1. IntroductionThe instability of the patellofemoral joint has gained great attention from clinicians and researchers alike, as new revelations in biomechanics and treatment options surface. We often distinguish traumatic dislocation of the patella from habitual dislocation. For a traumatic dislocation to occur, there has to have been an adequate traumatic event, such as a direct medial impact to the patella. Habitual dislocations of the patella arise during the physiological motion of the knee joint and commonly occur repeatedly. This is due to inherent joint instability or secondary joint instability acquired through not sufficiently treated post-traumatic injuries. The patellofemoral joint is guided and correctly aligned by the interaction of active, passive, and static stabilizers. In the complete extension of the knee joint, the medial ligamentary complex acts as a passive stabilizer. At around 30° knee flexion, the patella seats itself in the trochlear groove and is supported, statically, by the osseous structures. During higher degrees of flexion, the quadriceps muscles act as active stabilizers. Anatomical abnormalities categorized as predispositions are those that promote a deviation from the optimum force vectors, thereby resulting in a lateralization of the patella or incongruence of the patella and trochlea. Known predisposing factors are valgus deformity, increased internal rotation of the femur, increased external rotation of the tibia, elevated TTTG-distance (tibial-tuberosity to trochlear groove distance), high-riding patella, or dysplasia of the trochlea or patella itself. Muscular hypotrophy and laxity of the ligamentary complex can also act as a predisposing factor. The evaluation of predisposing factors helps us to identify patients at risk for dislocation events as well as derive definitive treatment options in order to prevent the development of recurring dislocations and subsequent joint damage [
1,
2,
3,
4,
5,
6,
7,
8,
9,
10].Patients who exhibit a high degree of predisposing factors have been shown to often suffer their first dislocation event as young adolescents [
6,
9,
11]. However, the presence of a predisposition does not lead to a dislocation in every case. Depending on the severity of the predisposition, it can be difficult to distinguish whether the cause of a dislocation event is of traumatic nature or can be attributed to a predisposition. Therefore, the mechanism of trauma should be included in the process of patient assessment. A certain treatment regimen is then chosen based on the resulting injuries incurred by the dislocation event and the underlying risk factors for a dislocation to reoccur.In the event of a first-time dislocation and lack of traumatic structural damage (e.g., flake fracture), non-surgical treatment options are usually chosen [
6,
12,
13,
14,
15]. Surgical treatment is often indicated in the case of recurring dislocations of the patella after a thorough workup of predisposing factors has been performed. If the mechanism of trauma is inadequate and a relevant predisposition is present, surgical therapy should be considered even after a first-time dislocation event [
6,
14,
16,
17]. 3. Methods
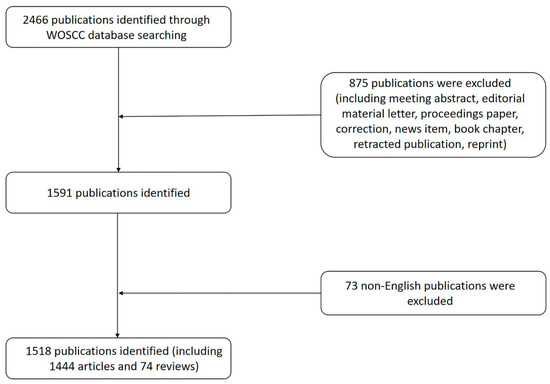
We included all patients who were treated in our clinic from January 2000 until April 2020 that were recorded with a diagnosis of “dislocation of the patella” on the standard form F1000 of the German statutory accident insurance. The cases that were not dislocations, after all, were excluded.
For data acquisition purposes we also utilized available digital imaging (X-ray, MRI, torsional-CT scans), as well as treatment documentation (out-patient documentation, discharge papers, surgical protocol).
Patients were grouped according to age with a cut-off at 18 years (smaller or equal to 18 and older than 18 years).
We evaluated general descriptive demographical aspects (age at trauma, gender), general information concerning the accident (mechanism of trauma, date of the traumatic event), and information concerning treatment (in-patient, total time of hospital stay, type of therapy, surgical technique chosen, time passed between trauma and surgical treatment). The data were obtained from the available form F1000 or the treatment documentation. For ease of systematical evaluation, we grouped the circumstances of the accidents in the subgroups direct impact, insufficient trauma, fall, rotational trauma, and unknown mechanism of trauma.
Furthermore, we evaluated anatomical aspects. The affected side, first-time dislocation or recurring, frontal axis, femoral and tibial torsion, TTTG value, height of the patella, shape of the trochlea according to Dejour [
18], and lateral trochlear inclination angle. Frontal axis measurements were performed on full-length standing AP radiographs, and torsional angles were measured in CT scans according to the method of Waidelich [
19]. Patella height was determined via the Insall-Salvati-Index [
20] and Caton-Dechamps-Index [
21]. Taking into consideration both methods of measurement, the cases were categorized as normal, normal to high-riding, normal to low-lying, high-riding, and low-lying. The shape of the trochlea was either classified as “normal” or categorized according to the Dejour subtypes A-D [
18] by means of axial MRI scans. Additionally, we measured the lateral trochlear inclination, i.e., the resulting angle by drawing a tangent line along the lateral trochlear facet and the posterior condylar tangential line, also by means of axial MRI scans.To analyze the relevance of predisposing factors, we determined the proportion of “knee-healthy” patients in each category with respect to the mechanism of trauma. Those labeled as “knee-healthy” exhibited measurement values that lie outside of the range of those patients who, in our clinic, are advised to undergo surgical treatment after having suffered a dislocated patella. Subjects were ruled out from the “knee-healthy” category if they exhibited a valgus deformity of greater or equal to 4 degrees, a femoral torsion of less or equal to -34 degrees, a tibial torsion of greater than or equal to 45 degrees, trochlear dysplasia Type D according to Dejour [
18], a TTTG value of greater or equal to 16 mm or a high-riding patella. We excluded those subjects from our study group whose frontal axis, torsional values, and TTTG value could not be determined.
The descriptive data were recorded and analyzed with Microsoft Excel 365®. Descriptive analysis was performed primarily for both age groups, as well as in trauma category-associated subgroups. When numerical data was recorded, we specified the median and range [smallest value, largest value].
5. DiscussionRates for recurrent events after a first-time dislocation event vary among different authors [
6,
17]. The risk of suffering another dislocation is higher after having suffered a prior dislocation, especially when the first-time dislocation occurred at a young age [
5,
14,
26]. The goal of successful treatment, on the one hand, is the adequate treatment of the acute trauma effects such as osteochondral damage, on the other hand, the (re-)establishment of stable joint integrity. The consequences of recurrent dislocations are far-reaching, ranging from functional limitations attributed to instability, persistent pain, and reduced stress capacity of the joint, to morphological damage such as cartilage-bone pathologies with increased risk of degenerative joint disease and reduced quality of life [
6,
12,
27].Traumatic first-time dislocations are usually treated non-surgically unless relevant osteochondral flakes are present [
6,
12,
13,
14,
15]. However, when is the cause of a dislocation event considered traumatic? If adequate trauma cannot be assumed, the cause must be sought in potential physical abnormalities. A concept of treatment can only be causally determined after a thorough evaluation of all potential underlying factors influencing the dislocation. Germany’s statutory accident insurance will cover an injury, including those with pre-existing conditions, if a certain traumatic event can, beyond a reasonable doubt, be legally accepted as the cause. Only 21% of adult knees and 20% of children’s knees in our cohort showed an absence of relevant pathological deviations. Overall, our study population of traumatic dislocations showed a large proportion of predisposing factors.A valgus configuration was a frequent predisposing factor with 20% in the adult cohort and almost twice as many in the pediatric cohort. The median values, however, did not exceed our correction limit of four degrees. There are currently no clear recommendations on the degree of axis deviation at which axis correction should be performed for patella maltracking [
28], but frontal axis deviation seems to only play a minor role in traumatic dislocations.Median torsional values also only deviated moderately from the norm for both cohorts. Considering the above-mentioned threshold values, however, clear pathologies were found in individual cases. Both groups had a similar number of cases that exceeded the threshold value for femoral torsion, while the adult population had a higher number of cases above the threshold for tibial torsion than the pediatric cohort. Thus, torsional deformities in childhood seem to play only a minor role [
29]. In adults, a torsional osteotomy is recommended with a symptomatic deviation of approximately 10 degrees or more [
4,
28]. Dickschas et al. [
4] showed that about 12% of patella instabilities are caused by torsional deformities.With a median TTTG value of 17 mm within the pediatric and 18 mm within the adult cohort, both were slightly elevated, while both groups showed a TTTG value above the correctional limit of 15 mm [
14,
22] in approximately half of the cases. The risk factor “high-riding patella” also showed increased relevance, with an incidence of just under 30% in adult cases and just over 40% in pediatric cases. Osteotomies of the tibial tuberosity were performed less frequently than would be expected based on the proportion of underlying pathology.Consistent with the increased number of cases that demonstrated trochlear dysplasia within the pediatric cohort (57%), the lateral trochlear inclination angle was less than 11 degrees in approximately one-third of cases. Unexpectedly, the adult cohort exhibited some form of trochlear abnormality in 36% of cases. In severe cases of trochlea dysplasia, a surgical re-shaping (trochleoplasty) may be indicated. Trochleoplasty may influence other predisposing factors, as patellar tilt and patellar height are influenced by a dysplastic trochlear geometry, and reconfiguration of the trochlea influences the TTTG value [
28]. Open growth plates are usually considered a contraindication for this procedure, in which case, one should resort to surgical procedures addressing the balance of associated soft-tissue structures.Schmeling et al. [
28] describe a classification system by naming five types of patellofemoral instability, which may assist clinicians in choosing an appropriate treatment regimen. Type 1 describes a traumatic patellar dislocation without maltracking or instability with a low risk of re-dislocation. Type 2 describes patellar instability without maltracking with a high risk of re-dislocation. Type 3 is defined as patellar instability with maltracking. Type 4 describes high-grade instability with loss of patellar guidance due to high-grade trochlear dysplasia, while type 5 is characterized by maltracking without instability. Types 1 and 2 can be easily interpreted and understood as traumatic events. However, the present study population demonstrated an increased incidence of predisposing factors hinting at pre-existing patellar maltracking, making it a necessity to evaluate the mechanism of trauma.Mechanisms of trauma such as stepping out of a vehicle or standing up from a seated position correspond to an everyday movement and are not viewed as adequate mechanisms of trauma for a patella dislocation to occur and were therefore grouped within the category “insufficient trauma”. Accordingly, this subgroup showed a low rate of “healthy knees” in both age groups. The children’s cohort in particular was characterized by a high proportion of trochlear dysplasia and a high-riding patella. The question arises why the proportion of this trauma category is also high in the adult cohort, as dislocations, given a relevant predisposition, would be expected to have also occurred at a younger age. This can be explained by the high proportion of recurrent dislocations within the adult cohort within the “inadequate trauma” category. Thus, these are not to be considered as traumatic. According to the allocation to type 3 or 4 of patellofemoral instability [
28], one should aim for a causal surgical therapy.Direct impact to the medial aspect of the knee, on the other hand, can plausibly cause a traumatic dislocation [
8,
30]. This theory is supported by the low proportion of recurrent dislocations and the correspondingly high proportion of first-time dislocations, as well as by the rather low proportion of underlying predisposing factors in the adult group. Comparatively, a pathological trochlear shape, patellar height, and lateral trochlear inclination angle could be witnessed more often in the pediatric cohort. There is also a lower proportion of “healthy knees” in the pediatric age group. This shows that clinicians should not be misled by the plausibility of certain mechanisms of trauma and dismiss other variables, especially in children. It remains important to consider underlying predisposing factors before initiating a certain treatment option.
The pediatric subgroup in the trauma category “rotational trauma” also showed an increase in pathological values regarding predisposing factors compared to the adult subgroup. Within the latter, however, the older age of the injured policyholders was noticeable, further supporting the trauma thesis.
With 100% first-time dislocations and the highest proportion of “healthy knees” in both age groups (60% in the pediatric cohort, 33% in the adult cohort), the trauma category “fall” represents a relevant and major cause for traumatic dislocation of the patella.
Ultimately, the surgical treatment chosen should be based on the presence of relevant predisposing factors and the resulting injuries incurred due to the dislocation event itself. In accordance with the recommendation for type 1, i.e., non-surgical treatment as long as there is no relevant osteochondral damage [
28], non-surgical treatment was initiated in 22% of adult cases and 26% of pediatric cases, corresponding to the proportions of “healthy knees”. In type 2, surgical treatment addressing the medial soft tissue is recommended [
28], while MPFL reconstruction has been shown to be superior to duplicating the retinaculum in adults [
31]. In children, MPFL reconstruction is still considered critical due to the insertion point being located at the distal femoral growth plate [
6]. Although there are studies that show a reduced risk of re-dislocation after surgical stabilization after having suffered a traumatic first-time dislocation with subsequent instability, long-term satisfaction in clinical scores is not significantly higher compared to non-surgical treatment [
13,
15,
16]. In the present study cohort, surgically addressing the medial ligamentary complex was the most common procedure performed in children and adults, in line with the above-mentioned recommendation.Contrary to one’s assumption on the treatment of mere traumatic dislocations of the patella, our study population underwent correctional osteotomies by means of tibial tuberosity osteotomy, torsional and frontal axis corrections, or trochleaplasty, as recommended for maltracking instability (types 3 and 4 [
28]). Within these cases, a sufficient mechanism of trauma is deemed questionable.

留言 (0)