
Remember me

Aim 1 of this study will adapt C2C for use in VA primary care. We will use an iterative process that includes focus groups and semi-structured interviews with key stakeholders (veteran patients, primary care providers [physicians, social workers, and psychologists], and VA national policy leaders). In Aim 2, we will conduct a two-site, pilot randomized controlled trial to determine the feasibility of conducting a larger scale trial to test C2C’s effectiveness, determine the acceptability of C2C among primary care patients with HD + , and explore the efficacy of C2C to improve veterans’ initiation of and engagement in alcohol care, and their alcohol and mental health (PTSD, depression) outcomes, at 3-month follow-up.
Aim 1: adapt C2C for VA primary careProcedureTo achieve Aim 1, we will use an iterative method, ADDIE: Analysis, Design, Development, Implementation, and Evaluation [33], that is commonly used in the field of instructional design to develop educational content. Analysis refers to sharing with key stakeholders the intervention’s goals (improving initiation of and engagement with alcohol care to benefit outcomes) and identifying stakeholder needs within the context of the target setting (primary care) and population (patients with HD +). Design refers to adapting the prototype of the C2C protocol based on information gathered during the Analysis phase. Development is the process of producing a final version of C2C (to be tested in Aim 2) based on feedback from stakeholders on the prototype. Implementation refers to putting C2C into action, i.e., implementing the adapted version in the target setting, including training the Care Coach to deliver C2C in Aim 2. The Evaluation phase consists of a formative evaluation to obtain feedback from stakeholders on C2C to optimize its acceptability for use in Aim 2.
We will recruit 12 veterans who screen positive for HD + in primary care, 6–10 providers (primary care physicians and providers in integrated primary care-mental health), and 6–10 national policy leaders to participate in semi-structured interviews. Half of the veterans and providers will be recruited from each of the two study sites. Sample sizes were determined using recommendations for the number of interviews needed to obtain theoretical saturation, which is the point at which no new insights emerge from additional interviews [34, 35]. National policy leaders will include VHA experts in primary care medicine and in the treatment of mental health and substance use disorders.
Recruitment: patientsTo recruit veterans, we will use the VA Corporate Data Warehouse (CDW; a national level database housing clinical, administrative, and financial information) to identify potentially eligible veterans seen in primary care at each of the two sites. We will identify veteran patients with HD + : (1) an AUDIT-C score of ≥ 5 (used by VA to indicate HD) and (2) a positive screen for PTSD and/or depression, i.e., Primary Care PTSD Screen for DSM-V (PC-PTSD-5) score of ≥ 3 [36] and/or Patient Health Questionnaire-2 (PHQ-2) score of ≥ 3 [37] in a VA primary care visit within the past year. We will invite identified patients to participate in the study.
Specifically, we will randomly select a subsample of patients from the CDW dataset to mail opt-out invitation letters. We expect women will represent about 3–10% of identified patients. Potential participants will receive a study packet that includes an invitation letter, an informed consent document, and notification that we will contact them by telephone (should they not opt-out) 10 days following the mailing. The study will be presented to potential participants as research to learn more about VA and community resources to improve their health. Study staff will explain to potential participants that during a recent health care visit they answered questions about their alcohol use in a way that indicated possible difficulties around drinking. Research assistants will confirm eligibility of interested patients by re-administering screens to determine whether patients continue to meet screening criteria for HD + . Research assistants will also assess cognitive functioning using the Montreal Cognitive Assessment (MOCA) section on orientation [38]. Veterans unable to answer orientation items with reasonable accuracy and whose interview suggests likely cognitive impairment will be ineligible. Research assistants will answer questions about study participation and obtain informed consent from interested and eligible patients. Participants will be compensated for each in-person interview.
Recruitment: providersTo recruit providers, at each site, project staff will email providers to briefly explain the project’s purpose and invite them to contact the study team to complete an interview. Emails will be followed with a phone call to answer questions, obtain informed consent, and schedule interviews (in person or by phone, while on or off duty, as providers prefer). We will use similar procedures to recruit national policy leaders to complete phone interviews.
Interviews: data collectionIn the interviews, participants will be asked to review a handout, elaborated upon by the interviewer, providing a description of C2C. Interviewees will be asked about the core C2C components, such as which parts may be hard to understand, how to best inform patients with HD + about care options, and duration of the intervention (e.g., whether C2C provides enough monitoring). Interviews will help ensure that C2C components (e.g., length of time between sessions, how patients who do not want help are approached) are appropriate for use with veterans with HD + and for use within VA. Implementation-related questions will assess the feasibility of using well-established procedures (e.g., training, facilitation) for rolling out evidence-based interventions throughout VA [39]. Feedback obtained will inform efforts to implement C2C in VA primary care in a subsequent, fully powered hybrid trial. All interviews will be audio recorded and transcribed to facilitate data analysis.
Interviews: data analysisData collected from the interviews will be analyzed using a rapid analytic technique called template analysis, a method of team-based qualitative analysis, which organizes and summarizes data into predefined conceptual domains [40, 41]. Project staff will read all interview transcripts to identify participants’ opinions about C2C and obtain suggested modifications for adapting C2C to the target population and clinical setting. Prototype templates will be created in electronic documents containing broad conceptual domains (e.g., modifications to the content and/or structure of each C2C session, training needs of providers to learn C2C). After developing protocol templates, project staff will combine individual templates into a summary template, with content grouped into categories within each conceptual domain. To establish analytic validity, template content will be illustrated with verbatim quotations from participants, which will provide verification of the accuracy of content labelling and grouping. Results will be used to develop a final version of C2C for use in Aim 2.
Aim 2: examine C2C’s feasibility, acceptability, and efficacy in two-site pilot trialEligibilityTo be eligible for Aim 2, veterans (n = 140) will (1) have screened positive for HD + in the prior 12 months and have positive rescreens, (2) not have received ≥ 3 sessions of specialty substance use disorder treatment or participated in ≥ 2 weekly mutual-help groups in the past 30 days, (3) not have significant cognitive impairment, (4) have ongoing access to a mobile or landline telephone, (5) provide at least one contact who will know their contact information, and (6) not have participated in an interview for Aim 1.
RecruitmentFor a fully powered randomized controlled trial, we will need to recruit 360 Veterans (adjusting for an expected 75% retention rate at 6-month follow-up). Specifically, considering a medium effect size of C2C, a sample size of 360 will be needed to achieve 80% power to detect a treatment effect between groups (on care initiation) with a type 1 error rate of 0.05. To achieve a sample size of 360, we will need to recruit 10 veteran patients per month over a 36-month period. Therefore, in the planned pilot study, we will determine the feasibility of recruiting 10 Veterans per month (5 at each site, a rate of about one participant per week per site) over a 14-month period.
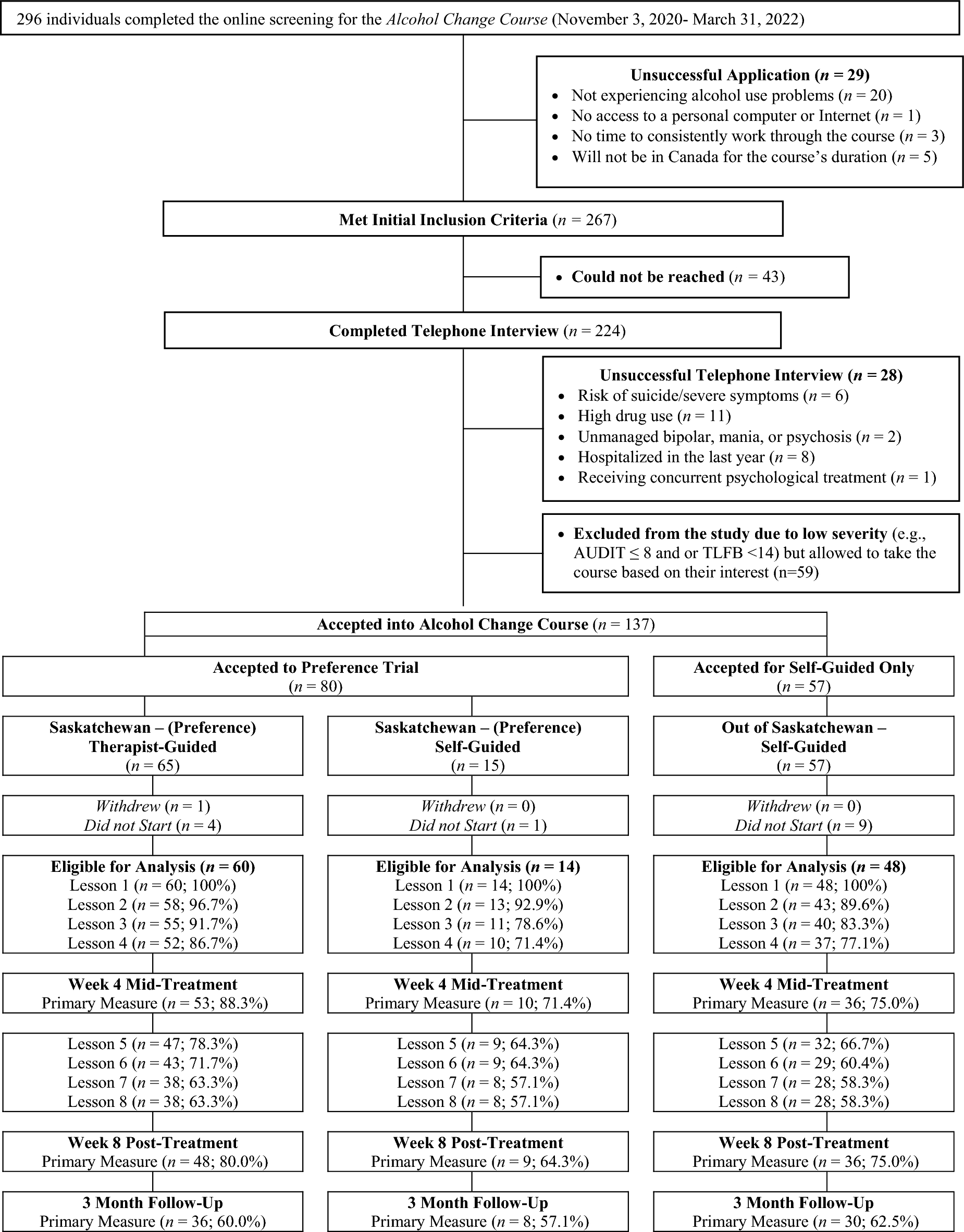
ProcedureRecruitment procedures for Aim 2 will follow procedures described for patients in Aim 1. Research assistants will confirm eligibility of interested patients by rescreening, using the same screeners, for HD + (to determine if they continue to meet study eligibility criteria) and determining eligibility on criteria that could not be prescreened with CDW data (cognitive function, have not participated in ≥ 3 alcohol treatment and ≥ 2 weekly mutual-help group sessions in the past 30 days, access to phone, available contact, non-participation in Aim 1). Patients who consent to participate will be randomly assigned to the UC or C2C condition using the Research Randomizer website after their baseline assessment. The flow of participants through the pilot trial is shown in Fig. 2.
Fig. 2
Flowchart of participants through the trial
UC conditionAll participants will be eligible to receive UC delivered by their VA primary care physician that includes mandated brief alcohol counseling and referral to specialty substance use disorder care according to VA practice guidelines.
C2C conditionVeterans assigned to the C2C condition will receive UC plus the C2C intervention. They will be contacted by the study Care Coach by phone to schedule their first session. C2C will provide up to five telephone or video conference sessions over seven weeks. Sessions will last about 30–60 min, depending on the participant’s specific needs.
Care coach training and supervisionThe same Care Coach will deliver C2C by telephone or video conference to participants at both study sites. The coach will participate in a two-day training on the C2C protocol and receive ongoing supervision. Training will begin with the rationale for the study, a review of the unique needs and challenges of veterans with HD + , and a summary of the literature on the effectiveness of strengths-based interventions, followed by observation and role-play exercises for delivering C2C and using the menu of alcohol care options. Specifics of the phone sessions will be reviewed: overall structure of each session; building rapport; how to discuss and assess personal strengths; identify whether the patient is interested in pursuing alcohol care; how to proceed if patients are not interested (continue encouraging, problem solving, monitoring) in care; how to proceed if patients are interested (present the menu of care options; help the patient choose an alcohol care option and support initiation); identify barriers to help-seeking and problem-solve solutions in a collaborative manner; and monitor progress. The coach will role-play phone and video conference sessions that will be audiotaped, coded for fidelity, and reviewed with supervision and feedback. After training, we will ensure the coach’s readiness to deliver C2C with a start-up practice phase. When the clinical supervisor agrees that the coach is consistently following the C2C protocol, the coach will be certified to begin conducting sessions with non-practice participants.
C2C fidelityTo assess the fidelity of the C2C intervention, the clinical supervisor will complete the C2C Fidelity Assessment [26], consisting of a checklist of core C2C components, after the first 10 phone calls (and 4 randomly chosen phone calls per month thereafter) between the Care Coach and participants. The C2C Fidelity Assessment will be modified to include content modifications arising from Aim 1. The coach will audio-record all sessions (with appropriate consent) so selected sessions can be evaluated for fidelity. Corrective feedback will be provided to the coach if needed. In addition, the coach will document any barriers or facilitators to intervention delivery that arise throughout the study.
MeasuresFeasibility will be measured as: (a) the proportion of veteran patients screening eligible for the study who enroll, (b) monthly enrollment rates compared to the benchmark of at least 10 patients per month, (c) participant 3-month follow-up rates compared to a benchmark of \(\ge \) 75%; and (d) C2C fidelity using the C2C Fidelity Assessment, i.e., a rating of \(\ge \) 80% completion of the basic core elements of C2C [42]. Acceptability will be operationalized as (a) > 50% of patients randomized to C2C complete at least three sessions [21] and (b) score of > 18 on patients’ satisfaction with C2C, assessed with the VA Multisite Study’s measure of satisfaction with substance use disorder treatment [43].
To explore C2C’s efficacy, we will collect the following data at baseline and 3-month follow-up (exceptions are noted).
Demographics: Age, sex, gender identity, race/ethnicity (baseline only), marital status, education, employment, income, and housing.
Alcohol consumption: 90-day Time Line Follow-Back (TLFB) [44]. The TLFB is a calendar-based, retrospective self-report measure that assesses quantity/frequency of alcohol consumed. It is reliable and accurate when administered over the telephone [44]. Alcohol quantity and frequency will be measured using days and percent of heavy drinking days (≥ 4 standard drinks per day for women; ≥ 5 for men). In addition, AUD diagnosis and severity will be measured using the 11 items in the DSM-5 [45, 46].
Depression: Patient Health Questionnaire-9 (PHQ-9) [47]. The PHQ-9 consists of nine questions that ask respondents how often they have “been bothered by any of the following problems” (with, e.g., sleep, energy, appetite) in the past two weeks (not at all = 0; nearly every day = 3) and are summed. Scores range from 0–27. Higher scores indicate more symptoms of depression. The PHQ-9 closely mirrors DSM criteria for depression and has excellent internal consistency and test–retest reliability.
PTSD: PTSD Checklist-5 (PCL-5) [48]. The PCL-5 is a 20-item self-report measure that assesses the 20 DSM-5 symptoms of PTSD. A total symptom severity score (range = 0–80) is obtained by summing the score for each item. Higher scores indicate more severe PTSD symptoms.
Drug use: Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) [49]. The ASSIST will assess lifetime (baseline only) and past 90-day drug use, i.e., use of illicit drugs (stimulants, inhalants, street opioids) and non-medical use of prescription drugs (opioids, sedatives).
Substance use and mental health care utilization (baseline only): Adapted version of the Addiction Severity Index (ASI) [50]. The ASI will be adapted to assess lifetime alcohol, drug, and mental health care utilization (VA and non-VA; baseline only).
Substance use and mental health care utilization (follow-up only): Adapted TLFB. The TLFB method will be adapted to determine the primary efficacy outcomes of initiation of and engagement in alcohol care. Initiation of alcohol care is a dichotomous variable (yes/no) with “yes” defined as the participant reporting at least one of the following: attended an initial meeting with an outpatient or residential program; attended a mutual-help group meeting; received > 30-days’ supply of AUD medication; or accessed ehealth for alcohol use. Engagement in alcohol care will be defined using two indices: the percentage of days in the past 90 that participants obtained any alcohol care; and the total number of alcohol care options participants obtained over the past 90 days (scores will range from 0 = no care to 4 = obtained all types of care: outpatient/residential, mutual-help, medication, e-health). CDW data will also identify use of VA substance use and mental health care including initiation of treatment, type of care and setting, and frequency and duration of each care type.
Mediators (see Fig. 1): Decisional conflict and motivation. Decisional conflict will be assessed with the Decisional Conflict Scale, a self-report measure used to assess decision uncertainty and discomfort [51, 52]. The scale’s 16 items yield five subscales (Informed, Values Clarity, Support, Uncertainty, Effective Decision) and a total score. The Readiness Ruler will assess motivation to initiate care [53]. It asks participants about their motivation to initiate alcohol care on a scale of 1 (less – not ready) to 10 (more – trying to seek care).
Assessment proceduresResearch assistants, blinded to condition, will collect baseline and follow-up data from participants over the telephone. Each assessment will take about one hour. We will use an intent-to-treat design and follow participants who do not complete the intervention. Participants will be compensated for completing the assessments. To ensure high follow-up rates we will use proactive retention strategies, e.g., interviewers are comfortable with the study population and trained to establish rapport; toll-free telephone numbers for participants to report contact information changes. We will use these procedures to target a follow-up rate of at least 75%.
Analysis planWe will examine the efficacy of C2C by comparing the two conditions (UC, C2C) on the primary outcomes of initiation of and engagement in alcohol care, and secondary outcomes of alcohol use, depression, and PTSD symptoms. To explore alcohol care initiation we will employ generalized estimating equations (GEE) or general linear models (GLM) using binomial distribution with logit link to determine whether participants differ by condition on alcohol care initiation at 3-month follow-up. To explore engagement in alcohol care we will use GEE or GLM models with cumulative logit or generalized logit to determine whether participants in the C2C condition had more engagement in alcohol care relative to UC over time. We will include a binary variable for study condition (C2C vs UC) and time for each assessment time point in the regression models and an interaction term between these two variables. Analyses for care engagement (percentage of days that alcohol care was obtained), alcohol (percent of drinking days and heavy drinking days), PTSD, and depression outcomes will be performed using GEE or GLM models to examine the effect of C2C over time. A normal distribution will be specified if an outcome is normally distributed; otherwise, an appropriate distribution (e.g., beta distribution for alcohol outcomes with percentages; gamma distribution for PTSD and depression outcomes) will be identified with the corresponding link specified. Variables for condition, time, site, and covariates will be included in all models along with the interaction term between condition and time. Models will be developed for each outcome separately.
We will also explore mechanisms (reasons C2C is effective) although the trial is not fully powered for this purpose. That is, decisional conflict and motivation to initiate alcohol care will be explored as potential mediators between condition and outcomes. We will use structural equation modeling (controlling for covariates) that corresponds to a hypothesized causal sequence among (1) C2C, (2) less decisional conflict and more motivation to seek alcohol care, (3) initiation of and engagement in alcohol care, and (4) alcohol, PTSD, and depression outcomes (Fig. 1). We will include the following paths simultaneously in the model: (1) condition (C2C vs UC) to decisional conflict and motivation to seek alcohol care, (2) decisional conflict and motivation to seek alcohol care to initiation of/engagement in alcohol care, and (3) initiation of/engagement in alcohol care to alcohol, PTSD, and depression outcomes. The dummy variables representing C2C and study site will be treated as exogenous; all other variables in the paths will be treated as endogenous. Other variables that are identified as strongly associated with condition at baseline may be included as exogenous. Model fit indices will be evaluated (e.g., RMSEA, SRMSR, CFI).
We will explore baseline levels of alcohol (probable AUD [AUDIT-C score > 8)] or not); PTSD (probable PTSD [PCL-5 score > 31] or not), and depression (moderate depression [PHQ-9 score > 10] or not) symptom severity as moderators of condition-outcome associations. We expect that all groups that receive C2C will benefit from it, but these analyses will provide data on whether C2C is especially helpful for patients with more or less severe baseline HD and PTSD and/or depression symptoms.
Debriefing interviewsAt 3-month follow-up, we will conduct in-person debriefing interviews with 20 participants assigned to the C2C condition to obtain data on its feasibility, acceptability, and perceived efficacy (including reasons C2C is or is not helpful). Interviews will be audiotaped and transcribed to facilitate analysis. Participants will be compensated for completion of the interview. Patients who receive < 3 C2C sessions (n = 14; 7 at each site) and patients who receive \(\ge \) 3 sessions (n = 6; 3 at each site) will be interviewed at the completion of their 3-month follow-up. In both subgroups, we will ensure that patients with probable AUD, probable PTSD, and at least moderate depression will be represented. Interviews will identify aspects of C2C that participants found helpful or not for initiating alcohol care and potential suggestions for improvement. Findings may inform strategies for deterring C2C dropout and improving C2C use and completion, as well as conceptual model development (e.g., identification of other potential mechanisms) of C2C.
Data collected from debriefing interviews will be analyzed using template analysis. Project members will read all interview transcripts to identify participants’ experiences participating in the C2C condition. Prototype templates will be created in electronic documents containing broad conceptual domains (e.g., what was your experience, what was helpful or not, what did you like and dislike) related to participating in C2C. Team members will combine prototype templates into a summary template (after reaching consensus on conceptual domains, aiming for 100% agreement) with content grouped into categories within each conceptual domain. The process of categorization will allow for the identification of experiences described by participants. To establish analytic validity, team members will illustrate template content with verbatim quotations from participants, which will provide verification of the accuracy of content labelling and grouping.
Comments (0)