The prevalence of depression among children and adolescents in China has increased significantly in recent years. Suicide events frequently occur; the suicide tendency of this population is twice that of adults, with a high recurrence rate [21]. The development of depression in children and adolescents is closely related to social, biological and psychological factors, and the age of first episodes is getting lower. Depression in this population is characterised by long-term low mood, low self-esteem, delusion, pessimism, hallucination, anorexia and even suicidal tendencies or behaviours, which seriously impact the social interaction, life and health of children and adolescents. Current clinical studies primarily focus on the treatment of depression scientifically and effectively to alleviate the condition and reduce the disability rate.
In the present study, Bifidobacterium combined with high-frequency rTMS was used for depression in adolescents and compared with oral escitalopram oxalate. The conditions of patients in the experimental group and the control group were improved. After treatment, the HAMD score decreased significantly; the levels of serum inflammatory factors, including TNF-α, IL-1β and IL-6, decreased, the levels of neuroendocrine indicators DA and 5-HT increased and that of COR decreased. Previous studies have shown that the onset of depression is primarily related to factors such as 5-HT, low norepinephrine function, dysregulated DA function in the mesolimbic system and decreased function of receptors [22,23,24]. Escitalopram oxalate is a commonly used 5-HT receptor inhibitor. It binds to the 5-HT receptor and subsequently affects the contact between 5-HT and the 5-HT receptor in the presynaptic membrane to directly reduce the uptake and increase the concentration of 5-HT in the synaptic space, which finally alleviates depression and anxiety. However, it is important to note that although the HAMD score differences between groups post-treatment were statistically significant, the clinical relevance of these differences should be interpreted with caution. The Minimal Clinically Important Difference (MCID) for HAMD-24 is estimated to be 3–5 points. The observed difference of approximately 2 points may not meet this threshold, suggesting that the real-world clinical impact of the observed changes may be limited.
In the present study, Bifidobacterium combined with high-frequency rTMS effectively improved the levels of serum inflammatory factors and neuroendocrine indicators in the experimental group. One potential mechanism for this effect is that oral probiotics, such as Bifidobacterium, may modulate gut microbiota composition, leading to an improved gut–brain axis function [25]. Research has shown that Bifidobacterium can enhance the diversity and abundance of beneficial gut bacteria, which in turn can influence the production of neurotransmitters and neuroactive compounds [26]. For instance, Bifidobacterium may promote the synthesis of serotonin (5-HT) in the gut, which is crucial for mood regulation [27]. The reduction of inflammatory factors such as TNF-α, IL-1β and IL-6 may reflect the regulation of the immune system, which in turn may positively affect the function of the central nervous system and alleviate depressive symptoms. Similarly, changes in neuroendocrine indicators enhanced neural plasticity and neural transmission, contributing to the observed clinical improvement. Furthermore, Bifidobacterium may influence the immune system by mediating immune cells to produce immunomodulators through various signalling pathways. This action can subsequently reduce the levels of pro-inflammatory factors, such as TNF-α, IL-1β and IL-6, while also regulating COR secretion, thereby affecting CNS function. By enhancing the metabolism of DA and 5-HT, Bifidobacterium may inhibit synaptic changes, protect the plasticity of hypothalamic neurons and improve overall brain function, ultimately inhibiting the development of depression.
Repetitive transcranial magnetic stimulation is a non-invasive, non-drug therapy widely used in clinical practice. During the procedure of rTMS, the magnetic stimulation coil is placed on the designated site of the scalp, usually the projection area of the prefrontal cortex. When the electric signal of the magnetic stimulator is discharged, a local magnetic field with a certain intensity is generated around the coil, and the magnetic field induces a current in the cerebral cortex. When the induced biological current exceeds the threshold of nerve cell excitability, nerve cells are activated to induce membrane depolarisation and trigger a series of physiological and biochemical reactions to relieve symptoms and treat diseases [28]. Although rTMS has shown promising results in treating various conditions, its potential impact on cognitive function remains an area of growing interest. Future studies could consider assessing cognitive function as an additional outcome measure to explore whether rTMS has beneficial effects in this domain, which may further support its therapeutic applications.
Clinical studies in recent years have found that intestinal flora dysregulation is involved in the development and progression of various mental disorders and affects the CNS and behaviour through pathways such as sustained immune response and neurotransmitter mediation [29]. In addition, gut microbiota products, such as cytokines, play an important role in the gut microbiota–brain interaction [30]. In addition, studies have revealed that gut microbiota is imbalanced in patients with MDD, the number of firmicutes is significantly higher than that of the general population and the number of probiotics in stool samples is significantly reduced [31,32,33]. In addition, changes in diet and living habits further lead to abnormal gut microflora [34]. Accordingly, conventional treatment methods, such as antidepressant drugs, alone are not effective in patients with depression. Therefore, the regulation of intestinal flora may serve as an adjuvant treatment for depression. Liu Daiyue et al. found that the improvement effect of antidepressants combined with intestinal flora regulators on clinical symptoms, adverse behaviours and cognitive function of patients with depression was better than that of antidepressants alone [35]. Bo Qiyu et al. showed that Bifidobacterium live bacteria combined with Prozac significantly alleviated the clinical symptoms and signs of patients with depression, and its efficacy was superior to that of Prozac alone in the treatment of this disease [36]. However, it is important to note that the shift in the gut microbiota may be transient and temporary. Some probiotic treatment trials did not find significant changes in gut microbiota composition after 4–8 weeks of intervention [10], suggesting that individuals may require a longer duration of treatment to achieve therapeutic effects. To advance this field, further larger-scale and longer-term studies are required.
Although the specific safety evidence of the combined use of probiotics and rTMS still needs further research, multiple studies have already supported the safety of using rTMS alone [37,38,39]. For instance, existing studies have shown that the application of rTMS in adolescents has demonstrated more significant clinical symptom improvements than in adults, and no safety or tolerability issues have been identified [39]. Furthermore, according to the “Expert Consensus on Clinical Application of Neuroregulation Techniques in Pediatrics” (2021) in China: rTMS should not be used for children under the age of 12. Therefore, the sample ages in this study were all above 12 years old. In terms of safety, no serious adverse reactions were reported in the two groups during the treatment. The treatment-related adverse reactions that the patients experienced, including headache, dizziness, hearing loss and other discomfort symptoms, were mild in severity and relieved within 1 day after the treatment. No patients discontinued treatment because of adverse reactions. There was no statistically significant difference in the incidence of adverse reactions between the two groups, indicating the favourable safety profile and tolerance of Bifidobacterium combined with high-frequency rTMS in the treatment of depression in adolescents.
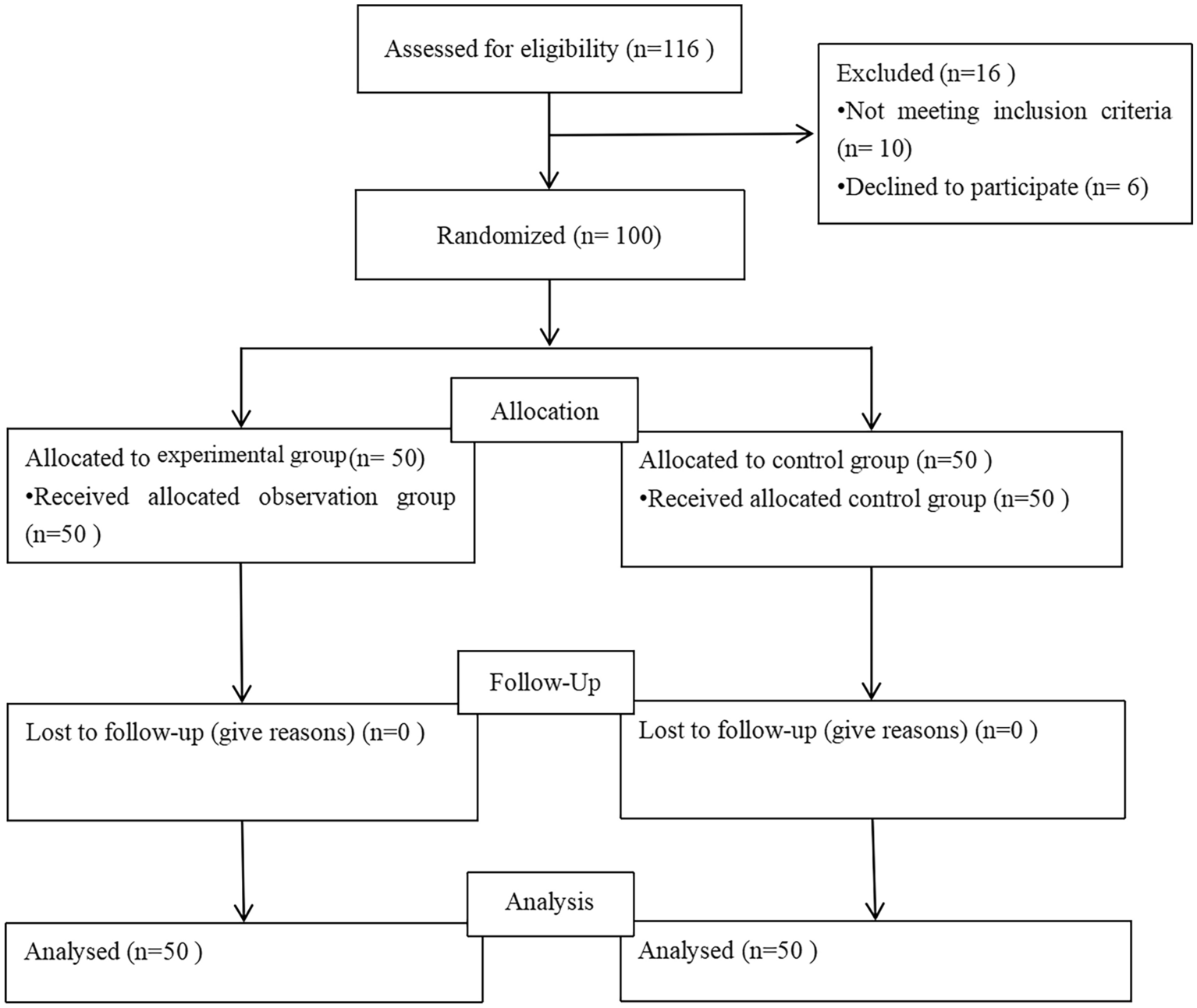
There are several limitations in the present study. First, the relatively small sample size of 100 patients may introduce selection bias and limit the generalisability of the results. Second, the short observation period restricts our ability to assess long-term effects. Additionally, conducting the study at a single centre may limit the diversity of the sample and the applicability of the findings to broader populations. Furthermore, the control group did not receive a placebo treatment, which could have influenced outcomes due to the absence of a comparison for the placebo effect. Participants from different groups were assigned to different wards as much as possible, and the packaging of the two groups of drugs was standardized. Patients in the control group were allowed to enter the rTMS treatment room, even though they did not receive treatment. Despite all these efforts we have made, we admit that some participants may still have guessed their treatment allocation. Although our primary objective was to explore the combined effects of Bifidobacterium and rTMS, we acknowledge that this design introduces a bias that makes it challenging to discern whether the observed effects are due to the individual interventions or their interaction. Furthermore, although the inter-group differences in HAMD-24 scores were statistically significant, we acknowledged that the clinical relevance of this difference was uncertain as it did not reach the minimum clinically important difference of 3–5 points. Last, we did not control for diet and lifestyle factors that may affect gut microbiota and study outcomes. Future research with larger sample sizes, longer observation periods and multicentre designs is needed to validate our findings and provide more robust evidence regarding the efficacy of Bifidobacterium combined with high-frequency rTMS in treating depression.


Comments (0)