
記住我


Diagnosis of ocular sarcoidosis recommended by IWOS, unless biopsy-proven, relies on various clinical and investigational criteria (Table 1). Most of the studies supporting these criteria or other potential sarcoidosis biomarkers included only adults. In clinical practice, in the absence of guidelines dedicated for children, the ocular sarcoidosis adults’ criteria are used also for the pediatric population. However, literature on ocular sarcoidosis biomarkers in children is very scarce or missing. Here, we resume the available data on systemic imaging modalities and biomarkers for ocular sarcoidosis relating to adults as well as to children.
Chest X-ray and chest computed tomography (CT) scanAdultsChest X-ray and/or chest computed CT scan are the mainstay imaging examinations in the diagnosis of granulomatous uveitis. Their role is to detect pulmonary changes characteristic for pulmonary sarcoidosis or tuberculosis. The findings that can support sarcoidosis diagnosis are bilateral hilar lymphadenopathy (BHL) and/or parenchymal lung changes. High resolution CT or CT with contrast were also described in patients with ocular sarcoidosis [52, 53].
In diagnosing presumed or probable ocular sarcoidosis, BHL and parenchymal lung changes are the criteria recognized by IWOS 2019. Chest X-ray and CT differ not only in their sensitivity and specificity in detecting this sarcoidosis related pulmonary features but also in availability and cost of the examination.
Chest X-ray still plays a role and its biggest advantage is low cost and availability. Chest X-ray was shown to be the second, after tuberculin skin test, most contributory investigation among the first step's systematic tests in patients with uveitis. Chest CT was placed among the second step's systematic tests in patients with uveitis, and among these it was a second most often contributory investigation, after HLA-B27 [54].
Chest CT was shown in many studies to have higher sensitivity (with similar specificity) in detecting BHL than chest X-ray. Nevertheless, for diagnosis of ocular sarcoidosis, even chest radiograph with its sensitivity 68% accompanied by specificity 96%, had high enough sensitivity to be considered as sufficient evidence of sarcoidosis among patients with uveitis [39]. In the same study, sensitivity of BHL on chest CT scan in patients with negative chest radiography results was 73% with high specificity 95%. Other recent studies showed lower chest X-ray BHL sensitivities in OS (57,1 -57,6%) (Burger 2021 57,1%, Niederer RL 2019, 57.6%) with 100% specificity. For comparison the chest CT scans BHL sensitivity for OS was higher and ranged from 85.7% [55] to 98.0% [35] with a specificity of 95.5%-100% [35, 55].
BHL, either by chest CT scans or chest X-ray, was found to be the most sensitive investigational finding in a study evaluating first IWOS ocular sarcoidosis criteria from 2009 [39].
Interestingly, BHL frequency is shown to significantly differ in an age-related manner in patients with uveitis associated with sarcoidosis. In Japan, older patients (> 65 years) with OS had BHL detectable in 52% and younger patients (≤ 65 years) in 78% of cases [56].
CT is also more sensitive in detecting parenchymal lung changes, another typical manifestation of pulmonary sarcoidosis [57]. Parenchymal lung changes consistent with sarcoidosis, as determined by pulmonologists or radiologists, is one of the revised IWOS criteria for suspected OS.
Parenchymal lung changes seen in chest CT scans can be seen both in sarcoidosis and tuberculosis. In one study, parenchymal involvement among patients with uveitis was observed more frequently in patients with tuberculosis than with presumed sarcoidosis [58]. Allegri et al. reported that among adult patients with definite and presumed ocular sarcoidosis, HRCT showed purely parenchymal involvement in 40% of patients and in 13,2% parenchymal involvement was combined with hilar and/or mediastinal lymphadenomegaly [40].
Children > 5 years and < 5 yearsThe sensitivity and specificity of various findings in chest imaging modalities in diagnosis of ocular sarcoidosis in children or in Blau syndrome is unknown.
However, in children of mean age 13 years with all types of sarcoidosis, bilateral hilar lymphadenopathy was shown to be the most frequent chest X-ray manifestation (78%) [1] Parenchymal involvement with or without BHL was less frequent (16%) [1]. Also, in contrast, enhanced chest CT in children with pulmonary sarcoidosis hilar/mediastinal lymphadenopathy was the most common finding [59].
In one study, among 13 children (median age 12 years old) with sarcoidosis-associated uveitis, none of the 3 patients with definite, biopsy-proven sarcoidosis in whom chest X-ray was performed, had chest X-ray consistent with sarcoidosis [41]. In the same study, 5 patients (39%) had X-ray consistent with sarcoidosis, and were classified as presumed or probable sarcoidosis following criteria established by authors [41].
In Blau syndrome, pulmonary involvement with interstitial lung disease (ILD) is rare but can occur [31, 60]. The studies do not specify presence of BHL in Blau syndrome, although generalized lymphadenopathy was observed in 52% of patients with Blau syndrome in one study [31].
Conclusion chest X-ray and chest computed tomography (CT) scanBoth chest X-ray and chest CT scan play an important role in detecting BHL and parenchymal lung changes that can support diagnosis of suspected ocular sarcoidosis in adults. They were proven to be the most sensitive investigations supporting diagnosis of OS in adults. In children, who have more often extrapulmonary sarcoidosis, there is no comparative data on chest X-ray and chest CT scan contribution to diagnosis of ocular sarcoidosis.
18F-fluorodeoxyglucose positron emission tomography imaging (FDG PET CT) and gallium-67 scintigraphyAdults18F-fluorodeoxyglucose positron emission tomography (FDG PET CT) and Gallium-67 scintigraphy are nuclear medicine imaging methods that use radiopharmaceuticals (FDG) or radioactive isotopes to detect increased inflammatory activity. 18F-fluorodeoxyglucose positron emission tomography indicates increased glucose uptake by macrophages and lymphocytes which indicates active sites of inflammation [61].
Although FDG PET CT has gained much more attention in the research in the last decade it is still not easily accessible everywhere, where Gallium-67 scintigraphy can still have its place. FDG PET CT advantages over Gallium-67 scintigraphy are increased contrast and resolution [62]. FDG PET CT was also shown to detect more pulmonary than non-pulmonary [63] or extra thoracic [64] sarcoidosis lesions than 67 Ga citrate scintigraphy.
Neither FDG PET CT nor Gallium-67 scintigraphy is recommended in standard systemic sarcoidosis workup. However, in cardiac sarcoidosis FDG PET CT is a second choice in a lack of cardiac MRI [61, 65].
Both Gallium-67 scintigraphy and 18F-fluorodeoxyglucose positron emission tomography are included in revised criteria for ocular sarcoidosis IWOS.
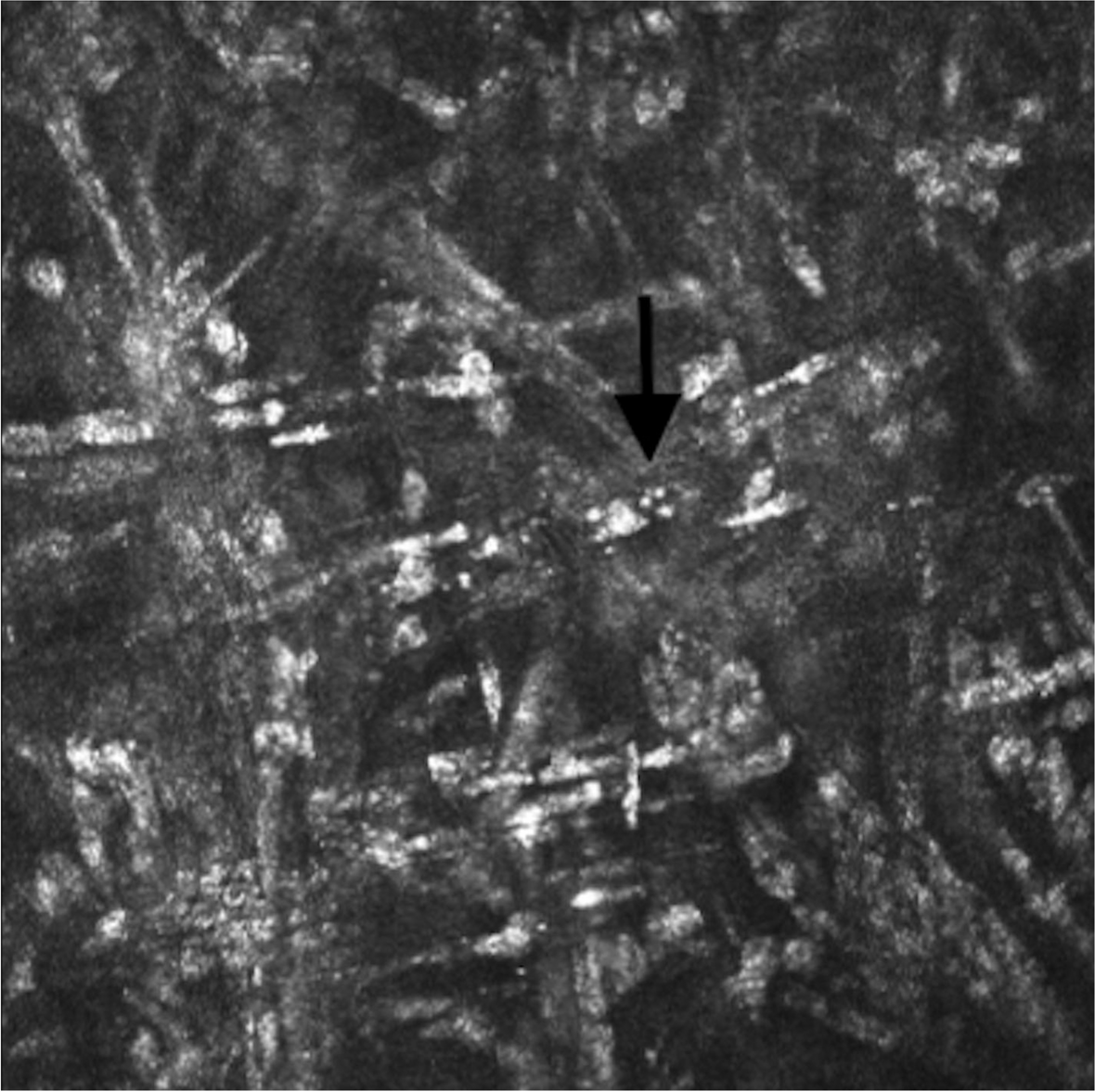
FDG PET CT’s main advantage is that it is a single whole-body examination that can detect various extrapulmonary sites of sarcoidosis [66]. In FDG PET CT and in Gallium-67 scintigraphy lambda sign and panda signs are used as characteristic signs [67, 68] for diagnosis of sarcoidosis. Moreover, other sites of FDG intake can also be helpful for diagnosis by indicating locations for accessible biopsies [66, 69] (Fig. 4A, B).
Fig. 4
Whole body 18F-FDG PET/ ultra low dose CT in a 11 year-old patient revealed abnormal 18F-FDG uptake not specific for an active granulomatous disease. A left axillary lymph node was biopsied and definite ocular sarcoidosis was diagnosed. A FDG PET/CT Fusion Coronal View. B FDG PET coronal view. Red and black arrows: Low hypermetabolic axillary bilateral lymph nodes
Opinions vary concerning the utility of FDG PET CT in ocular sarcoidosis in adults. Chauvelot et al., showed that FDG PET CT enabled the diagnosis of intraocular sarcoidosis even in patients with a normal CT scan [70]. However, Burger et al., did not observe additional benefit of FDG PET CT over chest CT in diagnosing suspected OS [55].
FDG PET CT’s sensitivity and specificity for ocular sarcoidosis are respectively 85.7% and 95.5%. Positive and negative predictive values for FDG PET CT for ocular sarcoidosis were also calculated to be 85.7% and 95.5% [55].
As far as gallium-67 scintigraphy is concerned, there is considerably less data related to ocular sarcoidosis. The combination of elevated ACE and a positive 67GA scan increased the diagnostic specificity to 100% without affecting sensitivity (73%) in patients with suspected ocular sarcoidosis and normal chest radiographs [71].
Children > 5 yearsFDG PET CT in pediatrics is a valuable diagnostic tool for fever of unknown origin (FUO) [72] leading to final diagnosis mostly of inflammatory (43%) or infectious (23%) origins, followed by malignancies (11%) [73]. FDG PET CT can also detect other granulomatous diseases such as intrathoracic and extra thoracic tuberculosis in children [74].
In children, a variety of strategies are possible to reduce the radiation dose while ensuring image quality [75]. These include CT attenuation correction and patient preparation.
Using ultra-low dose protocols in total body FDG PET CT is possible in children and should have special attention. Recently an ultra-low dose infection imaging using FDG PET CT was reported to be performed without sedation even in a newborn [76].
In diagnosing bilateral uveitis of undetermined origin in children, FDG PET/ ultra-low dose CT provided important information for final diagnosis in 30% patients [69]. In this study, for three pediatric patients the extra thoracic FDG intake showed biopsy accessible sites (cervical, axillary or inguinal lymph nodes) and led in 2 patients to biopsy proven, PET-CT guided ocular sarcoidosis (Fig. 4).
Children < 5 yearsNo studies were found on FDG PET CT in patients with Blau syndrome.
Conclusion 18F-fluorodeoxyglucose positron emission tomography imaging (FDG PET CT) and gallium-67 scintigraphyFDG PET CT and Gallium-67 scintigraphy have their place in diagnosing OS and abnormal intake and these imaging modalities are among the revised 2019 IWOS criteria in adults. In children, who have more often extra thoracic sarcoidosis presentations, a single whole body FDG PET/ ultra-low CT could be useful for final diagnosis in indeterminate uveitis as it can indicate places accessible for biopsy that are out of scope of thoracic CT. Nowadays, many strategies can be used to reduce the radiation dose, including PET/CT with ultra-low dose CT protocol which should be of special consideration in children.
CD4/CD8 ratio (> 3.5) in bronchoalveolar lavage fluidAdultsSystemic sarcoidosis diagnosis is supported by a CD4/CD8 ratio > 3.5 and lymphocytosis > 15% in bronchoalveolar lavage (BAL) fluid. However, BAL lymphocytosis alone is not specific for sarcoidosis as it is present in many other disorders, including hypersensitivity pneumonitis, nonspecific interstitial pneumonitis, or organizing pneumonia [77, 78]. Using CD4/CD8 ratio > 3.5 increases specificity for sarcoidosis to 93–96% but still does not have high sensitivity (53 to 59%).
Other authors cited by Kraaijvanger et al. showed a wider range of BAL CD4/CD8 ratio sensitivity (54—80%) with lower specificity (59—80%) [62].
In revised IWOS criteria, elevated CD4/CD8 ratio (> 3.5) in bronchoalveolar lavage fluid (BAL) was recognised as one of systemic investigations for diagnosing suspected ocular sarcoidosis. The sensitivity and specificity of CD4/CD8 ratio (> 3.5) in BAL in diagnosing ocular sarcoidosis was not reported in the literature. However, there are studies showing its importance in diagnosing ocular sarcoidosis even in patients with normal chest imaging [79] including high-resolution computed tomography (HRCT) [80]. Another study showed that positive BAL findings were present in 67.3% of adult patients with definite and presumed ocular sarcoidosis [40].
Children > 5 years and < 5 yearsIn children as well as in adults, BAL can be performed under sedation and topical anesthesia and using flexible bronchoscopy [81]. However, serial BAL is not routinely recommended in pulmonary sarcoidosis in children in whom BAL lymphocytosis does not correlate with disease activity and treatment response [3].
There is no data on the utility of CD4/CD8 ratio (> 3.5) in BAL in ocular sarcoidosis in children or in Blau Syndrome.
Conclusion CD4/CD8 ratio (> 3.5) in bronchoalveolar lavage fluidIn adults, testing CD4/CD8 ratio (> 3.5) in bronchoalveolar lavage fluid (BAL) can be considered in diagnosing suspected ocular sarcoidosis, as stated in revised IWOS criteria. However, its character needing at least sedation and topic anesthesia do not place it as a first-choice diagnostic examination. Furthermore, in children, it can be even less recommended due to lack of data regarding its utility in ocular sarcoidosis.
Serum Angiotensin Converting Enzyme (sACE)AdultsACE, studied in sarcoidosis since 1975, is the best-known serum biomarker in this disease. Serum ACE is an acid glycoprotein converting angiotensin I into angiotensin II. In the context of sarcoidosis ACE is produced by activated alveolar macrophages and correlates with granulomas burden [62]. Elevated sACE is also observed in ocular sarcoidosis, although no correlation was found between activity of sarcoidosis-associated uveitis and ACE [82].
Elevated sACE is one of the eight IWOS systemic investigations recommended as criteria for probable ocular sarcoidosis. However, it is not needed for definite or presumed ocular sarcoidosis (IWOS criteria 2019) nor for SUN Criteria for Sarcoidosis-Associated Uveitis) [7, 38]. sACE, as a sarcoidosis biomarker, is also mentioned among recent criteria of probable systemic sarcoidosis recommended by American Thoracic Society [65].
Elevated levels of sACE can be found not only in sarcoidosis but also in several other diseases, among which some can also have ocular manifestations eg. tuberculosis, leprosy, diabetes mellitus and histoplasmosis. sACE levels can be influenced by ACE inhibitors, corticosteroids use and cigarette smoking [33, 62, 83].
Notably, it was recently shown that genotype influences the sACE levels and some researchers advise to take ACE gene polymorphism into account while interpreting normal sACE levels for individuals. Taking into account the insertion (I)/deletion (D) polymorphism in the ACE gene can influence interpretation of 8,5% of measurements by either elevating or normalizing ACE values in patients with confirmed or suspected systemic sarcoidosis [84].
Sensitivity and specificity of sACE in ocular sarcoidosis varies among the studies. However, all recent studies are compatible with the fact that sACE has lower sensitivity than specificity, with sensitivity 48% and specificity 96% [50, 53, 83, 85, 86]. sACE had positive predictive value (PPV) of 44.9% and negative predictive value (NPV) 89.2% in diagnosing sarcoid uveitis [85].
To increase the sensitivity of sACE as a biomarker in ocular sarcoidosis, the combination with other biomarkers was tested leading to better sensitivity while keeping high specificity. The combinations of sACE and chest radiography, lymphopenia or sIL2R were studied and showed the following changes in sensitivity of combined examinations vs sensitivity of sACE alone. Combination of sACE and chest radiography showed increase of sensitivity (70% vs 30%) [82] as well as combination of sACE and sIL2R (75.0% vs 44.2%) [87]. Combination of sACE and lymphopenia showed an increase of sensitivity to 18.9% when compared with sensitivity of lymphopenia alone (15.3%) but showed a decrease in sensitivity when compared with sensitivity of sACE alone (45.8%) [85].
The standard cut off value of sACE for adults is 68 U/L. However, the optimal cutoff point for sACE levels in the population with uveitis was calculated to be 51 U/L [82]. The normal standard values may vary among the regions eg. in Japan standard sACE normal range is 7.0–25.0 IU/L [88] with recent proposition to change the cut-off value to 17.7 IU/L which would increase sensitivity of detecting sarcoidosis to 67.0% in Japan [88].
In a recent study of ocular sarcoidosis patients, the mean serum levels of ACE were 49.17 ± 29 IU/L versus 27.4 ± 15.34 IU/L in the control group of non-granulomatous (i.e., non-sarcoidosis) uveitis patients [50].
Children > 5 years and < 5 yearsAlthough, there is no study that determines sensitivity or specificity of sACE in children with ocular sarcoidosis, this biomarker is used in pediatric clinical practice. From a study in Louisiana on childhood sarcoidosis (n = 27) we know that ACE was elevated in 74% of sarcoidosis pediatric patients and among all patients in the study 77% children had uveitis [20]. Another study showed that among 13 children with probable, presumed, or definite sarcoidosis, 6 patients had elevated ACE levels [
留言 (0)