The systematic review identified a range of COPD self-management interventions implemented across Asian LMICs, revealing promising outcomes in improving health-related quality of life, reducing healthcare utilization, and enhancing self-management behaviors. The reviewed studies predominantly involved adult participants with moderate to severe COPD, highlighting the vulnerability of this population. Interventions varied from educational and exercise-based programs to technology-supported and nurse-led initiatives, with many demonstrating significant improvements in respiratory function, reduced hospitalizations, and lower out-of-pocket expenditures.
Impact of self-management interventions on COPD outcomes in low- and middle-income countries in Asia
The findings from this systematic review highlight both the potential benefits and the challenges of implementing COPD self-management programs in low- and middle-income countries (LMICs) in Asia. Given the significant burden of COPD in these regions and limited financial resources to support expanded healthcare services, self-management programs offer a promising strategy for improving patient outcomes while reducing the financial strain on healthcare systems. This review demonstrates that self-management interventions can enhance HRQoL interventions [25, 27, 28, 31], reduce exacerbation rates in China [30], and lower OOP costs in specific settings [32]. However, the variability in outcomes across studies indicates that context-specific barriers and facilitators affect these programs’ success.
The effectiveness of self-management programs in LMICs is closely linked to factors such as healthcare infrastructure, socioeconomic conditions, and cultural attitudes toward disease management [33]. Community-based interventions and digital health solutions have effectively improved COPD outcomes [29, 30]. Nevertheless, the benefits are often limited by issues related to health literacy, digital access, and financial constraints, especially in rural and underserved areas [34]. These challenges suggest that transferring self-management strategies from high-income countries to LMICs requires careful adaptation to meet local needs.
A significant barrier to the successful implementation of self-management interventions in Asian LMICs is the high OOP healthcare expenditure [3]. This financial burden can lead to delays in diagnosis, limited access to preventive care, and inconsistent adherence to treatment, resulting in more frequent exacerbations and hospitalizations [35]. Programs that reduce COPD-related costs should consider incorporating support mechanisms like insurance or community health workers (CHWs) to address these financial challenges.
While this review confirms the potential for self-management programs to provide a sustainable approach to COPD management in resource-constrained settings, it also emphasizes the need for region-specific modifications. For instance, studies showing high adherence to mobile health applications [30] suggest that digital interventions could be effective in urban areas with robust digital infrastructure.
In contrast, rural settings may benefit more from initiatives led by community health workers, offering regular, personalized support in areas with limited technology access [36]. CHW-led interventions in Nepal significantly improved patients’ inhaler techniques and functional ability, addressing health literacy and access gaps [24]. Movakher et al. found that home-based self-care programs with follow-up support, often facilitated by primary healthcare workers, reduced hospital readmissions and enhanced HRQoL in Iran [27]. These models were especially effective in rural and underserved regions, where access to formal healthcare systems is often limited. By acting as intermediaries, these individuals bridged gaps in health literacy, ensured adherence to treatment plans, and facilitated early recognition and management of exacerbations [37, 38]. This community-led approach is particularly valuable in addressing socioeconomic barriers, as it eliminates some of the direct and indirect costs associated with accessing care, such as transportation and consultation fees [39,40,41].
Such programs also offer a cost-effective alternative for healthcare systems. Zhang et al. highlighted that hospital outreach pulmonary rehabilitation programs reduced healthcare utilization while alleviating patient financial burdens [32]. CHWs or volunteer-led programs achieve similar results by shifting care delivery from more expensive tertiary facilities to community settings, reducing financial strain on health systems while maintaining or improving patient outcomes [42, 43]. These models align well with the broader goal of reducing OOP healthcare expenditures, a critical concern in LMICs where catastrophic health spending is common among COPD patients [30]. Additionally, these programs promote equity in care, ensuring that vulnerable populations, such as those in remote or economically disadvantaged areas, receive adequate support [21].
Overall, the results indicate that self-management programs can positively affect COPD outcomes in LMICs. However, the evidence regarding cost-effectiveness and cost-utility is limited, as only one included study [32] reported cost-related outcomes, showing that the program achieved CN¥3,655.94 in medical savings per patient per year and that every ¥1 spent led to ¥3.29 in savings. Given this limited evidence base, it is difficult to draw broad conclusions about the economic impact of COPD self-management programs in LMICs. Successful implementation still requires careful adaptation to each region’s unique healthcare challenges. Enhanced collaboration among healthcare providers, policymakers, and community organizations will be essential to optimizing these interventions and maximizing their impact on patient health and financial stability.
Although none of the included studies explicitly applied formal implementation frameworks, several theoretical models could strengthen the design and delivery of COPD self-management interventions. The Common-Sense Model of Illness Perceptions (CSM) links patients’ illness beliefs with self-management behaviors and quality of life, with interventions such as cognitive reframing demonstrating improvements in exercise capacity and well-being [44]. Social Cognitive Theory (SCT) emphasizes the role of self-efficacy and observational learning, with cognitive-behavioral strategies and peer modeling significantly reducing hospitalization rates [45, 46]. The Information–Motivation–Behavioral Skills (IMB) Model highlights how knowledge, motivation, and behavioral skills predict success in self-management. IMB-based interventions explain substantial variance in self-management outcomes [47]. Self-Determination Theory (SDT) focuses on autonomy, competence, and relatedness, showing strong associations with improved self-management knowledge and health-related quality of life [48]. Finally, Chaos and Complexity Theory offers a flexible, dynamic systems approach, advocating for personalized interventions that adapt to the unpredictable nature of COPD progression [49]. Future research should consider integrating such frameworks to enhance intervention design, implementation fidelity, scalability, and patient-centered outcomes in COPD self-management programs.
Quality of the study
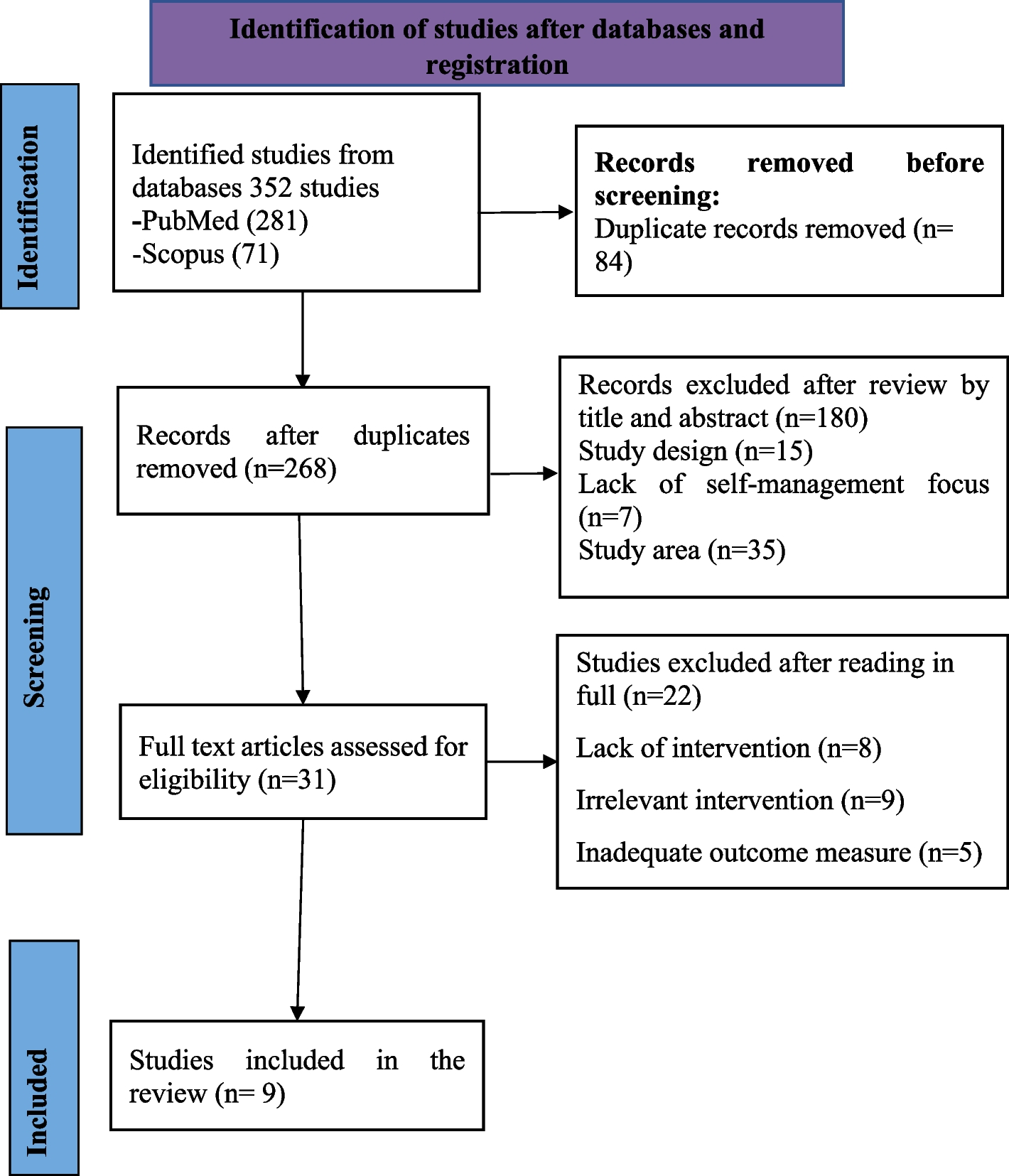
It is essential to highlight that all nine papers included in this review had a moderate risk of bias. Studies with good sample power and well-conducted methodology allow for more precise generalizations. However, the quality of the included studies does not allow generalizations, and their results should be interpreted concisely and cautiously.
Study strengths
The review provides essential insights into self-management interventions for COPD, particularly in Asian LMICs. These countries face unique challenges in healthcare delivery due to limited resources and high out-of-pocket expenses. The review examines various intervention strategies, including digital health solutions, community-based initiatives, and nurse-led programs, offering a comprehensive understanding of self-management approaches that can be tailored to local contexts.
One of this review’s significant contributions is its focus on health outcomes and cost-effectiveness analysis, essential for healthcare decision-making in resource-limited settings. The review equips policymakers and healthcare administrators with practical evidence to implement sustainable COPD management programs by evaluating different types of interventions alongside their costs. This thorough approach identifies cost-effective solutions that can be feasibly integrated into the healthcare systems of LMICs while maximizing patient benefits.
Additionally, including diverse intervention strategies allows for comparative analysis, helping stakeholders choose the methods that best align with their healthcare context and available resources.
Limitations
The systematic review has several limitations that should be taken into account. The differences in study design, quality, and sample sizes among the included studies lead to significant variability, making direct comparisons difficult. This challenge is particularly apparent in studies that report moderate bias levels in outcome measurement and adherence to interventions. Furthermore, while focusing on Asian LMICs provides valuable insights for that region, it may restrict the generalizability of the findings to other low-resource settings. This limitation stems from the differences in healthcare infrastructure, cultural practices, and socioeconomic conditions in different areas. Another limitation of this review is the scarcity of economic evaluations among the included studies, which limits conclusions regarding the cost-effectiveness and financial sustainability of COPD self-management interventions in LMICs.
Future research
Future research should focus on tailoring COPD self-management interventions to address the unique challenges in Asian LMICs. Studies should explore context-specific strategies for rural and urban areas, emphasizing disparities in digital access, health literacy, and financial resources. Digital health solutions, such as mobile health applications, require further evaluation for long-term effectiveness and accessibility, particularly in underserved regions. Additionally, targeted interventions for high-risk groups, such as elderly patients or economically disadvantaged populations, are essential to develop personalized approaches that enhance adherence and health outcomes.
Cost–benefit and cost-effectiveness analyses are critical to inform policy implementation in resource-constrained settings. Research should assess how community-based models and insurance-driven interventions can reduce out-of-pocket expenditures and healthcare costs while improving access to care. Community health worker-led programs and subsidy-based approaches should also be studied for their potential to address healthcare inequities and increase program sustainability. Additionally, integrating theoretical frameworks like the Common-Sense Model of Illness Perceptions and Social Cognitive Theory into intervention designs could help enhance their effectiveness and adaptability to diverse patient populations in LMICs.



Comments (0)