In this 13-year prospective longitudinal cohort study of an unselected population, we observed that while clinical regression of PCOS features was apparent in aging women, significant ovarian structural and hormonal differences persisted between the aging PCOS and healthy control groups. Notably, evaluations of aging PCOS women with different subphenotypes revealed no significant differences in structural or hormonal parameters between subphenotypes A-B, C, and D. Additionally, we identified an AMH threshold of 1.17 ng/mL for diagnosing PCOS at an average age of 45.3 ± 5.5 years, with moderate reliability (AUC = 0.71, 95% CI: 0.60–0.83).
Ultrasonographic evaluation in aging PCOS women and healthy controls
The ultrasonographic evaluation of aging women with PCOS remains an ongoing research topic. To our knowledge, only two studies have assessed OV, AFC or follicle number per ovary (FNPO) in aging PCOS and control patients with follow-up data [9, 23], and neither was conducted in an unselected population. Additionally, only two studies have reported age-stratified data [24, 25].
Hudecova et al. (2009) conducted a prospective cohort study evaluating 91 PCOS patients and 85 healthy controls, all aged ≥ 35 and trying to conceive at the time of assessment [9]. Since these women were diagnosed between 1987 and 1995, only NIH criteria were applicable at diagnosis. While the sample size and age range were similar to those in our study, the selection was limited to those seeking conception. The study found significantly higher OV (9.5 ± 6.6 ml vs. 6.6 ± 4.1 ml, p < 0.001) and AFC (11.7 ± 12.4 vs. 5.0 ± 2.4, p < 0.001) in the aging PCOS group compared to controls, aligning with our findings [9].
Lie Fong et al. (2017) conducted a large-scale study including 700 women with classical PCOS phenotypes (Phenotypes A & B) and 297 controls with normal menstrual cycles [23]. While OV was not assessed, FNPO declined with age in both groups, consistent with our findings. However, FNPO remained elevated in the PCOS group compared to controls. In older women, AMH demonstrated superior diagnostic performance over FNPO [AUC = 0.948 (0.927–0.970) vs. AUC = 0.874 (0.836–0.912), p = 0.00035]. A key limitation of this study was its focus on only classical PCOS phenotypes [23].
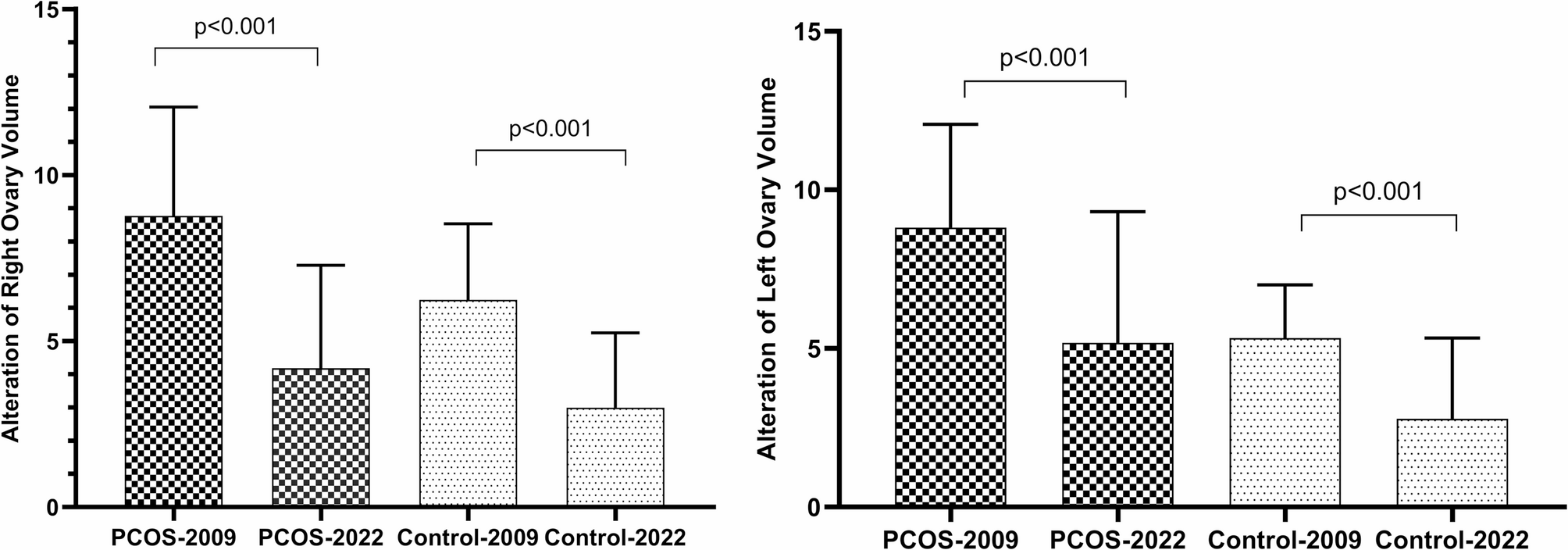
Panidis et al. (2019) conducted an observational study including 1,212 PCOS patients and 254 healthy controls, stratified into three age groups (< 20, 21–30, and 31–39 years) [24]. A significant decline in AFC with aging was observed (p < 0.018), consistent with other studies and our findings. In our study, ovarian volume, FNPO, and FNPR significantly decreased with age, particularly in the PCOS group (p = 0.047, p = 0.022, and p = 0.008, respectively). However, despite this decline, these values remained significantly higher in PCOS patients compared to controls (p < 0.001 for all), suggesting that ovarian structural changes persist with aging. This study, however, was limited to a referral population under 40 years of age [24].
A more recent cross-sectional study by Ahmad et al. (2019) included 245 PCOS patients diagnosed using NIH criteria and 756 healthy women (aged 25–40 years) from a referral population [25]. Their findings also showed significantly higher ovarian volume and AFC in PCOS women across age groups (p < 0.001), highlighting the need for age-specific AFC and ovarian volume thresholds. However, the study was limited to women under 40 and only used NIH criteria, restricting its generalizability [25].
Unlike previous studies, our study is, to our knowledge, the first to examine an unselected population of older women (aged 40–50 years). We found that ovarian volume and AFC remained significantly higher in aging women with PCOS compared to healthy controls. Moreover, at 13 years of follow-up, the PCOS group experienced a greater decline in AFC.
Hormonal evaluation in aging PCOS women and healthy controls
The current study findings align with the only two available previous studies with long-term follow-up that demonstrate an improvement in the biochemical and clinical profiles of PCOS with age [8, 26]. A study by Schmidt et al. (2011) reported a higher FAI and lower FSH levels in older postmenopausal PCOS women (60–79 years old) compared to controls, consistent with the current study observations [26]. However, unlike Schmidt et al., we found persistently higher levels of TT and DHEAS in the aging PCOS group, which may be due to differences in the study populations. Schmidt et al. was conducted in a hospital referral population that included older women (61–79 years old), whereas this study included an unselected population with a younger average age (45.3 ± 5.5 years). Additionally, while SHBG was lower in the PCOS group, the difference was not statistically significant, which contrasts with the significantly lower SHBG levels reported by Schmidt et al. [26].
Similarly, a long-term follow-up study conducted between 1991 and 2021 evaluated 596 patients diagnosed with PCOS according to the Rotterdam criteria [8]. Only those who repeatedly visited the outpatient clinic were included. The study also classified women with PCOS into sub-phenotypes. Estimated changes per 5-year age interval were calculated using multilevel linear and logistic regression analyses on data from 596 women who visited the outpatient clinic a total of 1,318 times [8]. A significant decline in TT, FAI, DHEAS, and AMH levels, along with an increase in SHBG with age, was observed [8]. These findings align with those of the current study, except for the nonsignificant change in SHBG levels. The discrepancy in SHBG levels may be due to the referral population, particularly the inclusion of hospital-based cohorts requiring more frequent visits, which introduces selection bias, as the most severe cases of PCOS may have been more likely to continue visiting the clinic repeatedly [7, 8].
Phenotypic changes over time
Phenotypic variations in PCOS have been documented with aging. Keizerswaard et al. [8] observed declines in the proportions of Phenotypes A, B, and D, with an increase in Phenotype C over time (~ 30 years of aging) in the selected study population. Similarly, Panidis et al. [24] reported a shift in phenotypic distribution, reporting that Phenotype A decreases with advancing age, while other phenotypes increase with age, but did not evaluate hormonal or ovarian morphology within phenotypes. In the current study, although the design could not permit to assess distribution of phenotypes, it expands on this by assessing hormonal and ovarian parameters within phenotypes. Despite phenotypic differences in younger women [21], we found no significant differences in modified-FG scores, TT, SHBG, FAI, DHEAS, or ovarian morphology among phenotypes during the aging period. This underscores the convergence of phenotypic profiles with age.
The role of AMH in diagnosing PCOS in older populations
AMH has been extensively studied as a potential diagnostic tool for PCOM and PCOS. In our cross-sectional study of an unselected prevalence study population, AMH demonstrated moderate diagnostic accuracy for PCOS across different criteria, with an adjusted AUC of 0.80 (NIH criteria), 0.74 (Rotterdam criteria), and 0.71 (AE-PCOS criteria). The diagnostic threshold for PCOM was 3.31 ng/mL (AUC: 0.87, 95% CI: 0.83–0.90, sensitivity: 53.1%, specificity: 93.2%), while for PCOS (according to Rotterdam criteria), it was 4.17 ng/mL (AUC: 0.74, 95% CI: 0.67–0.81, sensitivity: 38.5%, specificity: 91.1%). AMH showed the highest predictive value for phenotype A (AUC: 0.85, 95% CI: 0.77–0.92) but performed poorly for phenotypes B, C, and D [20].
Other recent studies on the referred population and their validation studies, including Dietz de Loos et al. [14] (n = 455 PCOS), Sathypalan et al. [16] (n = 105 PCOS), Saxena et al. [17] (n = 45 PCOS), Tehrani et al. [18] (n = 321 PCOS), and Piltonen et al. (n = 2917 PCOS) [15] suggest age-specific thresholds for AMH for diagnosis of PCOM, with values ranging from 3.2 to 4.9 ng/mL in younger cohorts.
A 2024 meta-analysis of 106 studies (including 19,465 cases and 29,318 controls) confirmed AMH as a valuable biomarker for PCOS, with pooled sensitivity and specificity of 0.79 and 0.82, respectively (AUC: 0.90, 95% CI: 0.87–0.93). Overall, a threshold of 5.39 ng/mL demonstrated high diagnostic accuracy (sensitivity: 88.6%, specificity: 92.75%) [27].
While AMH offers an accessible alternative to ultrasound for defining PCOM, technical challenges related to assay variability and standardization have delayed its integration into diagnostic criteria. However, a recent international consensus [5] now endorses AMH for defining PCOM in adults, marking a significant shift in PCOS diagnosis [28]. The 2023 International PCOS Assessment and Management Guidelines emphasize that AMH should not be used alone for diagnosis but can serve as a supporting criterion. Additionally, factors such as age, BMI, contraception use, surgical history, and menstrual cycle timing should be considered [5].
However, these thresholds are unsuitable for aging women due to age-related declines in AMH. In the current study, we identified an AMH threshold of 1.17 ng/mL for diagnosing PCOS in women with an average age of 45.3 ± 5.5 years. Although this threshold demonstrates moderate reliability (AUC = 0.71, 95%CI: 0.60–0.83). The observed differences in threshold values across studies highlight the importance of considering age in AMH-based diagnostics.
Strengths and limitations
This study is unique in the inclusion of an unselected population with a follow-up duration of 13 years, and subgroup analysis based on phenotypes at baseline. These factors enhance the generalizability of our findings and provide valuable insights into hormonal and ovarian structural changes with aging. However, the study’s limitations include the relatively small sample size and variations in AMH measurement methods between 2009 and 2022 may have influenced results, although comparisons were conducted separately for these time points.







Comments (0)