1. IntroductionPortal vein tumor thrombosis (PVTT) is found in approximately 10–40% of all hepatocellular carcinoma (HCC) patients at the time of diagnosis [
1,
2], and the overall survival (OS) is only 2.7 to 4 months with the best supportive care [
3,
4,
5]. Two randomized placebo-controlled trials for sorafenib (the SHARP and Asia-Pacific trials) have shown that it significantly improves the median OS (10.7 vs. 7.9 months and 6.5 vs. 4.2 months, respectively) in patients with advanced HCC [
3,
6], with an actual survival benefit of less than 3 months in both Western and Asian populations and an effectiveness that is lower in populations with HCC related to the hepatitis B virus (HBV) [
7]. Atezolizumab and bevacizumab combination therapy has recently been recommended as the first-line therapy for advanced HCC [
8]. Subgroup analysis showed that this combination therapy was superior to sorafenib in HCC patients with main portal vein tumor thrombus. The median survival time was reported to be 7.6 and 5.5 months, respectively (p = 0.104) [
9].In a recent meta-analysis, hepatic artery infusion chemotherapy (HAIC) was found to be more effective in terms of objective response rates (ORR), progression free survival (PFS) and OS than sorafenib for advanced HCC patients [
10]. In the literature, the reported median PFS and OS of HCC patients with PVTT treated by HAIC ranged from 2–6 months and 7–10 months, respectively [
11,
12,
13,
14,
15,
16,
17,
18], with Song et al. reporting the poorest OS (7 months), as 60% of their patients (30/50) presented main portal vein invasion [
16]. The results of other studies recommend that HAIC be combined with other therapies, such as radiation therapy [
19] or sorafenib [
20]. However, objective comparisons of the effectiveness of different treatment regimens have heretofore been precluded by a number of factors, such as the fact that the enrolled patients in most studies were in marked heterogeneity, presenting either PVTT (including segmental (Vp2), lobar (Vp3) or main portal vein (Vp4) invasion) or major PVTT (Vp3 plus Vp4), and that results (such as a 1.54 hazard ratio of Vp3–4 to Vp0–2) were reported in the OS of advanced HCC patients after HAIC [
20]. Therefore, it is of significant clinical interest to report solely on Vp4 patients in a large patient series. Moreover, most studies excluded the patients with extrahepatic spread (EHS) for locoregional HAIC therapy; Lyu et al. reported [
21] no significant survival difference in HCC patients with or without EHS after HAIC, which accounted for 43% of patients at the initial diagnosis in their series.
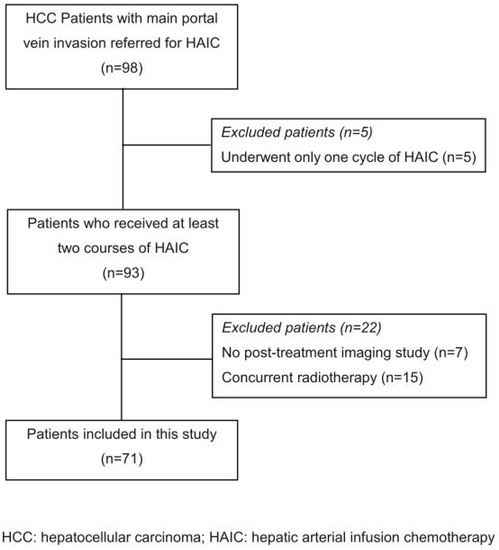
In the present retrospective study, we investigated the clinical outcomes of 71 Vp4 HCC patients who were treated by our “new” HAIC regimen, which combined a low dose of HAIC (24-hour infusion of cisplatin, mitomycin C, leucovorin and 5-FU for 5 consecutive days) followed by lipiodol injection, under the hypothesis that synergy between the separate chemo-cytotoxic and embolization effects could be achieved without significantly increasing liver toxicity. Patient subgroups with or without EHS or additional sorafenib target therapy were also analyzed and reported.
2. Materials and Methods
The data of consecutive eligible advanced HCC patients for the new regimen of HAIC in our hospital from January 2002 to December 2018 were retrospectively reviewed. HCC was diagnosed by either pathology or the elevation of α-fetal protein (AFP) levels above 400 ng/mL along with at least two different imaging modalities. The inclusion criteria were: (a) aged 18 to 85 years old; (b) advanced HCC with main portal vein invasion (Vp4); (c) Child–Pugh liver function class of A or B; (d) platelet counts ≥50,000/cumm; (e) prothrombin time INR ≤ 1.5; (f) white cell counts ≥2500/cumm; and (g) having received at least 2 courses of HAIC. Patients were excluded based on Eastern Cooperative Oncology Group (ECOG) performance statuses of 3 or 4, or patients who had received concurrent radiotherapy or if radiological follow-up images were unavailable. Patients with prior treatments or with EHS (regional LNs or distant metastasis) were not excluded in this study. The reason for not excluding patients with EHS was that the short-term cause of death in these patients was usually due to intrahepatic tumor rapid progress instead of extrahepatic lesions per se.
2.1. Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics review committee of Kaohsiung Veterans General Hospital.
The study was approved by the Kaohsiung Veterans General Hospital Institutional Review Board (IRB No. VGHKS22-CT7-03), which waived informed consent because this was a retrospective study without intervention or obtaining clinical specimens, and all of the data were analyzed anonymously.
2.2. New Hepatic Arterial Infusion Chemotherapy (HAIC)The left subclavian (axillary) artery was punctured under ultrasonographic guidance with the insertion of a 65 cm, 4-F catheter (RC1, Cordis, Johnson-Johnson, Roden, The Netherlands). The gastroduodenal artery (GDA) and/or right gastric artery were occluded by metallic coils to prevent gastroduodenal injury from the anticancer agents. Usually, the 4F catheter was used to embolize the GDA, and a microcatheter was used to embolize the RGA in some patients who revealed prominent RGA. For chemotherapy, the tip of the catheter was placed in the proper hepatic artery or replaced right hepatic artery under fluoroscopic guidance [
22]. No permanent delivery port system was used in this study. For HCC with dual hepatic artery blood supply, we did not embolize one of the dual supplying arteries for the purpose of flow diversion. Instead, we performed our HAIC regimen in each of the dual hepatic arteries separately with divided dose. For those with extrahepatic small collateral supplies, we performed superselective tumor embolization by injection of lipiodol and gelfoam pieces as the technique of routine TAE for HCC via the same arterial route.
Our hospital adopted a low-dose HAIC regimen from 1997 for the patients with advanced HCC, with a daily infusion of cisplatin (10 mg/m2), mitomycin-C (2 mg/m2) and Leucovorin (15 mg/m2) (dissolved in 50 mL isotonic sodium chloride solution) for 20–30 min, plus 100 mg/m2 of 5-fluorouracil (5-FU, dissolved in 250 mL of isotonic sodium chloride solution) administered for the remainder of the 24 h period using an infusion pump, for 5 consecutive days. Since January of 2002, we added partial embolization therapy by manual slow injection of 10 mL ethiodized oil (Lipiodol, Guerbet, France) into the hepatic artery after the 5 days of chemo-infusion (the “new” HAIC regimen). No gelfoam was injected to occlude the hepatic artery in this combination therapy.
Continuous heparin infusion of 5000 units daily (208 IU/hour) was given to prevent thrombus formation along the catheter surface. The angio-catheter was removed immediately after the injection of Lipiodol. The interval between the 2 courses of treatment was 6 weeks. Three-phase computed tomography (CT) or dynamic magnetic resonance imaging (MRI) of the liver was performed after every 2 courses of treatment, with an upper limit of 6–8 courses or until either radiological progress or death.
2.3. Sorafenib TherapyPatients in the combined HAIC and sorafenib group began sorafenib 400 mg BID either during or after the first HAIC session. Sorafenib doses were reduced, delayed, or temporarily interrupted if it was determined that there was clinically significant toxicity (grade 2 or higher, according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0) [
23]. Dose escalation or rechallenging with sorafenib was resumed when it was determined that toxicity had decreased and that the patient could tolerate the medication well. 2.4. Assessment of ResponseRadiologic response was determined according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST) guidelines [
24] and was defined as follows: complete response (CR)—no evidence of neoplastic disease; partial response (PR)—at least a 30% decrease in the sum of the diameters of “viable” (i.e., enhancement in the arterial phase) target lesions, taking as reference the baseline sum of the diameters of target lesions; stable disease (SD)—any cases that do not qualify for either partial response or progressive disease; and progressive disease (PD)—an increase of at least 20% in the sum of the diameters of viable target lesions, taking as reference the smallest sum of the diameters of viable target lesions recorded since treatment started.The PFS and OS periods were defined as the time elapsed between treatment initiation and tumor progression (as per the mRECIST guidelines) or death from any cause [
24], measured in increments of 0.5 months. As patients with metastatic lesions were not excluded in this study, we assessed the intra-hepatic PFS instead of the whole disease PFS. 2.5. Statistical Analysis
The data were expressed as mean ± standard deviation. Categorical variables were compared with the chi-squared test or Fisher’s exact test when appropriate, and continuous variables were compared with the Mann–Whitney test. The median PFS, OS and associated 95% confidence intervals (CI) were analyzed using the Kaplan–Meier curve, and the difference was determined by the log-rank test. Univariate and multivariate analyses of age, sex, tumor size, Child–Pugh classification, AFP level, treatment courses and additional sorafenib treatment were performed using Cox’s regression model with proportional hazards. The therapeutic outcomes in patients with or without additional sorafenib therapy were also compared and analyzed. A p-value of less than 0.05 was considered statistically significant. Statistical analysis was performed using the Statistical Product and Service Solutions (SPSS) version 18.0 software (SPSS Inc., Chicago, IL, USA).
4. DiscussionPortal vein tumor thrombosis (PVTT) occurs in 35–50% of HCC patients and involves the main trunk at the time of diagnosis in 15–30% of cases [
1,
2]. Although the HCC treatment guidelines that are endorsed by the American Association for the Study of Liver Diseases [
26] (AASLD) and European Association for the Study of the Liver [
27] (EASL) recommend sorafenib therapy as the sole treatment for advanced HCC, the clinical benefit of sorafenib by itself has been shown to be marginal [
6,
28]. Two randomized clinical trials reported the use of sorafenib prolonged the median overall survival relative to placebo control in patients with macroscopic vascular invasion from 4.9 months to 8.1 months (subanalysis of the SHARP trial) [
28] and from 4.2 months to 6.5 months (the Asia-Pacific trial) [
6]. However, the efficacy of sorafenib has been shown to be lower in areas where HBV shows predominance, such as in Asia (70%) [
7], a finding that was confirmed by the GIDEON (Global Investigation of Therapeutic Decisions in Hepatocellular Carcinoma and of Its Treatment with Sorafenib) study, suggesting that worsened prognosis factors have become more common in Asian populations [
29]. In recent years, there have been remarkable advances in systemic treatments for HCC. Cheng et al. reported a promising clinical outcome for a combination therapy of atezolizumab and bevacizumab, with a better overall survival (19.2 months) than that of sorafenib alone (13.4 months) in Child A, unresectable HCC patients [
30]. It is worth noting that 61.6% and 57.0% patients in each of their groups had no macrovascular invasion at study entry. Since vascular invasion in the advanced HCC patients is a prognostic risk of OS, and the OS of sorafenib in a prior Asian randomized controlled trial study [
6] was only 6.5 months (compared with the OS of 13.4 months of the afore-mentioned study [
30]), we speculated that the patient status of enrollment may be not the same in the two studies, as the definition of unresectable HCC may cover a wide variety of the disease status. This phenomenon again emphasizes the importance of clearly stratifying HCC status, as we did with the Vp4 patients in our present study. In addition, this high medical cost of combination regimen may limit its extensive application in advanced HCC. Searching for alternative-yet-effective therapies for the macrovascular-invaded HCC patients is therefore warranted.With refinements in surgical techniques, patient selection and perioperative management, resection for HCC with tumor thrombosis extending to the major portal vein is now possible. Chok et al. reported median OS of 8.58 months in patients with PVTT extending to or beyond the portal vein bifurcation treated by partial hepatectomy with thrombectomy [
31]. In a review article, Nevarez et al. concluded that partial hepatectomy with en bloc resection of PVTT in second-order and distal portal branches could offer significant benefits in terms of outcome measures in carefully selected patients by experienced centers, particularly in the sequelae of portal hypertension [
32]. Lee et al. also reported that PVTT extending to the main portal vein was a significant risk factor for recurrence and worse OS (p
33]. Given the development of effective systemic and locoregional therapy options, surgical resection in HCC patients with advanced PVTT should be cautioned against [
32].Im et al. conducted a nation-wide, multicenter study of radiotherapy (RT) for HCC patients with major PVTT and reported that the median OS of RT alone versus combined with other treatments were 8.7 months and 10.4 months, respectively (p = 0.023) [
19]. Katamura et al. reported a matched case-control study of a combination therapy of HAIC with three-dimensional conformal RT to treat HCC patients with major PVTT. Although the ORR was significantly higher for the RT group (75% vs. 25%, p = 0.012), there were no significant differences between the median OS (7.5 vs. 7.9 months) [
34]. Yttrium-90 radioembolization particles, especially of the glass microspheres, has a very small particle size (30 mm), allowing for deep infiltration into the tumor without ischemia of the hepatic parenchyma [
35]. The absence of overt arterial embolization effect is important for patients who have already had their portal venous occlusion due to malignant tumor invasion, as complete loss of blood supply from both the hepatic arterial and portal venous flow may result in very unfavorable clinical outcomes. Yttrium—90 Transarterial Radioembolization (TARE) was reported to be superior to sorafenib in prolonging survival of PVTT HCC patients in some retrospective studies [
33,
34,
35,
36,
37,
38,
39]. Abouchaleh et al. reported that 77 Vp4 patients receiving TARE had a median OS of 7.7 months in Child–Pugh A or B7 patients and 3.4 months for ≥B8 [
40]. Two Phase III trials—Sorafenib versus Radioembolization in Advanced Hepatocellular carcinoma (SARAH) [
41] and Selective Internal Radiation Therapy Versus Sorafeni (SIRveNIB) [
42]—failed to demonstrate any significant superiority of TARE compared with sorafenib. In the SARAH study, the presence of PVTT seemed to favor sorafenib in term of OS.In Japan and South Korea, HAIC is recommended instead of sorafenib as the first-line treatment option for advanced patients with PVTT [
43]. A recent meta-analysis showed that HAIC was more beneficial than sorafenib for advanced HCC patients in terms of ORR, PFS and OS [
9]. The reported tumor ORR and median OS ranged from 28% to 48% and 5.7 to 10.5 months, based on the enrolled patient characteristics, with either cisplatin-based [
15,
16,
17] or oxaliplatin-based regimens [
20]. Jeong [
13], Song [
44] and Ahn [
45] compared the therapeutic efficacy of HAIC alone and with sorafenib in treating advanced HCC (including Child–Pugh A and B patients) and found that patient survival could be significantly increased from 4.9–6.4 months to 7.1–10.0 months, respectively. Nagai et al., in a small series study (34 patients), reported that HAIC plus sorafenib treatment had more clinical benefit for PVTT patients than HAIC alone in Child–Pugh A patients (315 vs. 197 days) but not in Child–Pugh class B patients (234 vs. 228 days) [
46]. Liang further confirmed this conclusion in a large series of 225 patients, with a better OS of 12.9 months in the HAIC plus sorafenib group versus 10.5 months in the HAIC alone group, with a hazard ratio of 1.54 of Vp3–4 vs. Vp0–2 (p = 0.007) [
20]. In the present study, the median OSs of our 71 Vp4 HCC patients and 56 Child–Pugh A liver function patients were 13 and 14 months, respectively, which were superior to those of the RT, TARE, HAIC alone and HAIC plus RT or sorafenib combination therapy patients in other studies.
Table 4 compares the therapeutic outcomes of previously reported multidisciplinary treatment of advanced liver cancer with portal vein tumor thrombus.Iwamoto et al. reported a multicenter study of a new FP HAIC regimen (cisplatin suspended in lipiodol combined with 5-fluorouracil) to treat advanced HCC [
47]. After propensity score matching, the new-FP HAIC regimen revealed a better median OS than that of sorafenib (12 vs. 7.9 months, p
48]. In proposing our new HAIC regimen, we hypothesized that although varying degrees of cellular damage will inevitably ensue after continuous chemoinfusion, injured cancer cells can recover during the interval time between treatment courses or cycles. Therefore, an additional embolic effect by injecting lipiodol may help induce cellular death by some synergistic mechanism. Moreover, because of the high affinity of lipiodol for tumors, most of the injected 10 mL lipiodol will aggregate and be retained in the HCC mass, leaving the normal liver parenchyma less damaged. As the major portal veins were already occluded in these advanced HCC patients, we did not inject gelfoam pieces for embolization in order to preserve hepatic artery patency. The former hypothesis was confirmed by the clinical fact that the ORR increased from 20% of our prior sole low-dose HAIC study [
22] to 64.8% with a median OS of 13 months in our Vp4 patients.Although HCC patients with EHS are usually considered not candidates for locoregional therapy, Lyu et al. reported their experience of HAIC in 116 patients with 43% (50 patients) presenting with EHS21. Their results reveal a trend of better median OS in patients without EHS than those with EHS (14.8 vs. 9.8 months) but without reaching significance (p = 0.068). In Iwamoto’s series [
47], HAIC therapy did not have less OS in patients with MVI and EHS as compared with sorafenib therapy (7 and 5 months, respectively, p = 0.28). In the present series, 20 of the 71 (28.2%) Vp4 patients presented with EHS. Our results also reveal no significant survival difference between these two group with or without EHS (12 vs. 13 months, p = 0.434). The median OS of the patients with EHS after HAIC was superior to those of supportive care (2.7–4 months) [
3,
4,
5] or target/immunotherapy (5.5–7.6 months) [
9]. These findings might suggest that EHS should not be an absolute contraindication of HAIC in treating advanced HCC patients.In the present study, we failed to demonstrate the clinical benefits of additional sorafenib use. One possible explanation is that the synergistic effect by adding the lipiodol embolization far outweighs the stabilization effect of sorafenib. Another possible explanation may be that the with sorafenib patient group had higher percentages of high AFP (≥400 ng/mL) levels, although not reaching statistical significance, which have been shown to be an adverse prognostic factor for mortality in patients with advanced HCC [
20], although not in our series of the 71 Vp4 patients. The above factors may have influenced the OS of the sorafenib-plus group in our patients. Additional prospective comparative studies are warranted to draw a definitive conclusion on this issue.

Comments (0)