Canada is facing an escalating epidemic of unregulated drug overdoses, with fatalities in unprecedented numbers. More than 42,000 opioid toxicity deaths occurred in Canada between January 2016 and September 2023 [1]. The province of British Columbia (BC) is the most severely affected, with an annual rate of 45.3 opioid toxicity deaths per 100,000 population compared with the Canadian average of 19.4 per 100,000 population in 2022 [1].
The major driver of the ongoing crisis of drug overdoses and deaths is the increasing toxicity of the unregulated drug supply, fueled by fentanyl and its analogues. Fentanyl, a potent opioid agonist, was developed in the 1950 s to fill a need for strong and rapid analgesia. Because of these characteristics, fentanyl is commonly used to treat chronic cancer pain or in anesthesia [2]. Initially present as an adulterant in unregulated drugs, especially heroin, fentanyl is now the substance of choice for many people with opioid use disorder (OUD) [3].
The harms associated with fentanyl use are related to its high potency and short duration of action, leading to very frequent use, severe cravings, and more difficult to manage withdrawal symptoms [2, 4, 5]. Fentanyl was involved in 82% of Canadian opioid toxicity deaths in 2023 [1]. In BC, fentanyl was detected (alone or in combination with other drugs) in 86% of unregulated drug toxicity deaths in 2021, a striking increase from 5% in 2012 [6].
Opioid agonist therapy (OAT) has been shown to be safe and effective for the treatment of OUD. When prescribed in therapeutic doses, OAT decreases morbidity and mortality due to overdose and other OUD-related harms including serious acute and chronic infections including human immunodeficiency virus (HIV) and hepatitis C [7]. However, the shift to fentanyl in the unregulated drug supply has significantly complicated the management of OUD. People who use fentanyl experience severe withdrawal symptoms, often compromising OAT initiation, retention and adherence [4, 8].
Effective OAT doses are highly variable, depending on a number of factors, including the individual’s opioid tolerance and interindividual variability in pharmacokinetics [9]. Unfortunately, assessment of opioid tolerance is challenging, and is typically subjective, relying on the patient’s self-report of the amount and frequency of their opioid use, and is further complicated by the unpredictability of the unregulated drug supply [4]. Unknown opioid tolerance increases the risk of opioid overdose with OAT, and sequential administration of methadone without reaching steady state may cause “dose stacking” and the potential for dose accumulation [10]. In view of these risks, current North American OUD treatment guidelines (developed when heroin was the dominant opioid in the unregulated market) take a cautious approach, recommending low starting doses and slow, gradual dose increases [7, 11]. The British Columbia Centre on Substance Use (BCCSU) and Ontario’s Mentoring, Education, and Clinical Tools for Addiction: Partners in Health Integration (META:PHI) initiative have updated their guidance to reflect the changing unregulated drug market, providing recommendations for more rapid, albeit still conservative methadone initiation and titration [10, 12].
However, as previously noted, fentanyl is highly potent and is being used in large doses. As a result, currently recommended oral OAT induction protocols provide an inadequate speed of OAT titration for a large proportion of individuals with OUD who use unregulated fentanyl. Prescribing OAT according to current recommendations is frequently associated with persistence of severe and recurrent cravings and withdrawal symptoms over the weeks to months before therapeutic target levels of OAT can be reached, with ongoing unregulated substance use during the lengthy titration period [4, 8]. Indeed, a recent analysis of BC health administrative datasets including more than 55,000 people with OUD showed that, while OAT engagement and retention were protective against hospitalization and death, methadone initiation in compliance with current clinical guidelines was associated with increased risk of death or hospitalization within the first 6 months [13]. Even maximum recommended OAT doses are often inadequate to meet the opioid requirements of people who use fentanyl, leading to poor retention in OAT programs and continued use of unregulated drugs, with their attendant risks of overdose and death, even among those who remain on OAT [4, 13, 14].
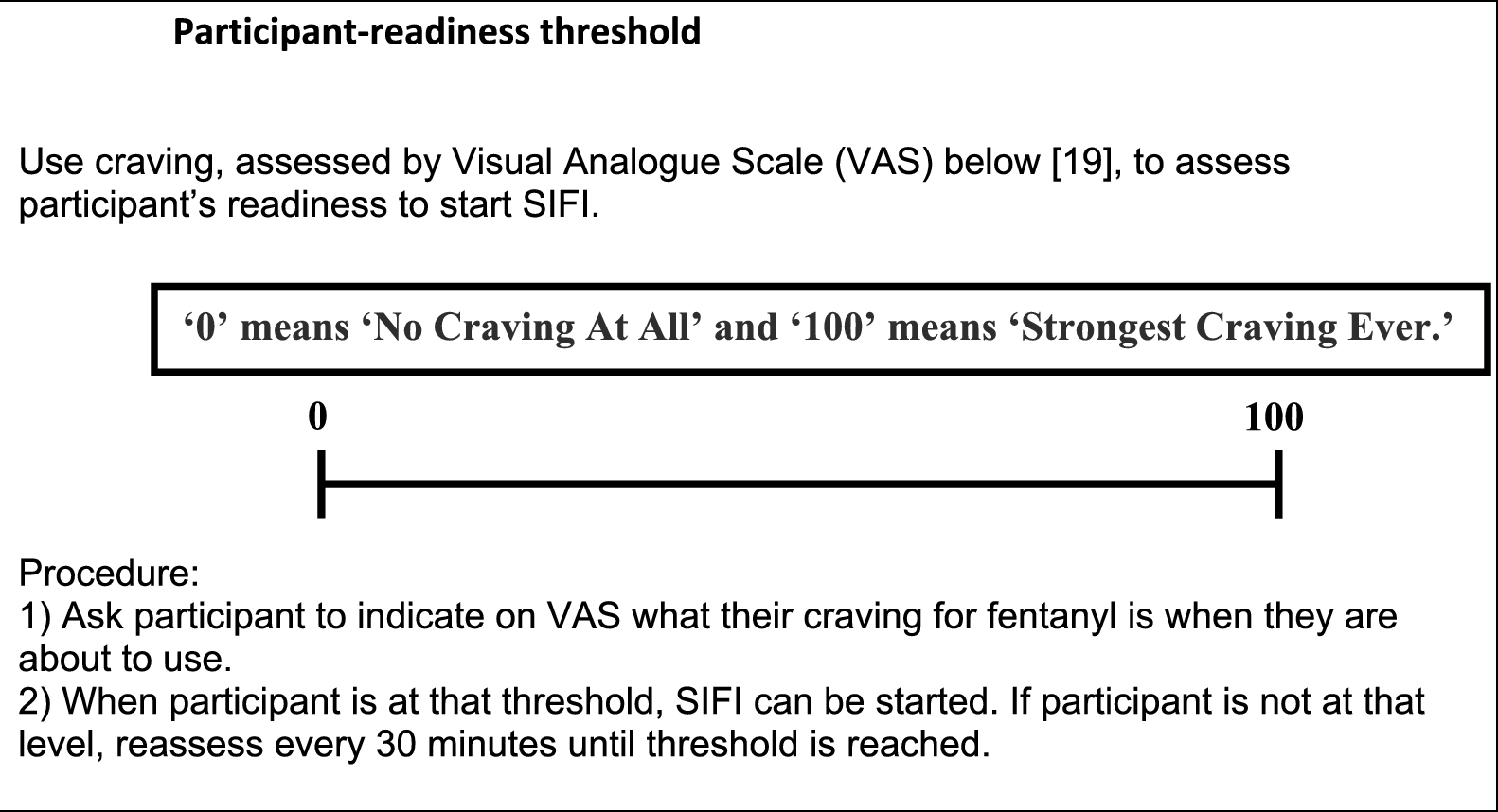
In an attempt to address this issue in the context of managing hospitalized individuals who use fentanyl, we pioneered a novel alternative induction protocol using a rapid intravenous symptom-inhibiting fentanyl induction (SIFI) for objectively determining opioid tolerance using medically-administered intravenous (IV) fentanyl [3]. Implementation of the SIFI protocol in hospitalized patients with OUD has proven feasible, safe, and effective in meeting the patients’ opioid requirements, and thereby effectively managing opioid withdrawal and averting patient-initiated discharge from hospital against medical advice. Herein we propose to conduct the first evaluation of the safety, efficacy, and acceptability of the SIFI protocol in an outpatient setting.
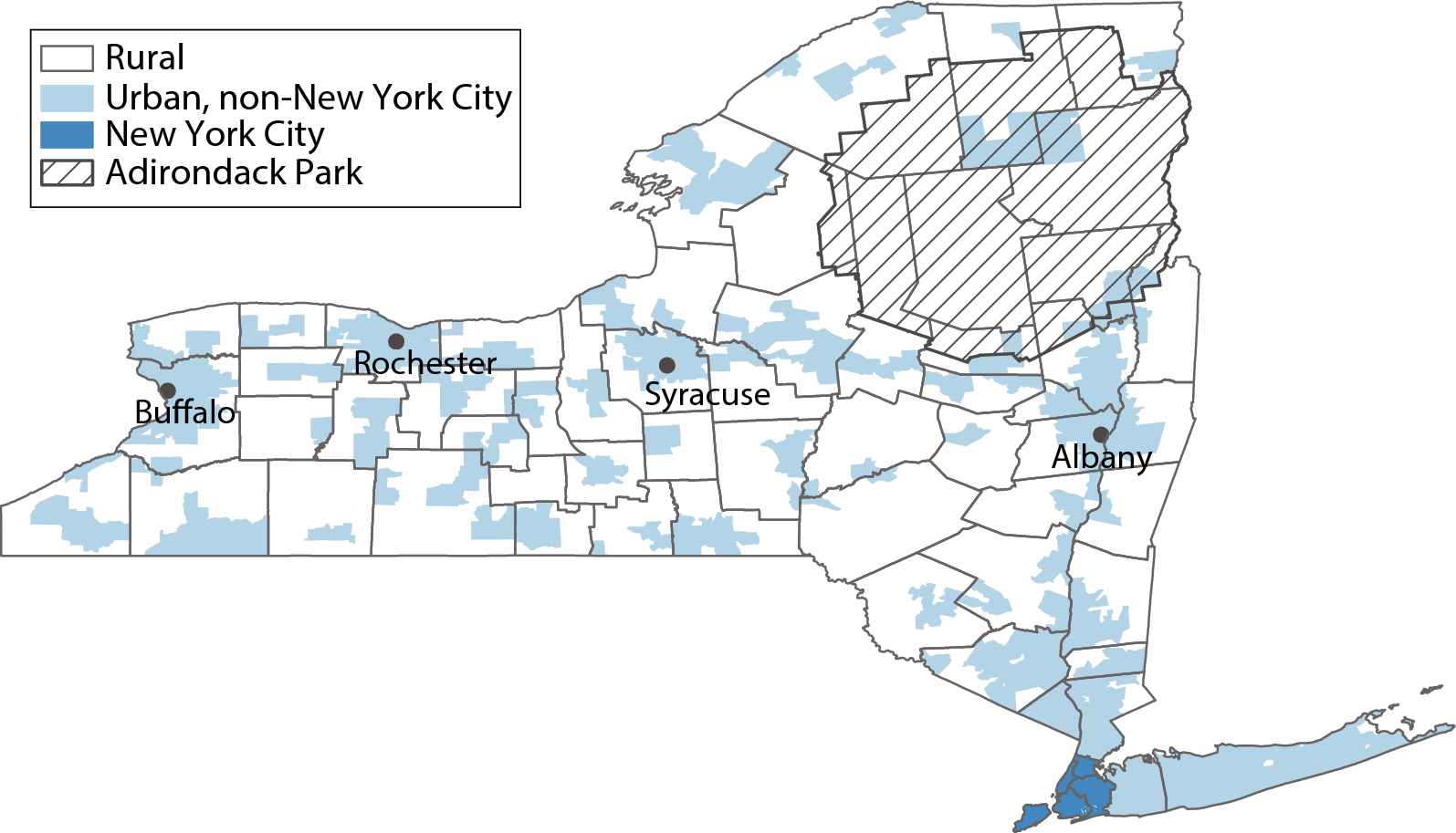
To this end, we will implement and evaluate our rapid IV fentanyl induction protocol among patients who use fentanyl and who are receiving services at Hope to Health, a community primary care clinic located in the Downtown Eastside neighborhood of Vancouver, the epicenter of the unregulated drug use epidemic in Canada.
In brief, we will use each individual’s calculated opioid tolerance to guide their transition onto OAT with oral methadone or sustained-release oral morphine (SROM), with the choice of agent based on a shared decision-making process between the patient and their clinician. Methadone or SROM starting doses will be individualized based on an objective assessment of the patient’s opioid requirements (with defined upper dose limits in the interests of safety), thus achieving therapeutic target levels more quickly than with standard OAT dosing according to current OUD treatment guidelines. We anticipate that opioid withdrawal and cravings will thus be more effectively managed, leading in turn to improved acceptability and retention on OAT.


Comments (0)