Case reports of NNHR have been described in five patients with positive test results for HSV or VZV in AH who had non-necrotizing retinitis consisting mainly of vasculitis, papillitis, or vitritis [2]. Other cases of non-necrotizing forms presenting as vasculitis and/or papillitis or panuveitis without retinal lesions were reported [3]. Albert et al. reported two cases of NNHR characterized by occlusive vasculitis with initial neovascularization. A herpetic etiology was confirmed by PCR analysis of ocular fluids: case 1 had a positive PCR for HSV1 on the AH while case 2 had a positive PCR for VZV on the vitreous sample [4]. Hazirolan et al. reported eight immunocompetent patients with NNHR. PCR analysis of vitreous samples confirmed the diagnosis: 63% of patients had HSV-1 DNA and 37% had VZV DNA [5]. Apart from NNHR, four cases of non-necrotizing herpetic vasculitis were also reported, and VZV was identified in the vitreous samples of two patients with PCR [6].
PCR was shown to be a powerful technique that allows detection of small quantities of DNA and RNA in ocular fluids. Various infectious agents can be detected with high specificity and sensitivity, including viruses. Results of PCR analysis of ocular fluids, being available within 24 to 48 h, have greatly improved the diagnosis of ocular viral infections, particularly those caused by human herpesviruses. AH analysis was contributory in 86.4% of patients with necrotizing viral retinopathies [3]. Bodaghi et al. found that the detection of HSV and/or VZV DNA by means of PCR in the AH was highly significant of recent productive infection in NNHR [2]. Our patient didn’t receive antiviral therapy before ACP. Indeed, antiviral drugs might decrease viral replication below the threshold of PCR sensitivity for viral detection [7]. A negative paracentesis could be repeated, especially in patients previously treated with antiviral therapy.
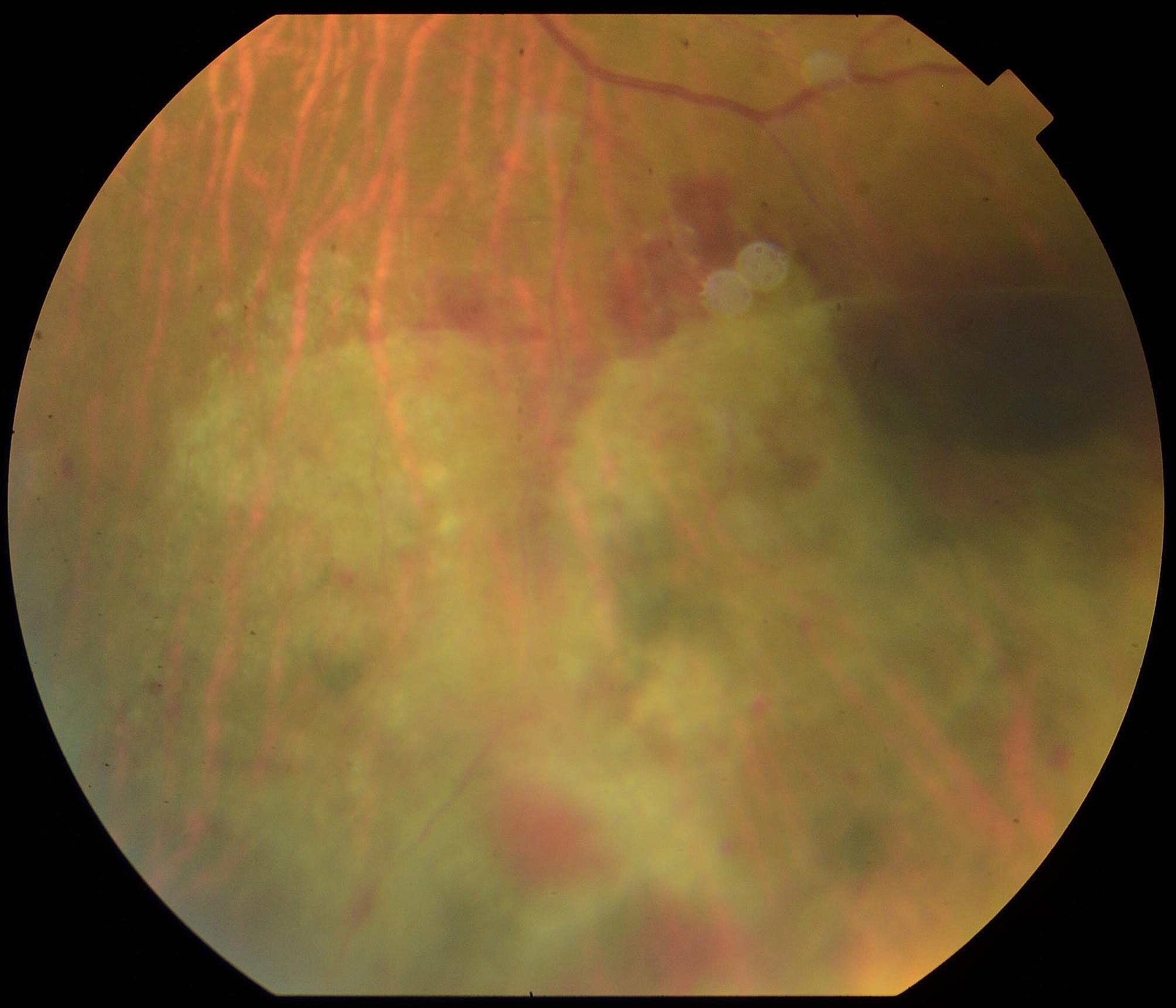
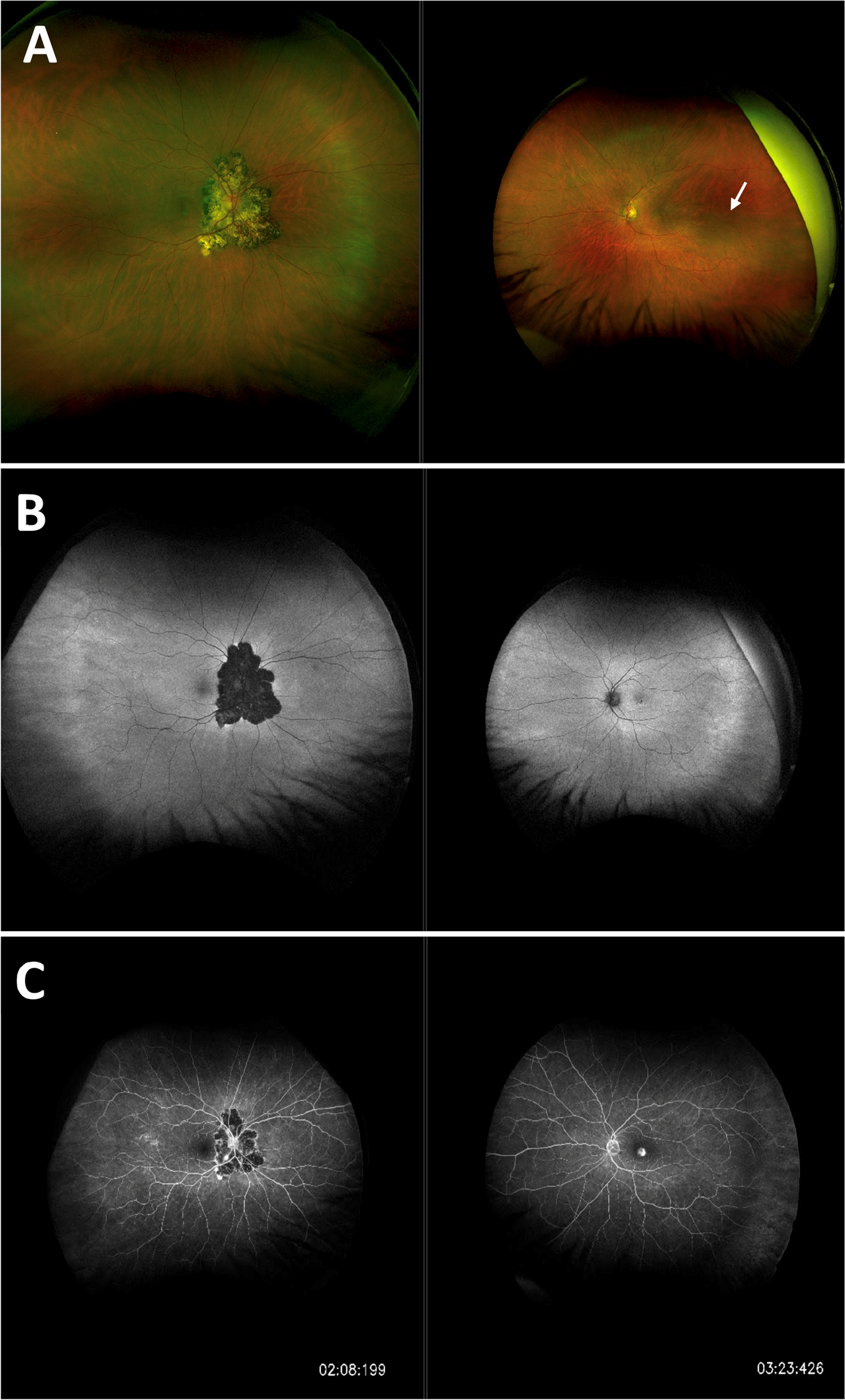
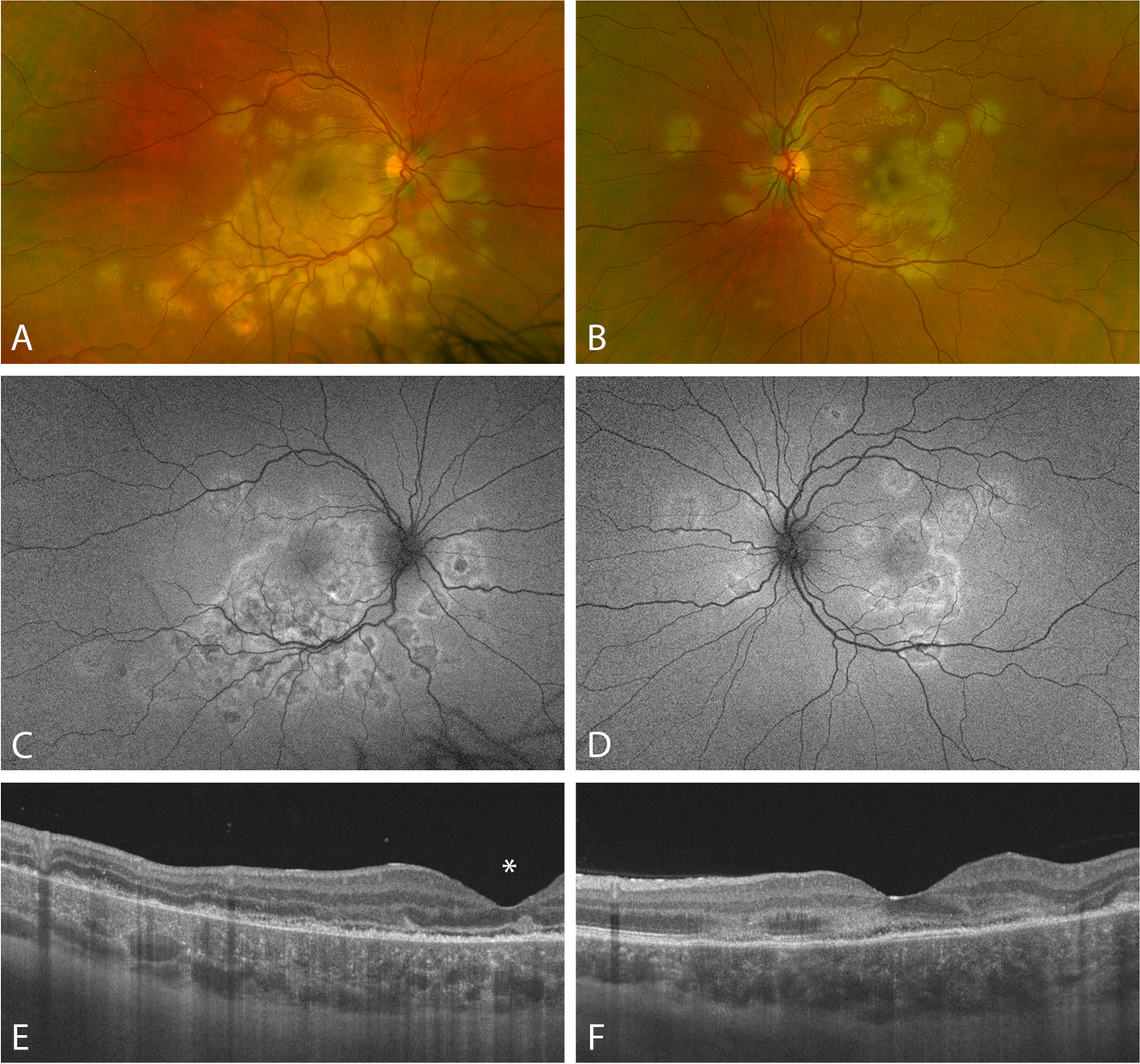
The viral retinitis described in our patient is different from most cases of atypical viral retinitis reported in the literature, but resembles the cases reported by Hazirolan et al., with retinal lesions that are smaller and focally situated at the posterior pole without progression with antiviral treatment [5].
The underlying reason for the variable clinical manifestations and severity of herpetic posterior uveitis is unknown but could be, in addition to pathogen-related factors, influenced by the variation in patients’ immune capacity. Bodaghi et al. hypothesized that necrotizing herpetic retinitis were due to an intracellular presence of the virus with subsequent cytopathic damage, whereas the NNHR were assumed to be associated with tissue damage based on immunological processes [2]. Wensing et al. suggested that NNHR occur in patients who have better functioning cellular immunity than patients with full-blown ARN [3].
Hazirolan et al. suggested that viral retinopathies might constitute a continuous spectrum of diseases, which clinical presentations depend on the patient’s immune status. Our patient, as well as theirs, with focal posterior non-necrotizing viral retinitis may be located at the starting point of the spectrum of herpetic retinopathies and constitute the mildest form of the disease [5]. However, more studies are required to test these hypotheses.
A remission was obtained in all cases after reaching the proper etiological diagnosis and initiating antiviral treatment. Oral acyclovir is mostly used for 6 weeks [8], but this period can be longer according to the disease response and the clinician practice [9]. Valacyclovir can also be used in the treatment of viral retinitis [10].
Albert et al. reported several recurrences after arrest of antiviral treatment, it was the first case of anterior uveitis recurrence after NNHR described in the literature [4]. Long-standing antiviral prophylaxis could be considered for such patients who present with recurrences of intraocular inflammation.
Future studies including a larger number of NNHR patients could reveal characteristics we were unable to identify here. The differential diagnosis of atypical viral retinitis is difficult clinically as it can mimic various other retinal conditions. In agreement with the previous studies, we propose viral analysis of ocular fluids in patients with retinitis, even in the absence of retinal necrosis, before initiation of immunomodulatory therapy and/or in those patients whose symptoms worsen while undergoing immunomodulatory treatments.



留言 (0)