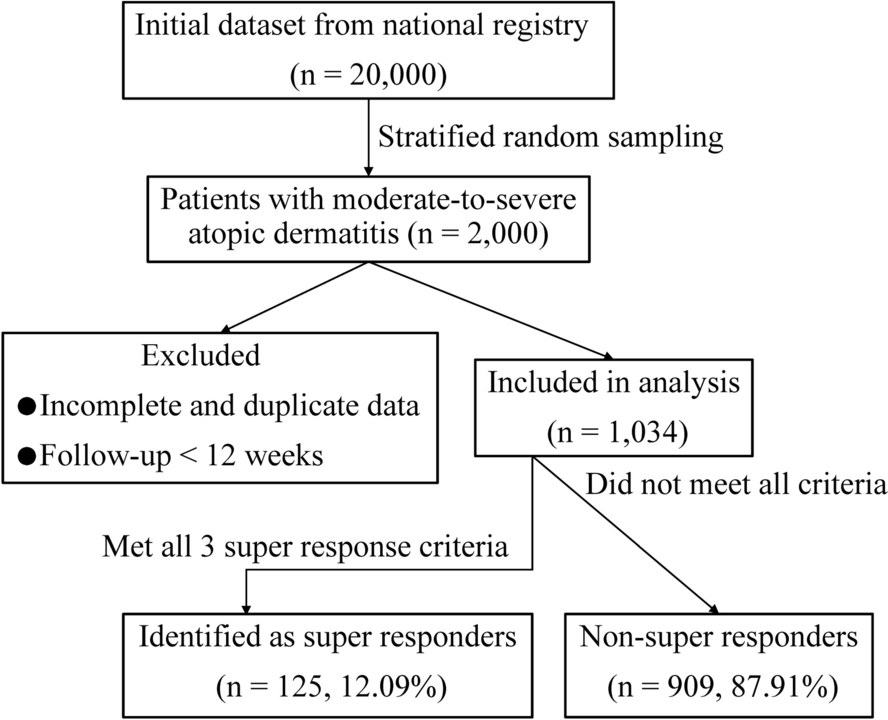
Currently, there is no universally accepted definition of SRs in AD clinical research. We propose that SRs should be identified through a comprehensive evaluation that incorporates not only objective improvement in skin lesions but also subjective relief of pruritus and significant enhancement in quality of life. Drawing on the previous study [11], we adopted a relatively stringent definition of SRs in this study: requiring the simultaneous achievement of EASI-75, a ≥ 4-point reduction in pruritus, and a ≥ 4-point improvement in DLQI.
In univariate analysis, we first found that SRs had a higher average age, with a similar gender distribution. Furthermore, patients with an age of onset after 12 years were more likely to achieve SR status. This phenomenon may reflect differences in type 2 inflammation activity or immune dysregulation across different age groups. Type 2 inflammation is generally more pronounced in childhood and adolescence, consistent with earlier AD onset [15,16]. In contrast, immune senescence in middle-aged and elderly patients may lead to reduced type 2 inflammation [17,18], resulting in a chronic low-grade inflammatory state that responds more readily to IL-4/IL-13 pathway inhibition [19]. Notably, immune status is not solely age-dependent but also influenced by genetics, environmental exposures, and lifestyle factors [20]. Although multiple clinical studies have confirmed that dupilumab provides significant clinical benefits across all age groups compared with conventional therapies [21,22,23], we advocate for future research to further refine the understanding of biologic efficacy and predictive factors in age- and onset-specific subgroups of patients with AD.
Similarly, in terms of immune status, we observed that patients with AD without prior biologic treatment had a higher proportion of SRs compared with those who had received biologics before. In mainland China, only a single biologic targeting one immune pathway is currently approved for AD treatment [24]. This suggests that patients with prior biologic exposure were likely treated with other biologics—either aimed at different immune pathways for comorbid immune conditions or due to an inadequate response or relapse after initial dupilumab therapy. Regardless of the reason, this subgroup likely presents with more complex immune dysregulation or has experienced immune drift, shifting from other types of immune imbalances to a type 2 inflammation-dominated AD phenotype. Consequently, these patients may be less likely to achieve SR status with dupilumab. Interestingly, peripheral blood eosinophil count did not significantly impact the proportion of SRs, suggesting that systemic markers may not reliably reflect local immune activity in skin lesions. Moreover, only 22.24% (230/1,034) of patients with AD in our study exhibited elevated eosinophil levels, lending partial support to this hypothesis.
In addition, baseline disease severity—reflected by the intensity of pruritus, the extent of eczematous lesions, and the degree of quality-of-life impairment—was positively correlated with SR. It is worth noting that, while the PP-NRS scale includes a category for severe pruritus, only mild and moderate levels were present in our dataset. As such, the observed association with moderate pruritus reflects the highest available level of baseline pruritus severity in this cohort. We speculate that the “itch-scratch” vicious cycle in AD leads to persistent skin barrier damage, creating a refractory state that perpetuates recurrent eczema flares. This cycle often results in secondary infections, poor sleep quality, and social dysfunction, further exacerbating the patient’s quality of life [25]. Existing studies have demonstrated that biologic therapy can rapidly alleviate pruritus [22,24], and this relief can break the itch-scratch-lesion-psychological distress loop. As a result, patients with more severe baseline disease may experience more pronounced positive feedback upon symptom improvement, which could enhance their adherence and motivation for continued treatment. Similarly, patients with AD with a history of systemic therapy likely have a better understanding of their disease and greater acceptance of biologic treatments. This treatment experience may contribute to better therapeutic outcomes, partially compensating for the more severe immune dysregulation typically seen in this group.
During AD treatment, higher doses of dupilumab and relatively shorter dosing intervals were associated with increased drug concentrations in the bloodstream, suggesting that optimizing the balance between treatment costs and clinical benefits is crucial for maximizing the cost-effectiveness of biologic therapy. However, this study is subject to several unmeasured confounding factors. First, confounding by indication may have occurred, as patients with more severe symptoms could have been more likely to receive higher dupilumab doses or shorter injection intervals, which may exaggerate the apparent association between dose intensity and treatment response. Second, treatment adherence could not be uniformly verified, and nonadherence among certain subgroups may have influenced the clinical outcomes. Third, physician discretion in dose adjustment may vary by clinical judgment or institutional protocols, contributing to prescribing bias. These factors limit the ability to draw definitive conclusions regarding the causal relationship between dose/frequency and SR. Future prospective studies with standardized treatment algorithms, electronic adherence tracking, and clinician decision audit tools are warranted to reduce these confounding effects and validate our findings.
Notably, once biologic therapy has been initiated, combining other medications or systemic immunosuppressive treatments did not increase the proportion of SRs. This finding reinforces the superiority of dupilumab monotherapy in treating AD while also underscoring the need for future studies to explore effective combination strategies that could further enhance biologic responses. Without such approaches, biologic treatment failure may complicate subsequent adjustments to personalized management plans for patients with AD [26,27]. Furthermore, commonly investigated factors traditionally considered as potential contributors to AD severity—such as high BMI, metabolic diseases (e.g., diabetes), a history of atopic diseases, psychological comorbidities (e.g., depression or anxiety), and family history—showed no significant association with SR status in the multivariate model, likely owing to shared variance with stronger predictors such as PP-NRS or DLQI. However, multicollinearity was formally assessed using both correlation matrices and VIF analysis, ensuring the robustness of the model. Nonetheless, the proportion of SRs in these groups was comparable to that of other statistically significant factors. This suggests that biologic therapy should still be actively considered for patients with moderate-to-severe AD, regardless of underlying physical conditions, comorbidities, or genetic predispositions.
Indeed, this study has several limitations. First, it is a retrospective analysis of prospectively collected registry data, which enabled the inclusion of a large, diverse real-world patient population reflective of routine clinical practice and ensured consistent time-sequencing between baseline predictors and treatment response. However, to ensure reliability of data analysis, we excluded patients with AD with incomplete follow-up (less than 12 weeks) or missing key variables, which may have introduced selection bias, potentially favoring patients with better adherence or more systematic care. Second, although the dataset was derived from a national, multicenter clinical research platform in China, external validation of our predictive findings was not conducted in a separate independent cohort. Therefore, the generalizability of baseline PP-NRS and DLQI as predictors of SR requires further confirmation. Future prospective, multicenter studies incorporating independent validation cohorts and biomarker data are warranted to strengthen clinical applicability and predictive accuracy. Finally, owing to limitations of the registry data, we were unable to analyze AD phenotypes (e.g., intrinsic versus extrinsic). As phenotypic differences may influence both treatment response and DLQI outcomes during dupilumab therapy, future studies should incorporate standardized phenotype classification28.
Taken together, these findings highlight the characteristics of SRs to anti-IL-4Rα biologic therapy. This predictive insight can facilitate a more collaborative approach in developing personalized treatment plans, help manage patient expectations regarding prognosis, improve treatment adherence, and guide timely adjustments to therapeutic regimens to achieve optimal outcomes.





Comments (0)