 months of the COVID-19 pandemic and compares the use of these treatments and subsequent outcomes among patients with varying demographic and clinical characteristics.
METHODSData were derived from The Phenotype Initiative, a project that conducted both retrospective and prospective enrollment of patients admitted with MIS-C between March 16, 2020 and March 10, 2021. Enrollment sites included Arnold Palmer Hospital for Children in Orlando, Florida, Children’s Healthcare of Atlanta in Georgia, Phoenix Children’s Hospital in Arizona and Saint Louis Children’s Hospital—Washington University in Missouri. Medical records from initial hospitalization and follow-up medical encounters were abstracted using a single case report form, which included patient demographics, underlying medical conditions, signs and symptoms, diagnostic and treatment information, and clinical outcomes.
Patient SampleAll enrolled patients were less than 21 years old at the time of MIS-C onset. To assess the timing of treatment, patients were divided into 2 groups—those hospitalized between March 16, 2020 and October 22, 2020, and from October 23, 2020 to March 10, 2021. This date represents the median date of hospital admission within the study cohort. Each site began admitting patients in March, June, July and August of 2020, and the last patient admission was recorded on March 10, 2021. Patients were classified into 3 disease severity categories: (1) patients who received intensive care unit (ICU)-level care; (2) non-ICU patients with cardiac complications; and (3) non-ICU patients without cardiac complications. Recipients of ICU-level care were classified as such if they were admitted to the ICU, received treatment with a vasoactive medication, were intubated or placed on mechanical ventilation, or were placed on extracorporeal membrane oxygenation (ECMO). Patients not meeting these criteria for ICU-level care were classified as non-ICU patients and divided into 2 groups based on the presence or absence of cardiac complications. Finally, we assessed treatments administered by groups according to common organ system involvement of MIS-C. These included the presence of gastrointestinal (ie, abdominal pain, vomiting or diarrhea), hematologic (ie, elevated d-dimer, lymphopenia or thrombocytopenia), mucocutaneous (ie, rash, lesions or conjunctival injection), respiratory [ie, cough, shortness of breath, chest pain or tightness, pneumonia, acute respiratory distress syndrome or pleural effusion], and cardiac involvement [ie, shock, elevated brain natriuretic peptide (BNP) or N-terminal prohormone BNP (NT-proBNP), elevated troponin, congestive heart failure, cardiac dysfunction, myocarditis, coronary artery aneurysm or dilatation, hypotension, pericardial effusion or any mitral regurgitation].
Guidelines and TreatmentsSite-specific treatment guidelines for the management of patients with MIS-C were developed and updated throughout the study period as treatment standards changed. The day of hospital admission was considered day 0. Patient-level data regarding the date of first and second administration of intravenous immunoglobulin (IVIG), start and end dates of steroid and aspirin administration, and peak dosing of each treatment were collected from medical record review. Given that different types of steroids (ie, methylprednisolone, prednisone, prednisolone, hydrocortisone and dexamethasone) were administered to patients at different hospitals, a corticosteroid dosage equivalency chart7 was used to standardize steroid dosage to methylprednisolone dosage in mg/kg/day. Steroids and aspirin were considered “high-dose” if the dosage was ≥10 mg/kg/day and low-dose if the dosage was <10 mg/kg/day. Timing of administration and dosage were also collected for immune modulators (defined as anakinra, tocilizumab, rituximab and sirolimus) and vasoactive or inotropic medications, when applicable. Finally, details about discharge medications were also collected.
Patient OutcomesOutcomes assessed were: length of stay (LOS) ≥8 days, receipt of ICU-level care, presence of shock or hypotension, treatment with immune modulators (a surrogate for refractory illness),4 and the presence of certain cardiac complications defined as arrhythmia, pericarditis, myocarditis, congestive heart failure, elevated troponin and additional complications observed on multiple echocardiograms conducted during or posthospitalization [ie, mitral regurgitation (mild, moderate or severe), coronary artery abnormalities (dilatation or aneurysms), ventricular dysfunction (of left, right or both ventricles) or a left ventricular ejection fraction <50%]. Coronary artery dilatation and aneurysm were defined by z-score classification guidelines for aneurysms in patients with KD.6 Patients with coronary artery dilatation had a z-score ≥2 and <2.5, whereas those with aneurysms were classified into 3 categories—small (z-score ≥2.5 and <5), medium (z-score ≥5–<10 and absolute dimension <8 mm), and large (or giant) (z-score ≥10 or absolute dimension ≥8 mm). Elevated troponin was defined as >0.04 ng/ml. Shock or hypotension was defined as a clinical diagnosis of shock or receipt of vasoactive or inotropic medications.
Propensity Score MatchingTreatment effectiveness was assessed for IVIG and low-dose steroids, as those were common first-line treatments for patients with MIS-C. Analyses were conducted to determine if receipt of these treatments within 1 day of hospitalization, separately or in combination, was associated with a lower risk of subsequent severe outcomes at 2 or more days after hospitalization. Severe outcomes of interest were: ICU-level care, shock/hypotension, coronary artery abnormality, any ventricular dysfunction, any mitral regurgitation, increased troponin levels (troponin that was elevated and continued to increase up to or after day 2 of hospitalization), hospital LOS ≥8 days, and receipt of immune modulators. Propensity score matching was used to generate comparable analytic groups of patients by similar demographic and clinical presentations for each treatment comparison, using optimal full matching (incorporating both matching and weights for matched patients) with distance measured through logistic regression.8 The variables used in the matching algorithm were determined in a prior study9 to be associated with risk of ICU admission: patient age, presence of cough, shortness of breath, abdominal pain, elevated D-dimer, elevated BNP or NT-proBNP, elevated troponin, elevated C-reactive protein, elevated ferritin, elevated interleukin-6, thrombocytopenia, lymphopenia and date of MIS-C symptom onset. Instead of the date of MIS-C symptom onset, we considered the timing of hospital admission on or before and after the median date of admission (October 22, 2020) to be associated with the risk of ICU admission because admissions early in the pandemic were known to be associated with more severe outcomes.9,10 Analyses assessing the use of IVIG within 1 day of hospitalization additionally matched for the use of low-dose steroids within 1 day of hospitalization, and vice versa. Patients receiving high-dose steroids or immune modulators within 1 day of hospitalization were excluded from these analyses, as these are not common first-line treatments. The estimated relative risk (RR) with a 95% confidence interval (CI) of each outcome given the treatment group was calculated using quasi-Poisson generalized linear modeling, controlling for all variables used in the matching algorithm.
StatisticsDifferences in categorical variables were computed using χ2 tests (or Fisher exact tests for comparisons with expected cell sizes below 5). All data were stored in a secure REDCap database, and data cleaning and analyses were conducted using R version 4.1.2, RStudio version 2022.02.3, and Microsoft Excel. This study was approved by each site’s institutional review boards. This activity was reviewed by CDC and was conducted consistent with applicable federal law and CDC policy as defined in 45 Code of Federal Regulations §46.102(I)(2).
RESULTSA total of 233 patients with MIS-C were enrolled in the study, 151 (64.8%) from Hospital A, 37 (15.9%) from Hospital B, 23 (9.9%) from Hospital C and 22 (9.4%) from Hospital D (Table 1). The median age of patients at the time of MIS-C onset was 9 years (IQR, 5–13 years). Among all patients, the most frequently administered treatments were at least 1 dose of IVIG (77.7%), any dose of steroids (88.4%) and any dose of aspirin (81.1%). The least frequently administered treatments were immune modulators (8.2%), noninvasive ventilation (eg, continuous positive airway pressure, bilevel positive airway pressure) (8.2%), mechanical ventilation or intubation (5.2%) and ECMO (1.7%) (Table 1). The proportion of patients at each hospital who received at least 1 dose of IVIG ranged from 67.5% to 100%. Similarly, the proportion of patients receiving low-dose steroids (45.9%–84.8%) and high-dose steroids (5.3%–45.9%) also varied between hospitals (Table 1).
TABLE 1. - All Treatments Administered to Patients With MIS-C by Institution, From March 16, 2020 to March 10, 2021 Treatment All Patients (N = 233), n (%) Hospital A*IVIG and any dose of steroids administered on the same day.
†The category for steroids is inclusive of all patients who received low- or high-dose steroids, which are presented in the 2 subsequent rows.
‡The category for aspirin is inclusive of all patients who received low- or high-dose aspirin, which are presented in the 2 subsequent rows.
§Anticoagulants administered included prophylactic and treatment doses but were not distinguished from each other for this study.
¶Immune modulators are defined as anakinra, tocilizumab, rituximab or sirolimus.
‖Modes of noninvasive ventilation are defined as continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP).
ECMO indicates extracorporeal membrane oxygenation; IVIG, intravenous immunoglobulin.
Table 2 shows the demographic characteristics of patients who received standard treatments for MIS-C.6 Patients 13–20 years old (64.3%) were less likely to receive 1 dose of IVIG compared with patients 0–5 (83.1%) and 6–12 years old (81.2%). Furthermore, males (83.1%) were more likely to receive 1 dose of IVIG compared with females (68.2%). Patients 6–12 years of age were more likely to receive high-dose aspirin (30.4%), whereas patients 13–20 years old (10.7%) were least likely to receive high-dose aspirin. Non-Hispanic, Black patients (39.8%) were least likely to receive IVIG and steroids in combination, and patients with unknown race (81.8%) were most likely to receive combination treatment. High-dose steroids were more frequently administered to Hispanic or Latino patients (28.3%) compared with patients of other races and ethnicities. No statistically significant difference by age group, sex, or race/ethnicity was observed among patients who received 2 doses of IVIG or low-dose steroids (Table 2).
TABLE 2. - Number and Percentage of Patients Receiving Treatments for MIS-C by Demographic Characteristics (N = 233) At Least One Dose of IVIG Two Doses of IVIG IVIG and Steroids* Low-dose Steroids High-dose Steroids High-dose Aspirin Age (years) 0–5 (n = 65) 54 (83.1) 7 (10.8) 39 (60.0) 46 (70.8) 11 (16.9) 16 (24.6) 6–12 (n = 112) 91 (81.2) 12 (10.7) 50 (44.6) 85 (75.9) 16 (14.3) 34 (30.4)* 13–20 (n = 56) 36 (64.3)† 5 (8.9) 25 (44.6) 38 (67.9) 9 (16.1) 6 (10.7)* Sex Male (n = 148) 123 (83.1)† 12 (8.1) 77 (52.0) 102 (68.9) 28 (18.9) 37 (25.0) Female (n = 85) 58 (68.2)† 12 (14.1) 37 (43.5) 67 (78.8) 8 (9.4) 19 (22.4) Race/ethnicity Non-Hispanic, white (n = 52) 39 (75.0) 5 (9.6) 28 (53.8) 40 (76.9) 5 (9.6) 11 (21.2) Non-Hispanic, black (n = 98) 73 (74.5) 11 (11.2) 39 (39.8)† 71 (72.4) 12 (12.2) 27 (27.6) Hispanic or Latino (n = 60) 48 (80.0) 6 (10.0) 33 (55.0) 39 (65.0) 17 (28.3)† 12 (20.0) Other‡ (n = 12) 11 (91.7) 1 (8.3) 5 (41.7) 10 (83.3) 1 (8.3) 3 (25.0) Unknown§ (n = 11) 10 (90.9) 1 (9.1) 9 (81.8)† 9 (81.8) 1 (9.1) 3 (27.3)*IVIG and Steroids administered on the same day.
†Percentage of patients in a demographic category receiving a specified treatment significantly differs from the percentage of patients in other demographic categories receiving the same treatment (P < 0.05). For example, patients of age 6–12 were compared to patients of ages 0–5 and 13–20. χ2 or Fisher exact two-sided P value if any expected cell counts were below 5.
‡Patients identified as American Indian/Alaska Native (n = 2), Asian (n = 5), Multi-race (n = 3) or Other (n = 2).
§11 patients did not report their race or ethnicity.
IVIG indicates intravenous immunoglobulin; MIS-C, multisystem inflammatory syndrome in children.
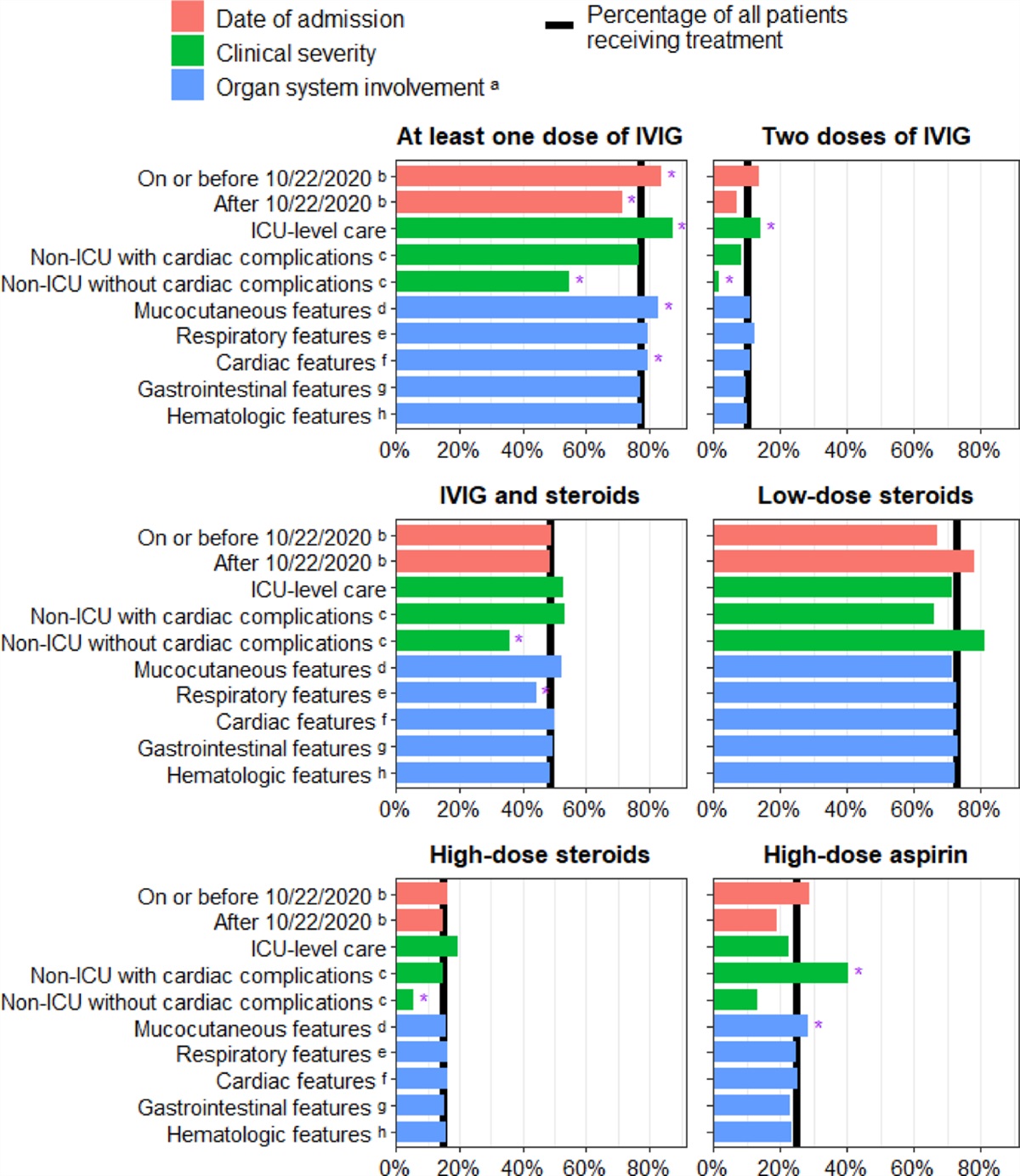
Patients admitted on or before October 22, 2020 were more likely to receive 1 dose of IVIG (83.9%) compared with patients admitted after this date (71.3%, Fig. 1). Patients receiving ICU-level care were more likely to receive at least 1 dose of IVIG (87.2%), 2 doses of IVIG (14.3%) and high-dose steroids (19.5%) compared with non-ICU patients. Non-ICU patients with cardiac complications were most likely to receive high-dose aspirin (40.4%), whereas non-ICU patients without cardiac complications were least likely to receive at least 1 dose of IVIG (54.7%), 2 doses of IVIG (1.9%), IVIG and steroids in combination (35.8%) or high-dose steroids (5.7%). Among all patients in the sample who received ICU-level care, 77.4% had cardiac complications, and 50.4% were 6–12 years old.
 FIGURE 1.:
FIGURE 1.: Percentage of patients receiving treatments for MIS-C by date of admission and clinical characteristics. *Percentage of patients in a demographic category receiving a specified treatment significantly differs from the percentage of patients in other demographic categories receiving the same treatment (P < 0.05). For example, patients receiving ICU-level care were compared with all non-ICU patients, regardless of the presence of cardiac complications. χ2 or Fisher exact two-sided P value if any expected cell counts were below 5. aOrgan system involvement categories are not mutually exclusive. bThe cutoff date of October 22, 2020, for timing of hospitalization, reflects the median date of hospital admissions among all patients. cCardiac complications are defined as arrhythmia, pericarditis, myocarditis, mitral regurgitation (mild, moderate or severe), coronary artery abnormalities (dilatation or aneurysms), elevated troponin, congestive heart failure, ventricular dysfunction (left, right or dysfunction in both ventricles), or a left ventricular ejection fraction less than <50%. dMucocutaneous features include the appearance of rash, mucocutaneous lesions, or conjunctival injection. eRespiratory features include cough, shortness of breath, chest pain or tightness, pneumonia, acute respiratory distress syndrome (ARDS), or pleural effusion. fCardiac features include shock, elevated brain natriuretic peptide (BNP) or N-terminal prohormone BNP (NT-proBNP), and elevated troponin. gGastrointestinal features include abdominal pain, vomiting, or diarrhea. hHematologic features include elevated d-dimer, lymphopenia or thrombocytopenia. Lymphopenia was defined as a lymphocyte count of <4500 cells per µl for infants <8 months, or less than 1500 cells per ml for persons ≥8 months of age. ICU indicates intensive care unit; IVIG, intravenous immunoglobulin; MIS-C, multisystem inflammatory syndrome in children.
Treatments also differed among patients with and without clinical features by organ system. Patients with mucocutaneous features were more likely to receive at least 1 dose of IVIG (82.8%) or high-dose aspirin (28.4%) compared with patients without mucocutaneous features (64.1% received IVIG and 12.5% received high-dose aspirin) (Fig. 1). Patients with respiratory features were less likely to receive IVIG and steroids on the same day (44.1%) compared with patients without respiratory features (59.7%). Finally, patients with cardiac features received at least 1 dose of IVIG more frequently (79.6%) compared with patients without cardiac features (41.7%). Administration of treatments did not significantly differ among patients with or without gastrointestinal or hematologic features (Fig. 1).
TABLE 3. - Details of Treatments Administered to Patients With MIS-C, From March 16, 2020 to March 10, 2021 (N = 233) Patients Treated,*Days from hospital admission (i.e., treatments given on the same day as hospitalization would be listed as 0).
†Patients who received immune modulators were administered anakinra, tocilizumab, rituximab or sirolimus. Three patients were discharged home with anakinra and 1 patient was discharged home with sirolimus.
IQR indicates interquartile range; IVIG, intravenous immunoglobulin.
All treatments, excluding second dose of IVIG, vasoactive medications and immune modulators, had a median day of administration of day 1 after hospital admission (Table 3). The median day of treatment for the second dose of IVIG and immune modulators was day 3. The median duration of treatment for patients who received high-dose steroids was 5.5 days compared with 4 days for patients who received low-dose steroids. All patients who received high-dose steroids during hospitalization were discharged home with steroids. The median dose of low- and high-dose steroids administered to patients with MIS-C was 2 mg/kg/day and 22.4 mg/kg/day, respectively (Table 3).
The 181 patients who received at least 1 dose of IVIG were more likely to exhibit elevated troponin levels (72.9%), experience shock or hypotension (70.7%) and receive ICU-level care (64.1%) compared with patients who did not receive IVIG. The 24 patients who received 2 doses of IVIG were more likely to have experienced shock or hypotension (87.5%), received ICU-level care (79.2%) and had an LOS of ≥8 days (70.8%) compared with patients not receiving 2 doses of IVIG. Furthermore, 169 patients who received low-dose steroids were more likely to have elevated troponin values (72.2%) but less likely to have received immune modulators (3.6%) compared with patients not receiving low-dose steroids. Patients who received high-dose steroids (36 patients) were significantly more likely than patients not receiving high-dose steroids to experience shock or hypotension (83.3%), but less than half required a hospital LOS of ≥8 days (47.2%) and less than one-third required treatment with immune modulators (30.6%). Coronary artery abnormalities were more common for patients receiving high-dose aspirin (33.9%) (Fig. 2, details of abnormalities in Table, Supplemental Digital Content 1, https://links.lww.com/INF/F204). Additional data related to patient demographics and severe outcomes are found in Table, Supplemental Digital Content 2, https://links.lww.com/INF/F205.
 FIGURE 2.:
FIGURE 2.: Prevalence of severe outcomes of MIS-C by treatment regimen at day 2 or later of hospitalization a . aTreatment regimens are not mutually exclusive. Percentages reflect the proportion of patients with severe outcomes within each treatment category. bPatients with an outcome of shock/hypotension experienced shock, were hypotensive and received vasoactive medications, or received vasoactive medications regardless of shock or hypotension. cPatients who were intubated or placed on mechanical ventilation are a subset of patients who received ICU-level care. dAny ventricular dysfunction is defined as dysfunction of the left, right or both ventricles. eAny mitral regurgitation is defined as mild, moderate or severe regurgitation. fCoronary artery abnormalities are defined as dilatation or aneurysm indicated by z-score. g Immune modulators administered included anakinra, tocilizumab, rituximab, or sirolimus. ICU, intensive care unit; IVIG, intravenous immunoglobulin; LOS, length of stay.
After propensity score matching to adjust for potential confounding, we observed that patients receiving IVIG within 1 day of hospitalization had a lower risk of having hospital LOS of ≥8 days (RR = 0.53, 95% CI: 0.31 –0.88) and a borderline lower risk of subsequently receiving immune modulators (RR = 0.38, 95% CI: 0.14–1.02) compared with patients who did not receive IVIG within 1 day of hospitalization (Fig. 3). Patients receiving low-dose steroids within 1 day of hospitalization were significantly less likely to have subsequent ventricular dysfunction (RR = 0.45, 95% CI: 0.26–0.77), increasing troponin levels (RR = 0.55, 95% CI: 0.40–0.75) or hospital LOS of ≥8 days (RR = 0.46, 95% CI: 0.29–0.74) compared with patients who did not receive low-dose steroids within 1 day of hospitalization (Fig. 3). Similarly, Figure 4 shows the RR of severe outcomes given the administration of both IVIG and low-dose steroids within 1 day of hospitalization. Compared with patients receiving only low-dose steroids within 1 day of hospitalization, patients receiving IVIG and low-dose steroids within 1 day of hospitalization were less likely to experience subsequent coronary artery abnormalities (RR = 0.05, 95% CI: 0.01–0.20). Additionally, compared with patients receiving only IVIG within 1 day of hospitalization, patients receiving IVIG and low-dose steroids in that timeframe were less likely to have increasing troponin (RR = 0.53, 95% CI: 0.40–0.71). The number of patients included in each comparison and the comparison of risk ratios before and after propensity score matching are shown in Table, Supplemental Digital Content 3, https://links.lww.com/INF/F206 and Table, Supplemental Digital Content 4, https://links.lww.com/INF/F207, respectively.
 FIGURE 3.:
FIGURE 3.: Relative risk of subsequent outcomes for patients with MIS-C receiving IVIG or low-dose steroids within 1 day of hospitalization compared with patients not receiving these treatments within 1 day of hospitalization, using propensity score matching to account for demographic and clinical confounding variables. aPatients who received ICU-level care stayed in the ICU for 1 or more days, received treatment with a vasoactive medication, were intubated or placed on mechanical ventilation, or were placed on extracorporeal membrane oxygenation (ECMO). bPatients with an outcome of shock/hypotension experienced shock, were hypotensive and received vasoactive medications, or received vasoactive medications regardless of shock or hypotension. cCoronary artery abnormalities are defined as dilatation or aneurysm indicated by z-score. dVentricular dysfunction is defined as dysfunction of the left, right or both ventricles. e Mitral regurgitation is defined as mild, moderate or severe regurgitation. fTroponin that was elevated (>0.04 ng/ml) and peaked at 2 or more days after hospitalization. gImmune modulators administered included anakinra, tocilizumab, rituximab or sirolimus. ICU, intensive care unit; IVIG, intravenous immunoglobulin; MIS-C, multisystem inflammatory syndrome in children.
 FIGURE 4.:
FIGURE 4.: Relative risk of subsequent outcomes for patients with MIS-C receiving both IVIG and low-dose steroids within 1 day of hospitalization compared with patients only receiving 1 of these treatments within 1 day of hospitalization, using propensity score matching to account for demographic and clinical confounding variables. *Calculation did not converge (risk ratio was not able to be estimated). aPatients who received ICU-level care stayed in the ICU for 1 or more days, received treatment with a vasoactive medication, were intubated or placed on mechanical ventilation, or were placed on extracorporeal membrane oxygenation (ECMO). bPatients with an outcome of shock/hypotension experienced shock, were hypotensive and received vasoactive medications or received vasoactive medications regardless of shock or hypotension. cCoronary artery abnormalities are defined as dilatation or aneurysm indicated by z-score. dVentricular dysfunction is defined as dysfunction of the left, right or both ventricles. eMitral regurgitation is defined as mild, moderate or severe regurgitation. fTroponin that was elevated (>0.04 ng/ml) and peaked at 2 or more days after hospitalization. gImmune modulators administered included anakinra, tocilizumab, rituximab or sirolimus. ICU, intensive care unit; IVIG, intravenous immunoglobulin; MIS-C, multisystem inflammatory syndrome in children.
DISCUSSIONThe present study highlights differences in treatment practice for patients with MIS-C during the first year of the pandemic by institution and by patient demographics and clinical characteristics. Importantly, when controlling for demographic and clinical characteristics, administration of IVIG and low-dose steroids within 1 day of hospitalization, separately or in combination, was associated with a lower risk of certain severe outcomes.
Treatment practices varied greatly across hospitals. For example, some hospitals administered IVIG for more severe cases who experienced KD-like symptoms or cardiovascular involvement, whereas others preferred to treat all patients with IVIG, regardless of severity. It is also possible that the infrequent use of IVIG as a first-line treatment in some hospitals was related to concerns about IVIG shortages during the initial phases of the pandemic. We also observed variations in the number of patients receiving 2 doses of IVIG and anticoagulants across hospitals. Higher rates of administration of both treatments may have been related to greater illness severity of patients. Finally, as treatment guidelines continuously evolved during the study period, patients hospitalized at different times may have received different treatments.
Unadjusted analyses primarily showed that receipt of specific MIS-C treatments was largely driven by patient clinical profiles. Patients with more KD-like features such as young age, being male and having mucocutaneous symptoms showed a significantly greater likelihood of receiving at least 1 dose of IVIG. Patients presenting with severe disease typically received high-dose steroids or a second dose of IVIG and were more likely to experience shock or hypotension, require intubation or mechanical ventilation, receive immune modulators, and have longer hospital stays. By using propensity score matching, adjusted analyses, and temporally distinct treatments and outcomes, we estimated the effects of treatments on the risk of subsequent clinical outcomes. While some reports suggest that IVIG aids in clinical improvement and recovery of cardiac function from MIS-C,11 not all studies have shown a clear benefit of its use alone.12,13 Prior studies have demo
Comments (0)