
Remember me

This section of the results presents the first step of the qualitative data analysis focused on origins, triggers and manifestations. Given that the manifestations are the most visible part of the emotional reactions, we will begin presenting the results with the manifestations and then move on to the origins and triggers. To illustrate these results, we will include selected excerpts from the interviews conducted with the participants. Each participant has been assigned a code name: Noemie, Hadrien, Paul, Marc, Lionel, and David.
ManifestationsWe identified three physicians’ manifestations that encompass their thoughts, emotions, and behaviors towards patients. The three manifestations had a dual polarity resulting in six types of reactions.
Emotional connection/avoidanceEmotional connection was identified when physicians recognized patient’s emotions and suffering. In these situations, physicians expressed sympathy, sadness, and, in case of positive outcome, relief.
I felt sorry for him, I thought, "Why does all this happen to such a good person?" The sessions were very heavy. But at the same time, I hoped that talking with him might help. (Noemie).
On the other hand, physicians sometimes experienced negative emotions, primarily fear and anger, mostly in situations where they felt threatened, manipulated, or unappreciated.
I was angry because for me, what he was doing was an abuse of the system and of our efforts. We were trying to help him while he himself was doing nothing to move forward. (Hadrien).
In these situations, they did not invest in the therapeutic relationship and carried out their work without genuine engagement, what we called emotional avoidance.
Sometimes we have such negative feelings towards the patient that we don’t even think, "I could do this or that to help". I think that was the case with this patient. (Hadrien)
Confidence/DoubtsThe second manifestation pertained to the physician’s level of confidence in their decision-making ability. With some patients, physicians could decide on the best actions to take based on the available information and had confidence in their decision.
It was a really easy decision. I could justify it both clinically and ethically. (Noemie)
In contrast, physicians might consider the available information to be contradictory or ambiguous, and they struggled to decide. They experienced uncertainty and doubts.
She had been talking about suicide for a long time, and recently, suicidal thoughts became more intrusive. But at the same time, there was no imminent risk. So, how can I decide when to intervene? (Paul).
It was often at this moment that challenging choices regarding involuntary hospitalization versus alternative treatments should be made, with coercion potentially undermining therapeutic alliance.
I didn’t want to intervene too aggressively for fear of breaking the relationship with the patient. But at the same time, I was afraid that if she would die by suicide, someone would review the file and say, "Why didn’t you do anything? She was talking about suicide." (Paul).
Powerlessness attributed to own limitations/to the patientThe third manifestation concerned physicians’ perception of their interventions, while feeling stuck in the treatment process. The binary aspect here involved the way physicians explained the impasse. First, the impasse was attributed to the physician’s feeling of not having enough means to help the patient.
I think that when he was discharged, the suicide risk remained very high. But there was nothing more we could do. […] He wasnt particularly depressed, he was going back to the same harmful environment. He had borderline personality traits, so he could have benefited from psychotherapy, but there was no psychotherapist in his village. (Hadrien).
In this case, physicians expressed a sense of failure, powerlessness, and discouragement.
There was no improvement; we kept him in the hospital just so that he wouldnt jump in front of the subway, and we pumped him with medications. So, the most intense feeling I had was actually powerlessness. (Noemie).
Second, the impasse resulted from patients’ attitudes, and physicians attributed them a part of the responsibility.
I wanted to show him that there was a gap between what he said and what we saw. So, I told him, "You’ve been in the hospital for a while now, and there’s been no progress. So, I think you’re simply making threats to get something. But that’s not the best way to get what you want". (Hadrien).
OriginsWe identified three clinicians’ needs orienting their relationship with suicidal patients. Associated specific challenges often hindered their fulfillment.
Need to helpThe first of the physicians’ needs was the need to help by developing a relationship where they could provide patients with resources and emotional support.
Most of the time, my initial reaction is to help, to give hope. I want to say something like, "Don’t worry, we will help you get through this.” (Marc)
Nevertheless, with suicidal patients, there were two situations where physicians did not feel they were in a genuine helping relationship. The first was when patients refused help, or when physicians themselves believed that the patient’s request for help was not sincere but rather a way to exploit them.
There are some patients who, even if they dont really need hospital treatment, do everything possible to get hospitalized. And the surest way to get hospitalized in psychiatry is through suicidal ideation. (Hadrien).
The second situation was when physicians perceived their patients’ suicidal thoughts as disproportionate to the suffering they observed.
I have never had a patient for whom I thought, "He is right, given his situation, the only solution left is death." Maybe it would be different if I worked with elderly people or patients with incurable illnesses. (Lionel).
Need for securityClinicians were aware that their patients’ lives were at stake, which heightened their concern about the potential harmful effects of making a wrong decision—not only on their patients but also on their own career and reputation. Consequently, they wanted to act in a way that avoided any risk for both, themselves, and their patient.
The psychiatrist’s main interest is to avoid problems. If we let someone go and they die by suicide, everyone will say, "Why didn’t you make a better risk assessment?". (Hadrien)
However, they understood that zero risk did not exist for reasons related to the suicidal patient, as well as to the nature of the evaluation. First, the information that patients share was not always perceived as credible.
The most challenging part of the job is assessing suicide risk when a patient is not authentic. It is impossible to be certain about assessment’s validity. (David)
Second, there were no objective tools to assess suicidality, and therefore, the evaluation often remained a matter of judgment.
I have a responsibility to evaluate something that is not easy to evaluate. We cannot stage suicide risk the same way we would with cancer. (Hadrien)
Need for efficacyFinally, physicians wanted to be efficacious, meaning they aimed to achieve specific outcomes in their work with suicidal patients. However, they often experienced a sense of inefficacy.
We begin residency with a lot of hope to help people, but we quickly come up against the system’s limits. So, the biggest challenge is accepting the limits. (David)
Their sense of inefficacy was tied to two beliefs about suicidality. The first was that modern psychiatry tends to pathologize all forms of suicidality, often compelling physicians to care for patients for whom treatment offers no real benefit.
In the past, there was a more medical aspect to psychiatry. But with each new DSM version, there is a kind of expansionism. We have medicalized things like personality disorders, binge-eating… And I feel that the same thing has happened with suicide. (Hadrien).
Second, they believed that if a patient truly wishes to die, there is little they can do to prevent it.
Nowadays, there is a perpetual struggle against suicide. I think we should not have this responsibility as psychiatrists. There are hopeless cases and we are not Gods. At the end of the day, if someone wants to commit suicide, they will do it. (Noemie).
In both cases, they felt that the healthcare system assigns them responsibility without providing them with the means to fulfill it.
TriggersWe identified five triggers of emotional reactions: 1) patient’s adverse life experiences, 2) symptoms, 3) suicide risk, 4) patient’s engagement and motivation, and 5) influence of a third-party.
Adverse life experiencesPhysicians’ understanding of patients’ life conditions was dominated by a perception of present or past adversity, which might involve traumatic events, social precarity, or physical illness.
He did not have an easy life. He lived in shelters and foster homes. (Paul)
The perception of patients’ relationships with significant persons was often shaped by a lack of emotional support, neglect or abuse by loved ones.
He felt really abandoned by his family. I asked if his parents came by, and he replied that it was the first time in his life that his father hugged him. (Lionel)
SymptomsInterviewed physicians tended to have a binary perception of medical conditions. On the one hand, there were patients with clear-cut depressive, manic, or psychotic symptoms.
He was very depressed. I had no doubt. In fact, I have rarely seen a depression like this. (Noemie)
On the other hand, there were patients without symptoms of acute psychiatric illness but with pathological personality traits.
He didn’t appear depressed. He seemed normal, but he had some personality traits that were not visible at first glance. A lot of passivity, dependence… (David)
Suicide riskDegree of suicidality and its evolution captured physicians’ attention: when patients had a concrete plan and appeared determined, risk was considered high.
He had very intrusive ideas of hanging himself. So, he went to the basement, tied a rope to a beam, stood on a chair… Eventually, he got scared and didn’t do it. But he was a patient who would most likely kill himself if we let him go. (Noemie).
In other situations, when patients had chronic suicidal ideation or when physicians found their statements insincere, risk was considered low.
He was a young man who was spending his time in the unit playing cards, telling jokes, who got involved in a relationship with another patient. For him, being in the hospital was like being on vacation. But every time I met him, he would say, "I’m desperate, I only think about suicide". (Hadrien).
Physicians sometimes perceived a potential for self-harm, but assessing immediate risk was difficult due to patients’ ambiguous statements or contradictions between their current and past state.
I had two contradictory sources of information. When I read the letter, I thought, "This is an involuntary hospitalization, no negotiation". However, I had someone in front of me who said he no longer had the same thoughts as the day before. (Marc).
However, physicians also reported situations where, regardless of the degree of initial risk assessment and despite treatment, suicidal ideation persisted, or patients engaged in self-harm.
He attempted suicide after two months in the hospital. So, we went back to square one. How can we consider hospital discharge under these conditions? (David)
Patient’s engagement and motivationPatients’ overall way of engaging in the relationship with their physician and in the treatment process was among the triggers. Relationally, physicians sometimes perceived patients as genuinely connecting with them and sincerely sharing their experiences and feelings…
I was struck by the shame, the simplicity… It was inconceivable for him to have reached that point (attempting suicide). (Noemie)
...and, regarding the treatment, in some cases, patient and physician aligned on the same treatment approach.
She had experienced several depressive episodes, so she knew well her illness. It was an easy decision for her. When I talked to her about hospital admission, she said, "Okay, this is it, I’m ready to go to the hospital." (Noemie).
In contrast, some patients hindered physicians from establishing a relationship, often by displaying indifference and insulting them
He was arrogant, aggressive, cynical. I thought that if I were in his place, if I were 18 years old and facing an older doctor, I would be very respectful. (Lionel)
… or by making treatment requests that conflict with the physician’s judgment—most commonly regarding hospital admission. These involved patients insisting on being admitted when physicians saw no justification for it or refusing hospital care recommended by the physician.
I felt some pressure, as if he was trying to convince me that he wasn’t suicidal so that I would let him go. Every time I tried to address other topics, he would say, "I’m not suicidal." (David).
Influence of a third-partyFinally, physicians’ understanding of their patient’s situation was sometimes shaped by input from other healthcare professionals or the patient’s friends or family, whose perspectives might either reinforce or challenge the physician’s judgment.
I spoke with the social worker, and I told her that I felt comfortable letting the patient go. However, she told me that she was a bit worried. So, I tore up the discharge prescription I had already prepared and said to her, "OK, I will go reevaluate him. If you’re not comfortable letting him go, I’m not comfortable either." (Paul).
Origins, triggers, and manifestations are summarized in Table 2.
Table 2 Groups of origins, triggers and manifestationsRelations between origins, triggers, and manifestationsThis section presents the second step of the qualitative data analysis, in which we searched for specific patterns linking origins, triggers, and manifestations in all encounters (N = 15) described by the six participants.
Each manifestation was specifically linked to one of the origins, either explicitly by the physician or through semantic proximity in the physician’s discourse: "emotional connection/avoidance" was linked to the "need to help"; "confidence/doubts" was linked to the "need for security"; " powerlessness attributed to own limitations/to the patient" was linked to the "need for efficacy."
Furthermore, each of the six types of reactions resulting from the dual polarity of the three manifestations was associated with one or two trigger panels, forming seven distinct patterns.
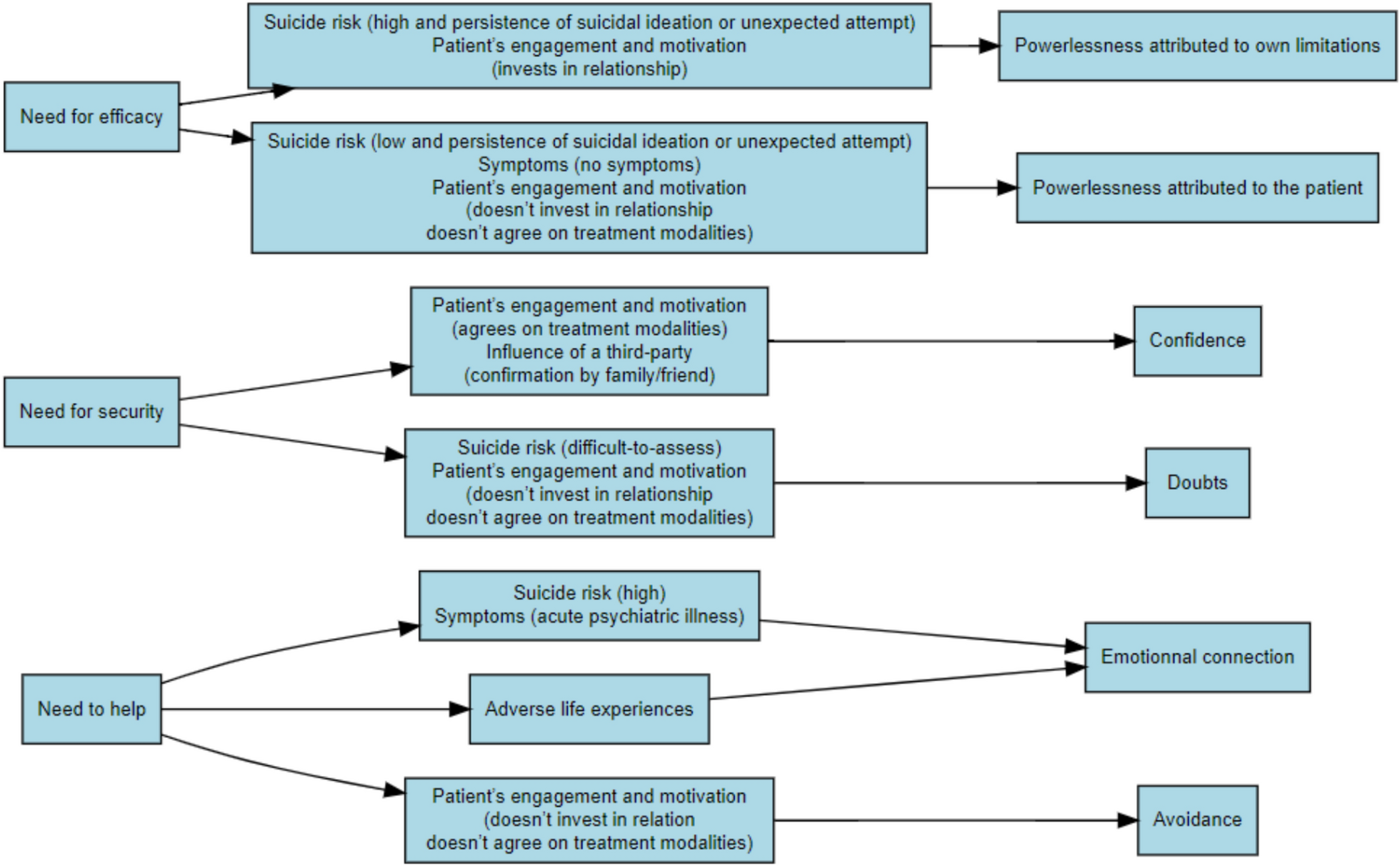
Figure 1 summarizes the 7 patterns while the set of patterns for each encounter grouped by manifestation are summarized in the Additional file 1.
Fig. 1
Flowchart showing how specific origins (left) interact with defined trigger panels (center) to generate distinct manifestations (right)
Summaries of an encounter for each of the seven patterns of origins-triggers-manifestations illustrate associations of the three components within each triad. Since the manifestations result from a combination of origins and triggers, we represent this with the formula Origin X + Trigger(s) Y = Manifestation Z.
Need to Help + (High Suicide Risk + Symptoms of Acute Psychiatric Illness) = Emotional Connection
Noemie was a young physician deeply committed to making a difference in her patients’ lives. However, she often struggled to understand patients dealing with suicidal thoughts. During a consultation at a general hospital, she met a man suffering from severe depression, who revealed that he had recently attempted suicide by hanging, abandoning the attempt at the very last moment. Noemie was struck by the intensity of his symptoms and convinced that the patient was at a high risk of suicide. She felt the patient’s pain and despair, a reaction that sharply contrasted with her usual inability in connecting with suicidal patients and felt determined to protect him.
Need to Help + Adverse Life Experiences = Emotional Connection
Providing emotional support to patients was a core component of Lionel’s professional identity. Nevertheless, he believed that no amount of grief, no matter how great, could justify suicide, and had therefore a difficult time empathizing with suicidal patients. During one of his shifts, Lionel evaluated a young man who had been taken to the hospital by a friend after attempting to jump into a river. Lionel initially experienced a negative emotional response to the patients arrogant and hostile demeanor. The patient talked candidly, during the interview, about his strained relationship with his family and his intense sense that his parents did not care about him. That enabled Lionel to interpret the patient’s suicide attempt as a desperate attempt to communicate his suffering to his parents. Reflecting on his own relationship with his father, Lionel felt a surge of empathy for the patient and a strong desire to support him through his suffering.
Need to Help + Low Patients Engagement/Motivation = Emotional Avoidance
Hadrien firmly believed that, even when they dont truly need treatment, some patients can go to great lengths to get admitted to a psychiatric hospital. According to him, the "safest and easiest" way for these patients to get admitted was to express suicidal thoughts. He therefore took care of this group of patients out of obligation and feeling that his efforts to help them were futile. He followed a patient at a psychiatric hospital who appeared to have no significant symptoms and seemed relaxed and at ease on the unit. However, in their one-on-one sessions, the patient portrayed himself as highly depressed and suicidal. The patient resisted Hadrien’s suggestion to discharge him, implying that if he left the hospital and later took his own life, it would be Hadrien’s fault. Hadrien interpreted the patients behavior as an attempt to manipulate him and this perception left him feeling angry.
Need for Security + (High Patients Engagement/Motivation + Confirmation by Family/Friend) = Confidence
For Marc, suicidal patients often have conflicting feelings about treatment. He knew that, if he had any doubts about a patients sincere commitment to treatment, his duty was to put the patients safety first. At a community center where he worked, Marc encountered a patient who had written a suicide note to his family the day before. During the interview, the patient said very little, but denied any suicidal thoughts and expressed a willingness to begin outpatient therapy if necessary. Marc made the decision not to hospitalize him but he was not totally convinced of the patients sincerity and, afterward, he felt doubts whether he had made the right choice. The next morning, the patient returned to the community center as planned, accompanied by a friend. Marc observed that the patient had followed the crisis plan, and the patients friend confirmed that everything had gone well. These signs reassured Marc and restored his confidence in the patients commitment and in his own decision to provide outpatient care.
Need for Security + (Suicide Risk Difficult-to-Assess + Low Patients Engagement/Motivation) = Doubts
David, a young physician, struggled to assess a patients suicide risk when there were doubts about the patients authenticity. He encountered a man who had arrived to the psychiatric emergency department after having texted his supervisor about having suicidal thoughts. However, during the interview, the patient denied any such thoughts stating repeatedly that he was fine and only wanted to return home. Already conflicted due to the contradiction between the text message and the patients statements during the interview, David felt that his patient was not cooperating authentically, leading to significant uncertainty about how to proceed.
Need for Efficacy + (High Suicide Risk + Persistence of Suicidal Ideation or Unexpected Attempt + High Patients Engagement/Motivation) = Powerlessness Attributed to Own Limitations
Noemie often felt that society imposes a relentless battle against suicide, and that, if a patient is truly determined to die, there is not much that can be done. She followed an adolescent at the hospital, who had heavily invested in his relationship with her. Despite trying various treatments, the patient remained highly symptomatic and suicidal, and shortly after his discharge from the hospital, he attempted suicide. Throughout his hospitalization, Noemie had struggled with a profound sense of helplessness, and when she learned of the attempt, she was overwhelmed by the belief that there was nothing she could have done to help her patient get better.
Need for efficacy + (Low Suicide Risk + Persistence of Suicidal Ideation or Unexpected Attempt + Absence of Symptoms + Low patient’s engagement/motivation) = Powerlessness Attributed to the Patient
Paul felt that the healthcare system, driven by the need to avoid legal consequences, often places on physicians the responsibility for managing suicidal patients without psychiatric disorders. He was convinced that these cases fall outside his purview. A suicidal patient he followed at the hospital had a personality disorder and chronic, though low, suicide risk. The patient often rejected proposed therapeutic options and, when upset, would imply that leaving the hospital without a satisfactory solution to his social problems might lead to his suicide. Paul was frustrated by the patients behavior that he perceived as immature and eventually told him that the challenges in his life were his own responsibility to address.
Comments (0)