This paper examined the cost-effectiveness of eight program delivery strategies, designed to alleviate symptoms of anxiety and depression among young children taking a health care perspective. As highlighted in previous research [9], the scarcity of resources in youth mental health necessitates budget al.location based on cost-effectiveness analyses to maximize health outcomes in the population. It is important to find a balance between the allocation of sufficient resources to reduce symptoms and prevent the onset of mental disorders, without allocating unnecessary resources that alternatively could have been used elsewhere.
Our analysis revealed that LLN, the long version with low parental involvement and no feedback, and SLN (the hybrid version, with low parental involvement and no feedback) emerged as efficient strategies for reducing depressive symptoms and improving QALY. While not on the frontier, SHN, the hybrid version with parental involvement and no feedback, was very close to being cost effective and could, in some instances, also be a possible strategy. For anxiety symptoms, slightly altered preferences were discerned, favoring the LLF (long version with low parental involvement and feedback) and the SLF (the hybrid version with low parental involvement and feedback) in addition to SLN as these strategies were on the cost-effectiveness frontier. Our hypothesis that the least resource-demanding alternatives would be the most cost effective was partially supported; however, the more resource-demanding alternatives also proved to be cost-effective.
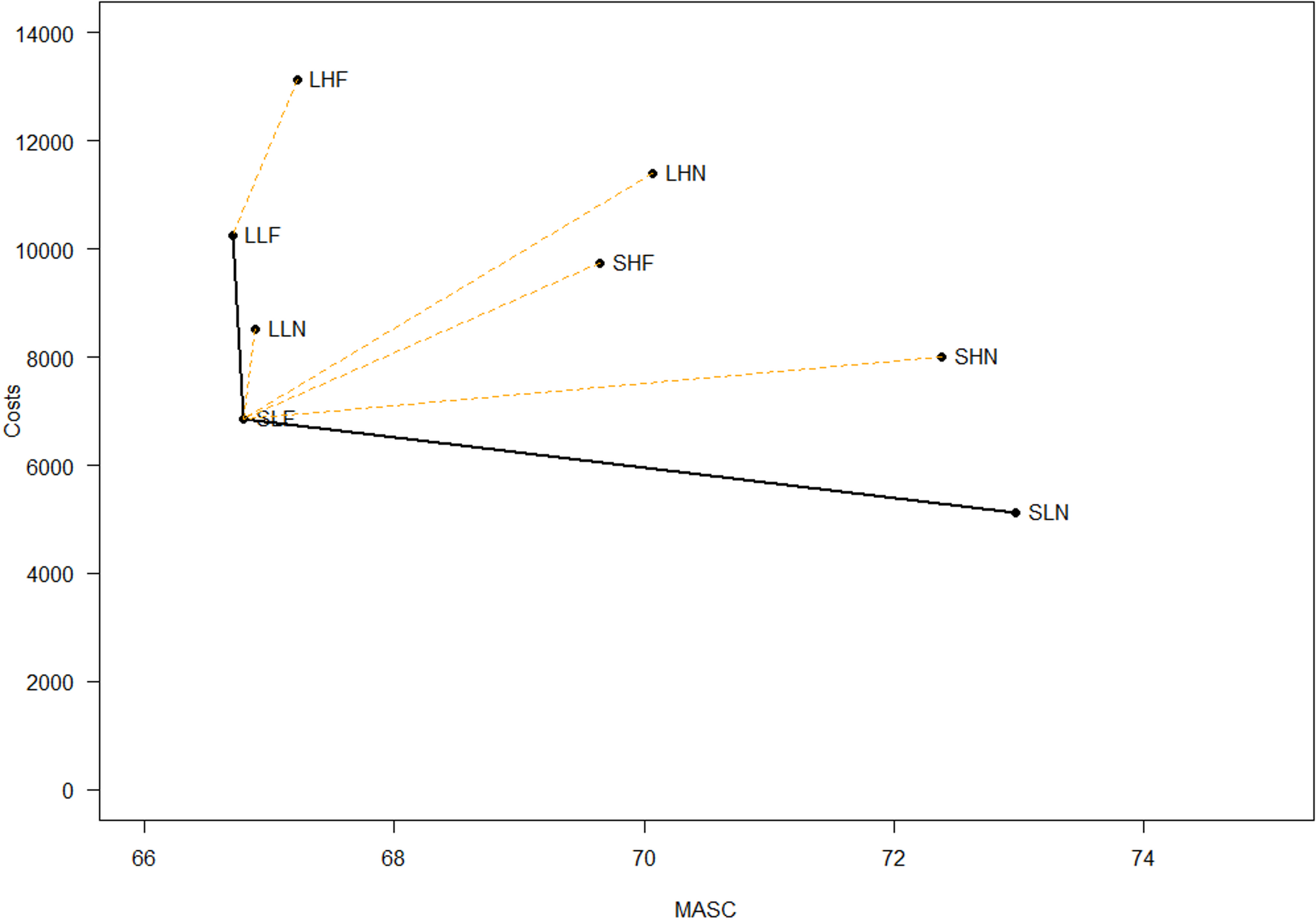
Examining the results more closely for anxiousness, the cost-effectiveness frontier reveals that SLN, SLF, and LLF are all on the frontier. This means these interventions are among the cost-effective options available. Comparing the different results, however, reveal that it appears to be important to determine resource intensity versus effectiveness as the SLN (short/hybrid solution with low parental involvement and no feedback) is the least resource-intensive intervention. However, it also results in the least reduction in anxiety symptoms (6.2 points Less compared to SLF and 6.3 points less compared to LLF). This indicates a trade-off between cost and effectiveness regarding symptom reduction. The SLF (short/hybrid, low parental involvement, and feedback) has higher costs than the SLN alternative, but results in greater symptom reduction. Of these two cost effective alternatives, SLF therefore emerges as the preferred intervention as it is a better balance between costs and reductions in symptoms. This suggests that the addition of feedback, even with slightly increased costs, improves the intervention’s effectiveness. Comparing the two other cost-effective alternatives, SLF and LLF, although LLF has higher costs than SLF, it offers only marginally better reductions in anxiety symptoms (difference of 0.09). This implies that the additional investment in LLF does not yield substantially better outcomes compared to SLF, reinforcing that SLF is the preferred cost-effective alternative. These results align with Lee, Barendregt and collegues [14], who found that school-based, internet delivered preventive interventions can be more cost effective compared to the more resource-demanding face-to-face interventions. Examining accumulated means over an extended period as is done in the current analysis makes it possible to capture sustained changes in outcomes measured by the MASC. Establishing the clinical significance of these changes remains a challenge, but is important in a preventive context where even small reductions in symptoms can be meaningful and especially so if they result in improved quality of life and better functioning. However, there are no standard methods for determining what should be used as a cutoff for clinical relevance. A difference of 6.2 points between two alternatives that both are on the cost effectiveness frontier may be clinically meaningful in this preventive setting. This perspective is reinforced by the overall reduction observed in MASC scores from T1 to T2 in this study as reported in Lisøy, Neumer [22], where reductions varied between 10.09 and 12.60 points. The MASC has demonstrated good psychometric properties [31]. Studies also show that even moderate score changes may be associated with improvements in functioning, relationships, and school performance [45]. Hence a 6.2 point reduction between cost effective alternatives could indicate a meaningful change with improved management of the youth’s health.
When evaluating options near the frontier, the strategy LLN (long with low parental involvement and no feedback) is “Extended dominated”. This indicates that, although LLN is not the least effective option when compared to the alternatives, it falls short in cost-effectiveness relative to the strategies on the frontier. In other words, LLN is not a preferable choice as there are other strategies that provide equivalent or better outcomes at lower or comparable costs. We therefore exclude LLN from consideration when optimizing resource allocation in the services.
Examining the cost effectiveness results for depressive symptoms, the SLN and LLN were positioned on the cost-effectiveness frontier (Fig. 2), indicating they are the most efficient use of resources given their cost and effectiveness profiles. Upon closer analysis, the intervention SLN (Hybrid version with low parental involvement and no feedback) is the least costly option. However, in the same way as for anxiousness, it also provides the lowest change in accumulated symptoms of depression compared to LLN. This means that while SLN might be preferred in scenarios where resources are particularly scarce, its effectiveness in reducing symptoms is smaller. The intervention LLN (Long version with low parental involvement and no feedback) has the highest costs among the two preferred interventions, but also offers the greatest reduction in symptoms, with a difference of 2.1 points on the SMFQ compared to the SLN. This makes LLN the best option for maximizing symptom reduction, but at a higher cost. While the strategy SHN (Hybrid version with high parental involvement and feedback) is not on the frontier, it is worth mentioning as a possible alternative. This strategy has higher costs than SLN, but it provides an additional symptom reduction of 1.7 points on the SMFQ, and the additional symptom reduction compared to LLN is only 0.4 points. This suggests that SHN might be a strategy to consider due to its greater efficacy in reducing symptoms if additional resources are available although it is just extended dominated. Again, it is not well established what a meaningful difference for depressive symptoms could be in this preventive context. The SMFQ has been validated in diverse populations and demonstrates strong psychometric properties [34]. Furthermore, studies indicate that the SMFQ is sensitive to change: for instance, Thabrew and colleagues [46] reported that the SMFQ exhibits ‘satisfactory sensitivity to change in a help-seeking adolescent sample with mild to moderate symptoms”. Examining the changes in scores for all the different delivery strategies as reported in Lisøy, Neumer [22], the reductions from T1 to T2 ranged between 2.36 to 2.70, and a difference in symptoms reductions in the cost-effective alternatives on the frontier of up to 2.09 points could most likely be clinically important as they are close to the actual reductions achieved from pre to post intervention. All other interventions are dominated by SLN and LLN, meaning they provide less cost-effective solutions.
The cost-effectiveness analysis for quality adjusted life years (QALYs) reveals that, similar to the findings for symptoms of anxiety (MASC) and depression (SMFQ), the intervention SLN (Hybrid version with low parental involvement and no feedback) is on the cost-effective frontier (Fig. 3). SLN incurs lower costs compared to alternative strategies, although it offers lower QALYs than the other options. This suggests that while SLN is affordable, its effectiveness in improving QALY is lower. The intervention LLN (Long version with low parental involvement and no feedback) is also considered cost-effective. It provides a higher QALY at a reasonable incremental cost (NOK 3386), positioning it as a favorable alternative for enhancing quality of life while maintaining cost efficiency. Other strategies such as SHF, LLF, LHF, and SLF are not on the cost-effectiveness frontier. SLF and SHN are however categorized as extended dominated, and remain close to the frontier, suggesting a degree of cost effectiveness under certain conditions. Both strategies align with the results of the SMFQ and the MASC, indicating their proximity to the frontier and potential as alternative options.
Examining the results in relation to the Norwegian threshold per QALY set to NOK 275,000 [25], the cost for the most expensive strategy is 95,188, which is well within the acceptable range.
The SLN remains a preferred option due to its low resource demands, and aligns with our findings for (MASC) and (SMFQ). The LLN intervention also holds a position on the frontier when examining depressive symptoms, reaffirming its cost-effectiveness in various outcome measures. Another short-duration strategy, SHN, involving parents with five parental meetings, lies close to the frontier, reinforcing its alignment with SMFQ outcomes. SLF, though extended dominated, aligns comparably with the cost effectiveness results of MASC.
Healthcare decision-makers should consider that while SLN has the lowest costs, LLN is also on the frontier and offers a better quality of life. Emphasizing these interventions can yield notable improvements in health outcomes, justifying their costs when resources permit.
In the analysis we included costs related to the intervention and its delivery, hence other costs related to the use of healthcare services and/or social services are not included. This leads to an underestimation of the costs for each child in the trial. Whether inclusion of these costs would result in changes in incremental costs is uncertain. If the use of services declines with improved health, incremental costs are overestimated. On the other hand, increased knowledge and follow-up can also initiate increased demand for services and help, which could increase the incremental costs.
We should also bear in mind that for youths in particular, the economic impact of poor mental health extends beyond healthcare costs to sectors such as education and justice [47,48,49]. The lack of investments in prevention, as pointed out by McDaid, Park [50] may be due to exactly the fact that prevention often involves multiple sectors where the costs may be incurred in one sector, while the benefits are incurred in another sector, and often later, or that the sector does not have improving mental health as its primary objective. For instance, schools prioritize education and may lack resources for preventive interventions, and the health sector benefits do not directly impact the educational sector.
Examining the association of the variables, the moderate positive correlation at T1 between MASC and SMFQ was 0.438, p < 0.001, suggesting that higher anxiety symptoms tend to be associated with higher depressive symptoms. We found a correlation coefficient between MASC and HRQoL of -0.368, indicating that higher anxiety symptoms tend to be associated with lower HRQoL. Lastly, the correlation coefficient between SMFQ T1 and QALYS T1 was − 0.597, which indicates a strong negative correlation, suggesting that higher depressive symptoms tend to be associated with lower HRQoL. The significant correlations between these primary outcomes indicate the interconnected nature of mental health symptoms and overall quality of life. Interventions targeting reductions in anxiety and depressive symptoms could potentially lead to improvements in quality of life.
The comprehensive cost-effectiveness analysis across different measures—anxiety symptoms (MASC), depressive symptoms (SMFQ), and QALYs, provides guidance on how to optimize the allocation of resources for mental health interventions.
Given intermediate resources, interventions like SLF provide a balance between cost and effectiveness and should be prioritized over less effective yet cheaper strategies like SLN. A focus on SLF can lead to better health outcomes while ensuring that the additional resources invested lead to important improvements in symptom reduction for anxiety. Furthermore, SHN also strikes a balance between cost and reduction of symptoms and may be a possible alternative. This aligns with principles of health economics and effective resource utilization.
For resource-limited settings SLN may serve as a choice due to its low cost, despite its modest effectiveness. This may for instance be the case with limited personnel in primary health services. To provide a more cost-effective intervention where reach is improved and with acceptable reductions in symptoms is obtained, may therefore ensure that research-based interventions are adopted in the health services.
LLN, however, is preferred in more ideal situations where the priority is health outcomes over costs, justifying its superior reduction in depression symptoms.
Strengths and Limitations.
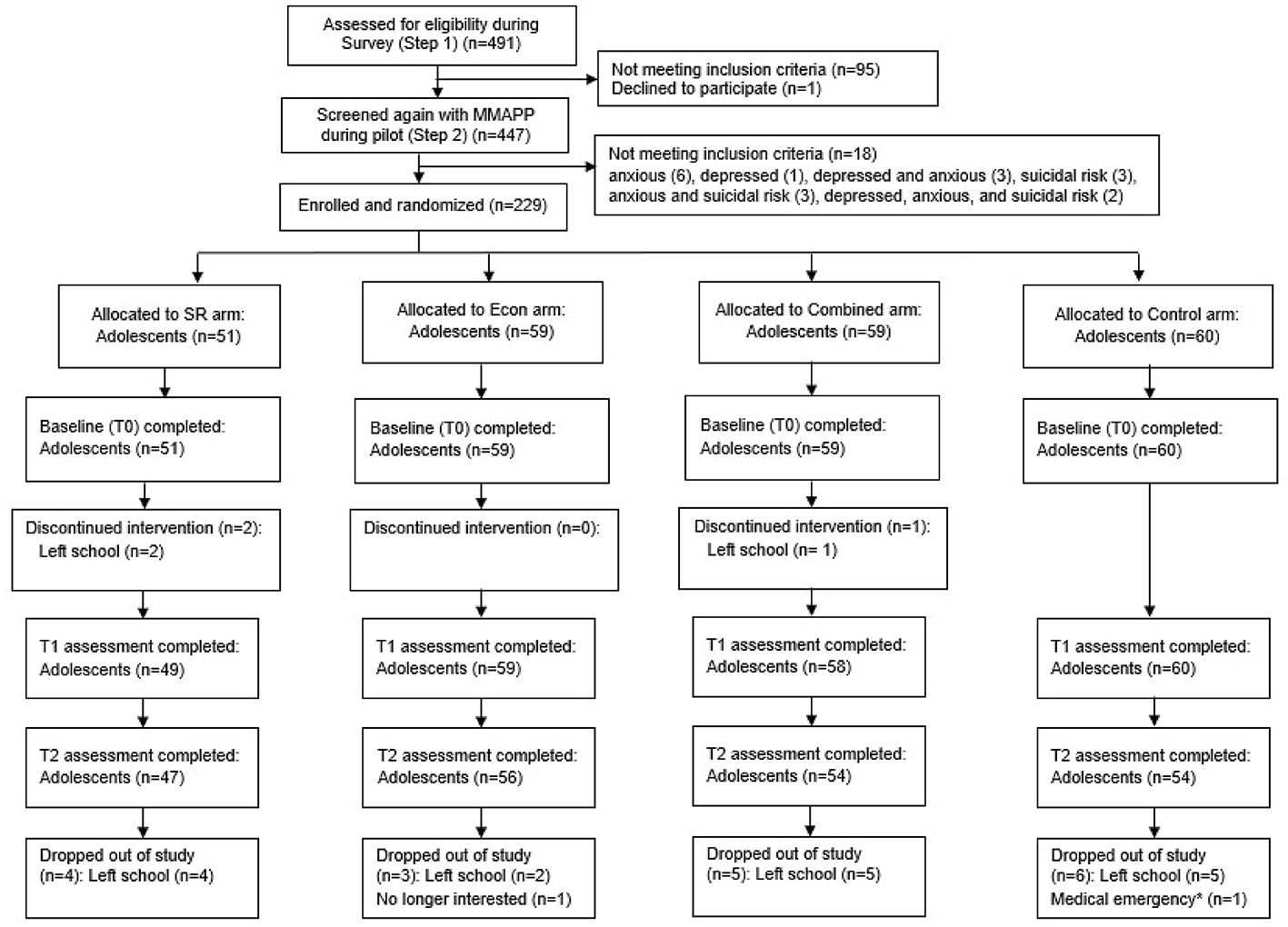
The trial’s large sample size with participants from both urban and rural schools across the country, enhances the generalizability of the findings. The innovative factorial design allowed for a comparison of different delivery strategies of an intervention targeting common mental health problems in youth. Child anxiety and depression symptoms were assessed using well established and validated measures. Additionally, the study achieved satisfactory child response rates across all three timepoints, ensuring reliable longitudinal data. The trial, conducted within a real-world school setting and utilizing first-line school health nurses as group leaders, supports the practical interpretation of results and the potential for translating research into practice.
However, the study also presents limitations:
While researchers have recommended factorial designs in new and innovative optimization frameworks, few cost-effectiveness studies have employed this design. As a result, there are no well-established guidelines for examining cost-effectiveness specifically tailored to such designs.
The absence of a control group in this study receiving no strategy or combination of strategies, which could be compared to the eight different intervention delivery strategies, is another notable limitation. Control groups are commonly used to establish baseline measures in cost-effectiveness analysis, offering a point of comparison for evaluating incremental benefits of interventions, while in this study we compared cost effectiveness of eight different alternatives.
Furthermore, examining costs and outcomes using the Incremental Cost-Effectiveness Ratio (ICER) may pose challenges. Although researchers can adapt ICER to a factorial design, they typically use it to compare an active intervention against a control condition. For factorial studies involving multiple strategies, there is no established consensus on the best method to determine cost-effectiveness [20]. According to Dziak [20], the fundamental concepts of the cost-effectiveness frontier still apply, but it remains a dilemma between developing a complex versus a parsimonious model, each having its own set of advantages and disadvantages.
Another important consideration is the choice of comparator strategies included in the study. As pointed out by O’Mahony, Naber [51], the ICER will depend both on costs and effects of the strategy, as well as on which strategies researchers include for comparison. While we included strategies based on a rationale of examining different strategies for ensuring effectiveness and delivery of the intervention, we cannot rule out that other strategies could have been relevant to include. While cost-effectiveness from a health service perspective was the aim of this study, the results could possibly have presented otherwise if all costs, including costs of parental involvement and parental absenteeism from work related to the child’s problem, use of other healthcare and social services, had been included.
In the analyses above, results are based on mean values, not taking uncertainty in the health outcomes and costs into account. Uncertainty in the health outcomes could have been explored by the variation in individual health outcome scores according to strategies. However, regarding costs this was not possible as we estimated costs per strategy, not varying between individuals. With more detailed information on costs, additional analyses would be relevant to include.
Lastly, although validated measures for clinical outcomes were used, we derived the calculation of Quality-Adjusted Life years (QALYs) from ten items of the Health-Related Quality of Life (HRQoL) measure Kidscreen, using an algorithm developed by Chen et al., 2014 for this purpose. This reliance on a subset of items, and a specific algorithm may introduce some degree of uncertainty in the assessment of QALYs. The use of QALYs is the recommended outcome measure according to Norwegian guidelines for priority setting, but where EQ-5D-5 L is the preferred instrument [52]. Whether EQ-5D-5 L would derive at similar findings would have to be analyzed in future studies.



Comments (0)