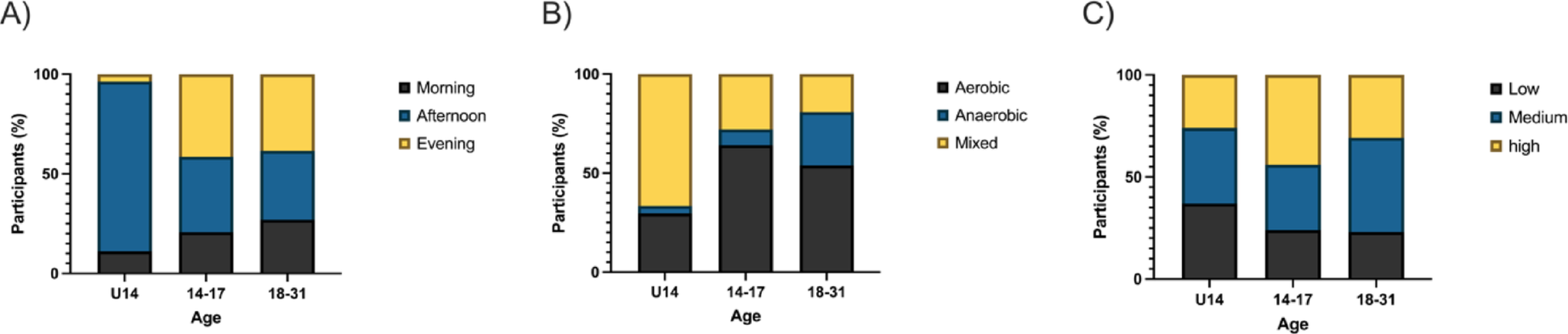
In this cross-sectional single-center study, we investigated the associations between bout-related PA – specifically its timing, type, and intensity – and glycemic outcomes in youth and young adults with T1D. Our findings indicate that exercise timing and intensity are associated with select glycemic variables, whereas exercise type showed limited influence.
Differences in glycemic responses were observed across age groups and time-of-day subgroups. Adolescents aged 14–17 years demonstrated more favorable glycemic profiles during morning sessions, exhibiting significantly lower mean glucose compared to the younger groups (U14). Conversely, morning exercise in the U14 group was associated with higher TAR and lower TIR compared to afternoon exercise, suggesting that early-day PA may not yield optimal glycemic outcomes in this younger subgroup.
These findings echo prior studies indicating that morning exercise, particularly under fasted conditions, may contribute to greater glucose stability [14]. Yardley et al. [15], for example, reported smaller declines in blood glucose following fasted morning exercise compared to sessions performed later in the day. Nonetheless, such benefits may be age- and context-dependent, as our results highlight divergent responses across developmental stages. Notably, our study did not involve fasted training, which may partially explain why morning exercise was not universally beneficial – particularly among U14 participants.
Additionally, morning sessions in the 14–17 group were characterized by elevated TBR, both compared to their afternoon/evening sessions and to younger participants. This suggests that although mid-adolescents may experience improved glycemic control overall with morning PA, they could also face a higher risk of hypoglycemia, underscoring the need for vigilant glucose monitoring and individualized insulin/CHO adjustments. Physiologically, morning exercise occurs during a time of relatively low circulating insulin levels and heightened insulin sensitivity, particularly in adolescents, which can increase the risk of hypoglycemia. Additionally, the counter-regulatory hormonal response (e.g., cortisol, growth hormone) may be blunted in some individuals at this time of day. Behaviorally, adolescents may be less likely to adequately adjust insulin dosing or carbohydrate intake before morning physical activity, especially in unsupervised or routine school-day settings. These combined factors could contribute to an increased risk of post-exercise hypoglycemia in this group.
Contrary to earlier research suggesting distinct glycemic responses to aerobic versus anaerobic modalities [15,16,17, 22], our results showed no significant differences in glycemic variables across exercise types (aerobic, anaerobic, mixed). Mean glucose, TIR, TBR, TAR, and TIME > 250 mg/dL remained statistically comparable, with only minor non-significant trends observed.
These findings may be attributed to participants’ high proficiency in diabetes self-management tailored to activity demands. As such, exercise-triggered fluctuations may be attenuated when diabetes management is optimized.
Training intensity, on the other hand, was associated with significant differences in exercise volume, particularly among younger participants (U14). In contrast, adolescents aged 14–17 years exhibited higher TAR during high-load sessions, suggesting a risk of post-exercise hyperglycemia following more strenuous activity. These findings are in line with studies showing that high-intensity training or resistance workouts, particularly later in the day, can trigger acute glucose elevations due to counter-regulatory hormone release [15,16,17, 22].
Interestingly, glycemic variables in the 18-31-year group remained relatively stable across exercise intensities, implying that age-related metabolic factors or higher PA experience may buffer against glucose variability.
Several limitations should be acknowledged. First, our study did not assess immediate post-exercise glucose responses, precluding evaluation of acute hypoglycemia or rebound hyperglycemia. Second, nutritional strategies and caloric intake were not strictly controlled and they may represent potential confounders. Third, as all participants were youth and young adults, the findings may not be generalized to older adults, who often exhibit reduced counter-regulatory hormone responses, lower CHO oxidation, and impaired glycemic correction mechanisms [23, 24].
Moreover, participant chronotype was not measured. Previous research suggests that morning or evening preferences can impact exercise tolerance and glycemic responses [25]. This variable could partly explain the observed interindividual variability in glycemic outcomes based on time of day.
All participants had access to CGM and CSII and received regular training on insulin and CHO adjustments. This likely enhanced overall glycemic control and minimized exercise-related glycemic excursions, limiting the ability to detect larger between-condition differences.
Our findings underscore the need for future research to assess:
Chronotype-exercise interactions in glycemic regulation;
Immediate post-exercise glycemia, especially for high-risk periods like overnight;
Longitudinal effects of routine PA timing and load on glycemic variability and HbA1c in broader populations, including older adults and those with suboptimal control.
Until such data are available, personalized exercise prescriptions remain critical. Rather than strictly enforcing exercise at a specific time, clinicians may achieve better adherence and outcomes by focusing on consistent, manageable PA routines tailored to individual glycemic patterns, preferences, and lifestyle factors.
While exercise timing and intensity influenced some glycemic variables in this well-managed cohort of young people with T1D, exercise type had minimal impact. Adolescents aged 14–17 years appeared to benefit metabolically from morning PA but also faced increased hypoglycemia risk. High-load training in adolescents were associated with glycemic variability, emphasizing the importance of age-specific, intensity-adjusted glycemic strategies. Overall, this study supports the promotion of regular PA in T1D, with a focus on individualization rather than rigid timing protocols.



Comments (0)