
記住我


A 25-year-old healthy male presented to our clinic in 2018 with sudden painless loss of vision in the left eye (OS). The visual acuity (VA) was 20/300 at presentation. The patient had no history of recent systemic illness or vaccinations. Examination findings included normal anterior segment, clear vitreous, optic disc hyperemia, dilated and tortuous retinal veins along with retinal ischemic whitening of the cilioretinal artery territory (Fig. 1a). Fundus fluorescein angiography (FFA) revealed delayed venous filling and delayed emptying, and impaired filling of the cilioretinal artery, confirming the diagnosis of combined non-ischemic CRVO and CLRAO (Fig. 1b and c). Examination of the fellow eye was unremarkable (Fig. 1d), and remained unremarkable to the last follow-up. Systemic evaluation including blood pressure, fasting blood sugar, complete blood cell count (CBC), hemoglobin, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), urea, electrolytes, coagulation profile, cryoglobulins, antiphospholipid antibodies, factor V Leiden mutation, protein C and S levels, antithrombin III mutation, prothrombin mutation, homocysteine levels, serum protein electrophoresis, carotid ultrasound, and echocardiogram revealed no obvious abnormalities. His VA continued to improve, reaching 20/30 in four months. Five months following the initial presentation, he returned with a severe visual loss (20/400) in the left eye. He also had ciliary injection and an inflammatory anterior chamber reaction with a hypopyon of 0.2 mm height. Mild vitritis was also present accompanied by severe periphlebitis in a frosted branch pattern (Fig. 2a). A repeated FFA showed severe generalized retinal capillary non-perfusion sparing the macula (Fig. 2b and c). Spectral domain optical coherence tomography (SD-OCT) revealed a newly formed severe ME (Fig. 2d). Upon further detailed questioning, the patient recalled suffering from occasional oral ulcers. There was no history of genital ulcers, erythema nodosum of the skin, joint pain, neurological, nor gastrointestinal symptoms. The combined presence of oral and ocular lesions indicates a diagnosis of Behcet’s disease based on the international criteria for Behçet's disease [4].
Fig. 1
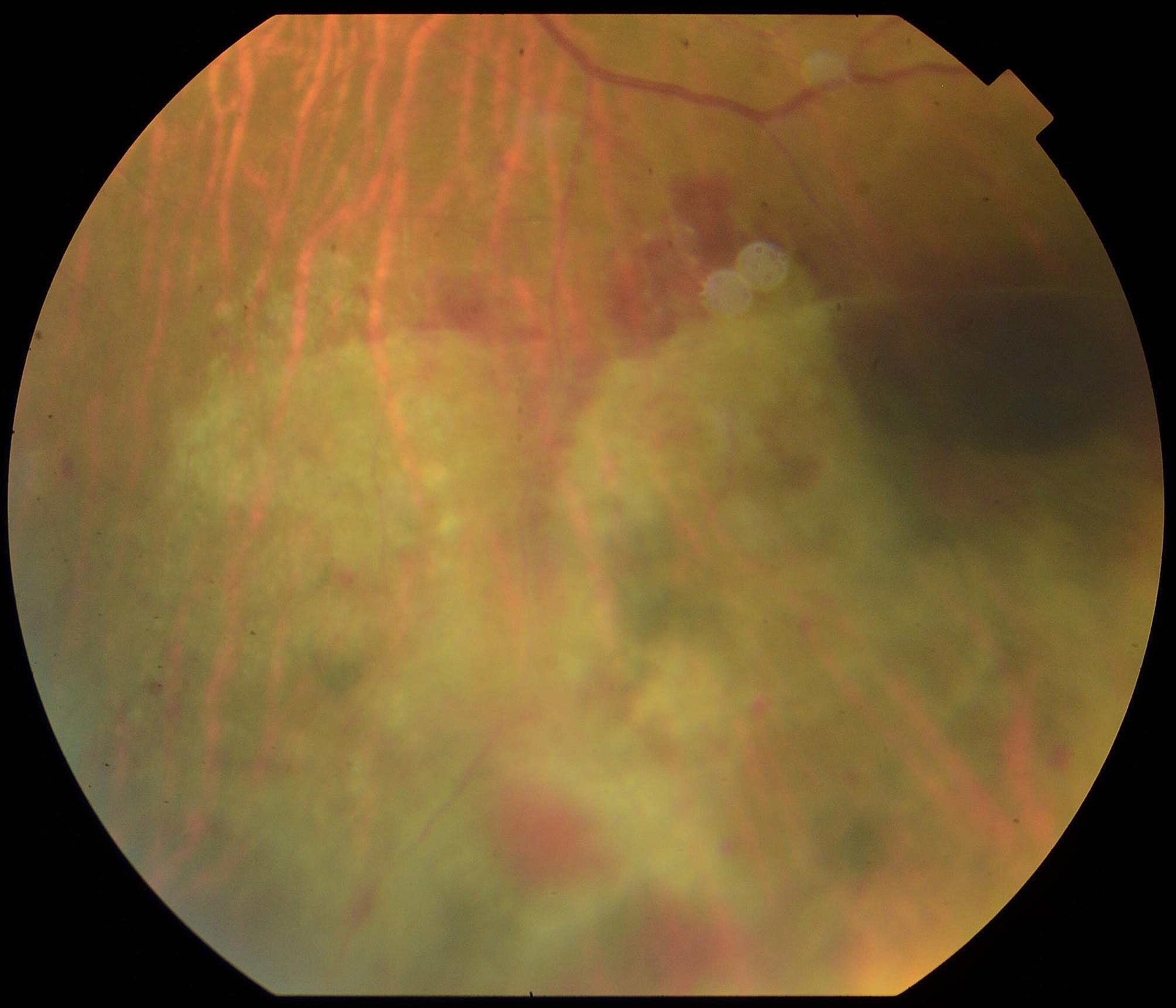
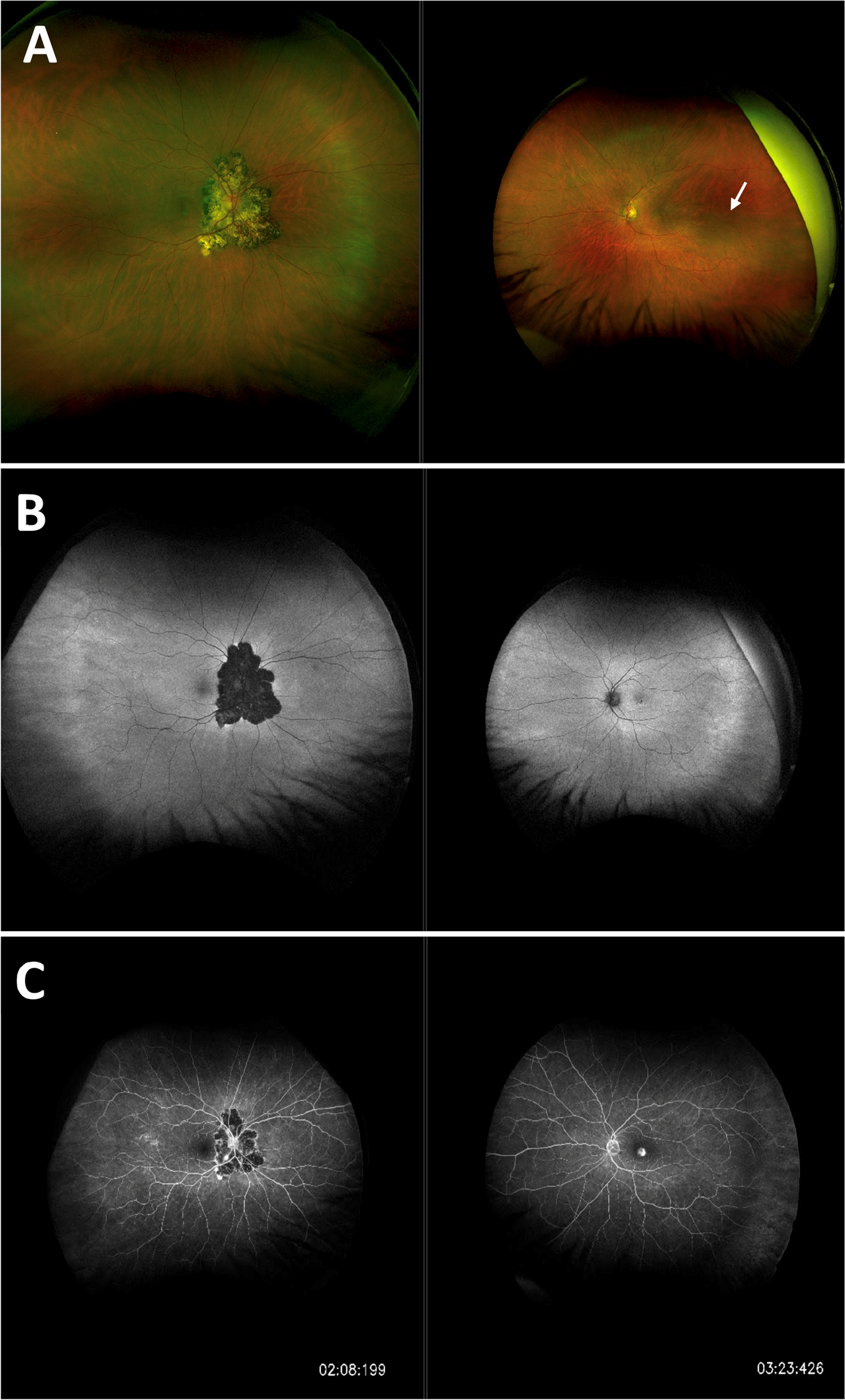
Imaging at initial presentation. a Color fundus photograph of the left eye showing dilated tortuous veins, swollen optic disc, and ischemic retinal whitening at the distribution of cilioretinal artery, Note: the two white areas above the superior retinal arcades represent a reflection artefact from the fundus camera. b A fluorescein angiogram showing disc leakage, with no abnormal vascular leakage or capillary non-perfusion (note: consecutive angiography frames revealed an obvious delay in the venous filling). c SD-OCT image showing inner retinal hyperreflectivity and thickening involving the nasal macula in the left eye. d Color fundus photo and fluorescin angiogram image of the normal right eye
Fig. 2
Imaging five months after the initial presentation. a The same eye shows increased disc edema with hyperemia, macular edema, and thick perivascular sheathing along the major vessels (predominantly venous), typical of frosted branch angiitis. b and c Early and late fluorescein angiograms revealed extensive retinal capillary non-perfusion and leakage from the optic nerve head and retinal veins. d SD-OCT shows severe macular edema
The patient was admitted to the hospital for further investigation and management. Full medical examination was unremarkable; there were no clinical signs of lymphoma, leukemia, sarcoidosis, tuberculosis, multiple sclerosis, systemic lupus erythematosus, or other autoimmune diseases. Laboratory tests were carried out, including CBC, renal and liver function tests, angiotensin converting enzyme level, CRP, ESR, serum protein electrophoresis, HLA-B51, autoimmune markers (anticardiolipin antibodies, anti-neutrophil cytoplasmic antibodies, antinuclear antibodies, antimitochondrial antibodies, rheumatoid factor, anti-double-stranded DNA, anti-single stranded DNA, anti-Scl-70 antibodies, and anti-Jo-1 antibodies), and serological tests for syphilis, viral hepatitis and HIV. ESR was high 34 mm/h (baseline ESR = 7 mm/h). Results of all other tests were within normal limits or negative. Chest computed tomography scan and doppler ultrasonography of carotid arteries were also normal.
Two days later, following a negative tuberculin skin test, a pulse therapy of intravenous methylprednisolone (1 g/day for 3 days) was initiated followed by a tapering regimen of oral prednisolone (1 mg/kg) and immunosuppressive therapy (Azathioprine 1 mg/kg, increased later to 2 mg/kg). One week later, there was a marked resolution of the perivascular sheathing and retinal hemorrhages. Two months later, all signs of inflammation had resolved with a slight improvement in ME. Treatment for ME was started with monthly intravitreal bevacizumab (1.25 mg/0.05 ml), which resulted in a good response after completing the loading regimen (three injections). Five months later, the ME resurged after a period of non-compliance to maintenance immunosuppressive medications. The ME eventually resolved after additional two injections of bevacizumab followed by two injections of aflibercept (Fig. 3a) with a resultant VA of 20/25. Twelve months from commencing immunosuppressive therapy, there were no signs of inflammation (Fig. 3b and c). Later, sector laser photocoagulation was applied to the ischemic retina when small tufts of retinal neovascularization were noted.
Fig. 3
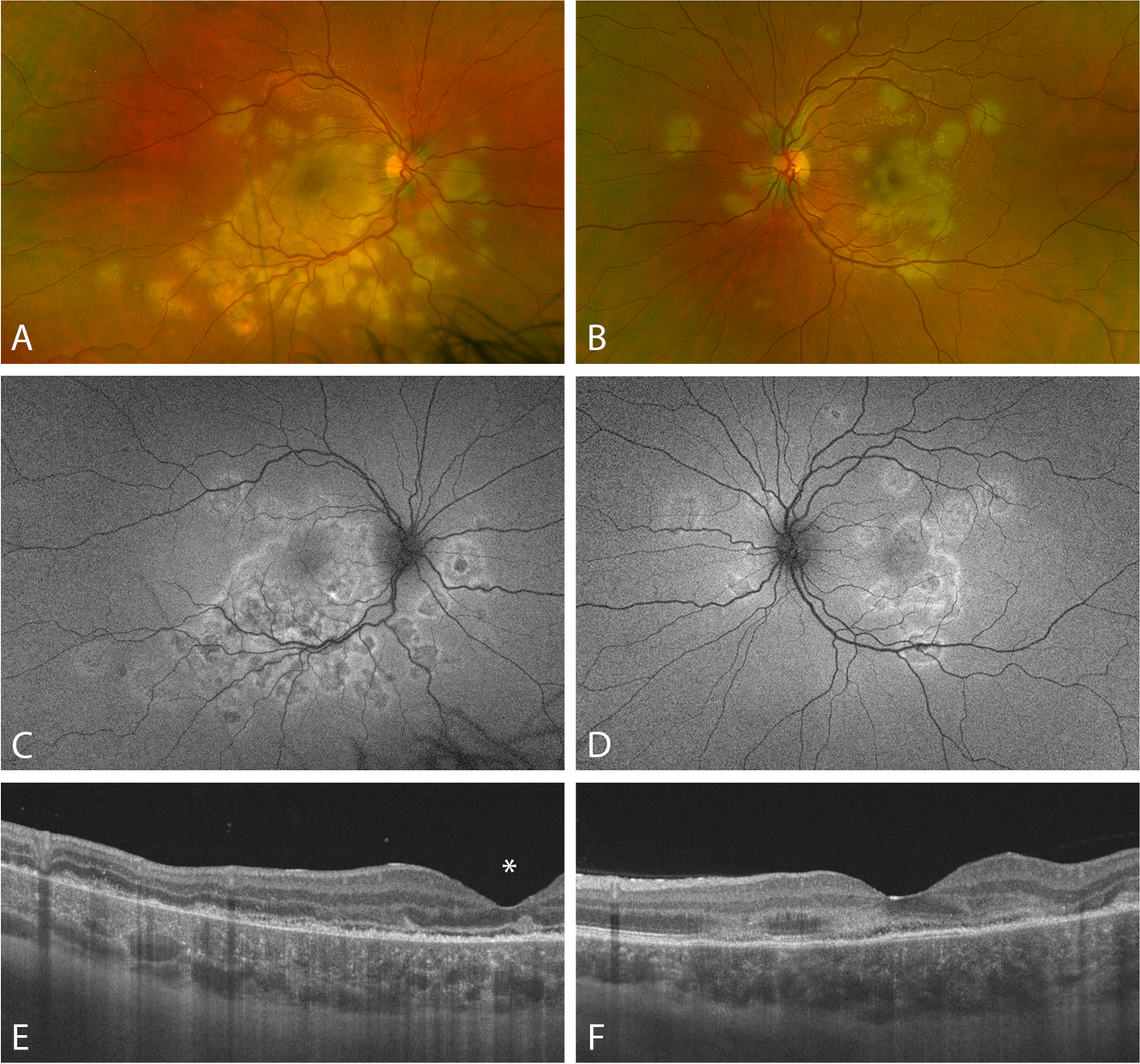
Imaging following treatment. a SD-OCT showed resolved macular edema following serial anti-VEGF injections and inner retinal atrophy from previous cilioretinal artery occlusion. At 12 months following immunosuppressive therapy, b fundus photo shows resolution of inflammatory signs, residual venous tortuosity and intraretinal hemorrhages and (c) late frame of fluorescein angiogram shows resolution of leakage from the optic nerve head and retinal veins and persistence of the retinal capillary non-perfusion
留言 (0)