1. IntroductionGastric cancer (GC) grows complex, like an incurable wound, leading to a systemic inflammatory immune response, which plays a major role in the progression of GC. Previous study has revealed that increased interaction between systemic inflammatory responses is correlated with poor outcomes in cancer patients [
1]. Presently, the main comprehensive treatment of GCs is based on surgery, but surgery generates a mighty blow to the body, followed by causing a corresponding inflammatory response and stimulating the immune system to cause a metabolic stress response. Furthermore, relevant research indicated that poor nutritional status always led to poor prognosis of patients after critical surgery [
2]. Furthermore, some studies have indicated that perioperative nutritional support may affect the long-term prognosis of cancer patients [
3,
4]. Thus, preoperative inflammation and nutritional status are very important to evaluate the therapeutic effect.A variety of indicators have been used in GC as clinical predict prognostics such as preoperative neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), prognostic nutrition index (PNI), albumin to globulin ratio (AGR), tumor-node-metastasis (TNM) stage, and so on [
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15]. However, previous study has shown that the TNM stage is not particularly sensitive for the prognosis of GC [
7], which means that it is not enough to predict patient outcomes based on TNM classification alone. Moreover, due to the heterogeneity of the tumor, even patients with the same TNM stage or with the same treatment strategy may have different outcomes [
16,
17]. Some studies have indicated that high preoperative NLR and PLR are associated with a poor prognosis and high PLR is associated with progressive GC metastasis [
5,
18]. Lee et al. supposed that preoperative NLR and PLR were independent prognostic factors for overall survival (OS) in advanced GC [
19]. Several studies have revealed that AGR and PNI are prognostic factors for various cancers including colorectal cancer, small-cell lung cancer, renal cell cancer, and glioblastoma [
20,
21,
22,
23]. PNI was also recognized as a valuable prognostic predictor for cancers of the digestive system [
13,
24]. A few studies have reported that low AGR is an independent prognostic factor for the assessment of cancers [
25,
26]. Recently, it has been shown that the nomogram, which is a simple graphical visualization combining and quantifying all independent prognostic factors, plays an increasingly vital role in medical sciences and clinical studies [
27]. Although there are some prognostic nomograms available for gastric cancer [
28,
29,
30], only a few of them considered the patient’s inflammatory and nutritional factors, which are simple and effective risk factors. Therefore, in order to predict the prognosis of GC accurately, we incorporated the clinicopathologic features and preoperative inflammatory and nutritional factors to propose a nomogram and perform tests to validate whether this model could predict the prognosis more accurately compared with traditional TNM staging systems. 2. Material and Methods 2.1. Patient PopulationA retrospective study was performed in 522 patients with histologically diagnosed GC from 2014 to 2019 at the Fujian Provincial Hospital (Fuzhou, Fujian, China). Among them, 389 GC patients treated at the Department of Surgical Oncology between February 2014 and April 2019 formed the primary cohort, and 133 GC patients treated at the Department of Gastrointestinal Surgery between October 2014 and March 2017 formed the validation cohort. The inclusion criteria were as follows: (1) Patients who were diagnosed with GC histologically; (2) did not received any treatment preoperatively; (3) distal radical gastrectomy for GC (R0 resection + D2 lymph node dissection) [
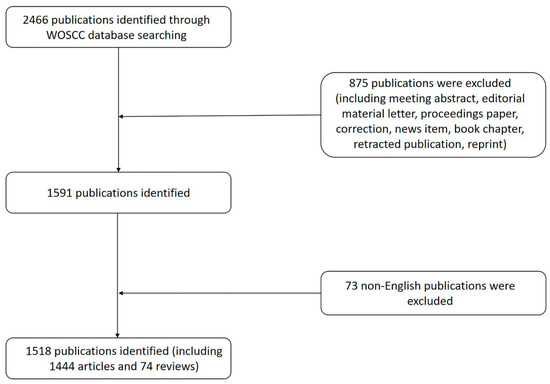
27]. The exclusion criteria were as follows: (1) Dependence on enteral nutrition (EN), parenteral nutrition (PN) or presence of acute inflammation (elevated serum C-reaction protein or procalcitonin) for 2 weeks; (2) patients diagnosed with a second tumor or an indefinite disease; (3) patients who received palliative resections; and (4) patients without complete clinical data. Written informed consent for participation or publication was provided by all patients. This study was reviewed and approved by the Ethics Committee of Fujian Provincial Hospital. All study procedures were performed in accordance with the 1964 Declaration of Helsinki and later versions. 2.2. Data Collection
The clinical characteristics included age, gender, tumor size, Borrmann type, TNM stage, pathological type, histological grade, and OS status. The levels of preoperative inflammatory factors were collected. The results of preoperative blood tests including the serum albumin level and serum globulin level, neutrophil, lymphocyte, and platelet blood cell count was obtained within 1 week before surgery. NLR is the neutrophil count (N)/lymphocyte count (L). PLR is the platelet count (PLT)/lymphocyte count (L). PNI is the Onodera Prognostic Nutrition Index (PNI), PNI = 5*Lymphocyte count (L × 109/L) + serum albumin (ALB g/L). AGR is serum albumin (ALB g/L)/serum globulin (GLB g/L).
2.3. Follow-Up
After completion of primary treatment, all patients with GC were followed up periodically according to the clinical guidelines. During the first 2 years, the patients were followed up every 3 months. Patients with no recurrence during the next 3–5 years were generally followed up every 6 months and annually thereafter. Patients who did not attend our hospital on time were followed-up by telephone to obtain the information about their treatment and survival status. The duration of the follow-up in our study was measured as the overall survival (OS), taking into account the time from GC diagnosis to last follow-up or death.
2.4. Statistical Analysis
Statistical analyses were performed using SPSS 26.0 (IBM, Chicago, IL, USA) and R for Windows (version 4.2.0). The propensity score was calculated based on age, gender, tumor size, tumor stage, node stage, metastasis stage, clinical stage, Borrmann type, pathological type, histological grade, OS status, NLR, PLR, PNI, and AGR. Patients in the primary cohort were matched 1:1 using nearest neighbor matching, based on the closest propensity score to those in the validation cohort. X-tile statistical software (version 3.6.1) was used to evaluate the optimal cutoff points of this study, and continuous variables were converted into categorical variables, which were classified according to the clinical results. We used univariate and multivariate regression analyses to analyze the risk factors in the primary cohort. A nomogram was established based on the results of multivariate analysis by the rms package. Discrimination and calibration tests were used to validate the accuracy of the nomogram in the primary as well as external validation cohorts. We used Harrell’s concordance index (C-index) to measure the discrimination of the nomogram. The value of the C-index ranged from 0.5 to 1.0, where 0.5 indicates random chance, while 1.0 means that the model was fully capable of predicting the outcome correctly. The calibration curve of the nomogram for predicting the OS was drawn. Then, we calculated the total points of each patient based on the established nomogram model, and used the X-tile program to delineate two groups of patients with different prognostic risks based on the total points. The Kaplan–Meier method and log-rank test were used to compare the survival curves of the dichotomous risk groups. All statistical tests were two-sided, and p < 0.05 indicates a statistically significant difference.
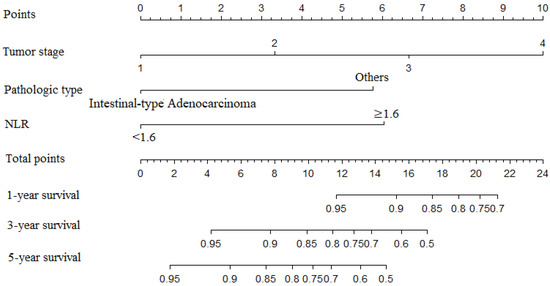
4. DiscussionAccurate prediction of the prognosis of cancer patients is of great significance to determine the definitive treatment or management plan [
31,
32]. Although most of us used traditional TNM staging systems to predict the prognosis of GC patients clinically, several studies have recently supposed that some drawbacks may exist when predicting the prognosis of GC patients only according to the TNM classification [
17,
18]. Previous studies have indicated that preoperative immunological and nutritional conditions are associated with both the postoperative and long-term outcomes of malignant tumors [
33,
34,
35,
36]. In our study, we found that NLR, PNI, and AGR were associated with the OS of GC patients in univariate analysis, but only NLR was an independent prognostic factor in multivariate analysis, together with tumor stage and pathological type. As we know, a nomogram can be established according to a Cox regression model, which is considered as a prediction model in clinic. The nomogram consists of coordinate axes and a scoring system. Each axis represents an independent survival predictor, and the corresponding score on the axis represents the impact of the predictor. As a result, we can see a perceptible visualization of the survival of a specific disease easily by nomogram. Thus, we established a nomogram according to the weights of these factors in the model, which was simple and effective to evaluate. All factors included in the model are easily available in clinical practice, and the internal validation showed consistent and stable predictive power, making it a practical tool for clinical reference.According to our results, this model performed well in predicting the OS of GC patients, with a C-index of 0.753 in the primary cohort and 0.748 in the validation cohort. Moreover, our model predicted the OS of GC patients more accurately than the TNM stage (0.689 in primary cohort and 0.727 in validation cohort). Furthermore, we found that the nomogram prediction and actual observation were fairly close according to the calibration curves. The TNM stage only reflects the depth of tumor invasion, lymph node metastasis, and whether there is distant metastasis. Mao YP et al. observed that patients with the same TNM stage may have different clinical outcomes; conversely, patients with the same clinical outcome can be classified into different TNM stages [
17]. Therefore, the traditional TNM staging system sometimes fails to accurately predict the OS of GC patients, and the model in this study can remedy this deficiency.Actually, previous studies have developed several other nomograms to predict the individual survival of patients with gastric cancer. However, there have been some shortcomings. In a study published in 2021, the model was validated internally using the bootstrap method, lacking external validation in an independent cohort from a different institution [
29]. Another study developed and validated a nomogram for GC patients using a multicenter database in Korea [
30], however, it mainly focused on the clinical features and pathological results. Furthermore, this study only included patients who underwent open gastrectomy. It is worth noting that although a study published in 2022 was to use a web-based nomogram so that any expert could calculate the overall survival probability and had a long-term follow-up period, it did not include some clinical and pathological characteristics into the model [
28]. In contrast, we incorporated clinicopathologic features and preoperative inflammatory factors to propose a nomogram, which could predict the prognosis of gastric cancer patients after distal radical gastrectomy. The results of our study indicated that patients with GC had different prognosis of OS by varying perioperative inflammatory and nutritional status (
Table 2). Furthermore, due to combining the clinical inflammatory factors, the pathological type of GC, and traditional TNM stage, our method took into account the anatomical and individual patient differences to predict the 1-, 3-, and 5-year OS of GC patients more accurately. It is worth noting that the differences between the groups predicted by this nomogram for different prognoses were significant in the primary cohort and the validation cohort (
Table 4), which means that this model performed well in predicting the overall survival. Thus, we supposed that patients with a high number of total points according to this model were classified as high risk and should be given active therapy and special attention.Several studies have reported that chronic inflammation is closely associated with GC invasion and metastasis [
37,
38]. Inflammatory cells such as neutrophils, lymphocytes, and platelets continue to produce a range of cytokines and chemokines, which promote tumor growth, invasion, and metastasis when the tumor microenvironment is forming [
39]. Tumor growth could easily lead to impaired nutrient absorption and a broken immuno-nutritional status, which would lead to a persistent chronic inflammatory response and promote tumor growth. The inflammation caused by surgery corresponds to the degree of surgical trauma, leading to metabolic stress in the body. In order to heal the trauma caused by surgery, the body needs to carry out metabolism, so that the body can use protein and muscle to restore the normal nutritional state of the body in a short period of time. There is increasing evidence that the prognosis of tumor patients is closely related to their nutritional status [
34,
35,
36]. However, it is still unknown as to why preoperative malnutrition leads to poor postoperative outcome. Previous study has suggested that malnutrition impaired immune function, which led to an increased risk of postoperative infection and tumor metastasis [
40]. Some studies have considered that malnutrition is a chronic or subacute state. Although the degree of its inflammatory response is different, it could lead to changes in components of the human body and the decline in immune function [
41,
42]. Meanwhile, malnutrition could activate the systemic inflammatory response and influence host immunity [
14]. In terms of the systemic inflammatory and nutritional factors, our univariate analysis showed that NLR, PNI, and AGR were associated with the prognosis of GC patients, but only NLR was an independent prognostic factor after multivariate analysis. Previous studies considered NLR as a highly reproducible, cost-effective, and widely available prognostic marker for GC patients [
43,
44,
45]. Relevant research has also indicated that the preoperative NLR correlated with not only the long-term outcomes, but also the perioperative outcomes of GC patients [
46].The mechanisms by which systemic inflammatory responses are associated with tumor progression have been extensively discussed. One reason for this correlation is that in patients with high NLR, tumor growth may be supported by neutrophil-derived cytokines such as vascular endothelial growth factor, interleukin-18, and matrix metalloproteinases [
46]. Additionally, the increased number of neutrophils around the tumor may suppress the anti-tumor immune responses of natural killer cells and activated T cells [
46]. At the same time, the decrease in the number of lymphocytes may weaken the lymphocyte-mediated antitumor cellular immune response. Therefore, it may be that neutrophilia and lymphopenia work together to increase NLR, thereby promoting angiogenesis, suppressing antitumor responses, and ultimately promoting tumor growth and progression [
43,
44,
45].
Despite several advantages of our model, there were still some limitations to the current study. First, this study was a retrospective analysis, and there may have been sample selection bias in our study. Second, both cohorts in this study were from the same medical center, and the sample sizes of the two cohorts were not large enough. Thus, for this model to be valid, more data from other institutions in other regions will be needed in the future.

Comments (0)