
記住我
Dear Editor,
A 21-year-old woman presented with multiple, tiny, skin-coloured to hyperpigmented asymptomatic papules and depressions on bilateral palms for 6 months [Figure 1a]. The patient did not have any similar lesions elsewhere on the body. The lesions were slowly progressive and enlarging in size. Based on the clinical findings, palmar psoriasis, lichen planus, palmar wart, lichen nitidus and palmar porokeratosis were kept as differential diagnoses.
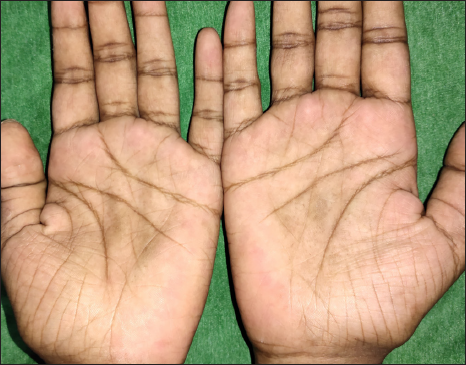
Figure 1a: Showing multiple tiny skin-coloured to hyperpigmented papules and depressions on the central aspect of both palms.
Export to PPT
Dermoscopic examination with polarising mode showed multiple well-circumscribed brownish-yellow depressed areas surrounded by a hyperpigmented rim. A few lesions showed fine peripheral scaling. A few punctate haemorrhages were also noted [Figure 1b].
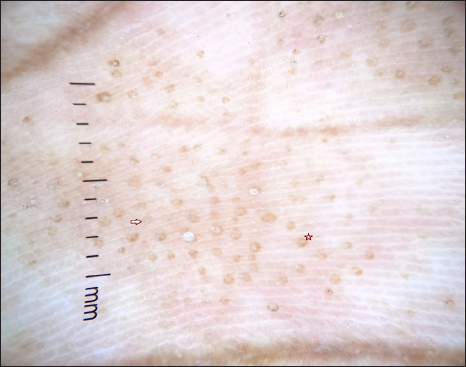
Figure 1b: Dermoscopic image (10×) with polarising mode showing multiple well-circumscribed brownish-yellow depressed areas surrounded by a hyperpigmented rim (star) and a few lesions showing fine peripheral scaling (arrow mark).
Export to PPT
Histopathological examination revealed thin epidermis with overlying parakeratosis, hypogranulosis and underlying basal layer degeneration along with expanded papillary dermis filled with lymphohistiocytic infiltrate [Figure 1c]. The dermoscopic and histopathological correlation was described in Table 1.
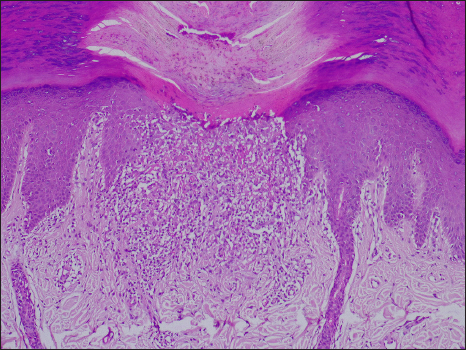
Figure 1c: Showing focal parakeratosis with underlying thin epidermis and expanded papillary dermis with lymphohistiocytic infiltrate (H&E, 100×).
Export to PPT
Table 1: Dermoscopic and histopathological correlation of palmar lichen nitidus
Dermoscopy Microscopy Brown-yellow depressed areas Dermal lymphohistiocytic infiltrate Hyperpigmented rim Peripheral elongated rete ridges Scales ParakeratosisA diagnosis of isolated palmar lichen nitidus was made and the patient was started on 0.1% betamethasone dipropionate ointment once daily. Currently, the patient is on regular follow-up and the lesions are resolving.
Lichen nitidus is most commonly located on the trunk, genitalia and extremities. Isolated palmar lichen nitidus is a rare manifestation. Both unilateral and bilateral palmar involvement has been described in the literature with different morphological presentations which include pruritic papules, asymptomatic pinhead-sized papules, pompholyx-like lesions, hyperkeratotic plaques, palmar pitting, fissuring and palmar purpura-like lesions.1
Clinically, the disease should be differentiated from palmoplantar psoriasis, palmar wart, pompholyx, hand eczema, palmar lichen planus, localised porokeratosis and pitted keratolysis. Table 2 describes the dermoscopic comparison of lichen nitidus of palms and its differentials. Jayasree et al. described multiple oval depressions and pits with yellowish plugs along the dermatoglyphics of the palm in a background of erythema. The elongated and acanthotic rete ridges enclosing circumscribed collection of lymphohistiocytic infiltrate give rise to the yellowish areas and dilated capillaries in the dermis contribute to the background erythema.2 Round erythematous depressions with dotted and linear vessels and yellow depressions interrupting linear parallel scales are other dermoscopic findings described.3
Table 2: Dermoscopic comparison of lichen nitidus of palms and its differentials
Clinical differentials Dermoscopic findings Histopathology Palmar psoriasis White scales, regular arrangement of dots and globular vessels. Parakeratosis with Munro micro abscesses and suprapapillary epidermal thinning. Palmar eczema Yellow scales, irregular arrangement of atypical vessels. Hyperkeratosis with focal parakeratosis, irregular elongation of rete ridges and spongiosis. Palmar wart Papillomatous growth, linear and dotted vessels. Epidermal papillomatosis with hyperkeratosis, hypergranulosis and koilocytes. Punctate palmoplantar porokeratosis White track structure in the periphery and homogenous brown globules in the centre. Cornoid lamella (tiers of parakeratotic columns) with underlying dyskeratosis. Palmar lichen planus Brownish areas, Wickham striae. Hyperkeratosis, hypergranulosis and basal layer degeneration with lichenoid, band-like infiltrate in the dermis. Pompholyx Featureless areas. Marked spongiosis along with spongiotic vesicle. Pitted keratolysis Black circles in parallel pattern. Crateriform defects (or pits) with bacteria within the corneal layer.Durusu et al reported a case of palmar lichen nitidus with multiple grouped hyperkeratotic papules and pitting over the palmar aspect of phalanges which on dermoscopy showed areas of comedo-like depressions encircled by white linear or halo-like scaling.4 In a case of purpuric variant of palmar lichen nitidus, punctate haemorrhages were observed on dermoscopy, which occurred as a result of hyalinisation of dermal capillaries and RBC extravasation.5
We report this case because lichen nitidus presenting with involvement of both palms alone is a rarity. Though this presentation is very uncommon, lichen nitidus should be kept as a differential in asymptomatic, isolated palmar lesions presenting with multiple tiny papules.
留言 (0)