Our systematic review and meta-analysis aimed to comprehensively evaluate the association between vitiligo and the risk of malignancies, including melanoma, NMSC, and lymphoma. While previous studies have largely focused on the connection between vitiligo and skin cancers, such as melanoma and NMSC [12, 31], our study is the first to simultaneously investigate the incidence of lymphoma, a non-skin-related malignancy, alongside skin malignancies. By employing rigorous statistical analyses, we address a critical gap in the existing literature.
Melanoma Risk
Our analysis found no statistically significant association between vitiligo and the risk of melanoma, although trends toward a reduced risk were observed. The pooled hazard ratio (HR 0.80; 95% CI 0.27–2.34) highlights the necessity of cautious interpretation because of substantial heterogeneity (I2 = 80%). Immune-mediated destruction of melanocytes, a hallmark of vitiligo, may explain these observed trends. Enhanced immune surveillance, particularly through heightened T cell activity, is proposed as a protective mechanism that targets aberrant melanocytes, thereby reducing the likelihood of malignant transformation [32, 33]. This hypothesis aligns with prior studies, such as those by Teulings et al., who reported a threefold reduction in melanoma incidence among patients with vitiligo [25] and Lindelöf et al., who documented minimal melanoma incidence in vitiligo populations over long-term follow-up periods [28].
However, these results must be interpreted in the context of broader epidemiological trends. For instance, declining melanoma incidence in regions like Sweden and Hungary may reflect improvements in preventive measures and early detection efforts, which could confound the observed associations [34, 35].
Non-melanoma Skin Cancer Risk
For NMSC, the pooled HR of 0.38 (95% CI 0.00–732.76) suggests a potential reduction in risk, but the wide confidence intervals limit definitive conclusions. It is noteworthy that both studies included in the NMSC meta-analysis were based on Asian populations [10, 27]. Prior studies, such as those by Schallreuter et al. [29] and Paradisi et al. [24], have reported reduced photodamage and lower NMSC incidence in patients with vitiligo despite comparable UV exposure. This paradox may be explained by the protective effects of immune hyperactivity, which targets atypical keratinocytes in addition to melanocytes [36]. However, conflicting evidence exists, as Hexsel et al. [9] reported statistically non-significant elevated NMSC rates in patients with vitiligo.
Lymphoma Risk
Unlike autoimmune diseases such as rheumatoid arthritis, Sjögren’s syndrome, and celiac disease—which exhibit increased lymphoma risk due to chronic B cell and T cell activation [37,38,39,40]—our analysis found no significant association between vitiligo and lymphoma risk. Nevertheless, these findings must be interpreted with caution, as statistical insignificance may be influenced by the limited number of studies included in the analysis.
It is plausible that vitiligo operates through distinct immune pathways compared to other autoimmune disorders. However, isolated studies, such as Hadi et al. [30], have reported a 3.33-fold increased risk of lymphoma in patients with vitiligo, underscoring the potential heterogeneity in outcomes that warrants further exploration; therefore, further studies reporting lymphoma risk in such populations are required.
Proposed Mechanisms Linking Vitiligo to Reduced Cancer Risk
Several hypotheses have been proposed to explain a potentially reduced risk of skin cancer in vitiligo. A key mechanism involves enhanced immune surveillance, particularly elevated levels of circulating natural killer (NK) cells in patients with vitiligo [31, 41]. NK cells play a critical role in defending against cutaneous squamous cell carcinoma, and their increased presence in both lesional and non-lesional skin may contribute to antitumour activity [31].
In melanoma, genome-wide association studies have identified protective polymorphisms in the TYR gene, which encodes tyrosinase, an essential enzyme in melanin synthesis [42]. These variants may reduce tyrosinase activity or alter melanocyte behaviour, decreasing the likelihood of malignant transformation [11, 42]. Tyrosinase, along with other melanogenic proteins such as gp100 and MART-1, are key antigens targeted by cytotoxic CD8+ T cells, which are central to tumour surveillance and control [43]. In vitiligo, autoreactive CD8+ T cells specific to melanocyte antigens are both necessary and sufficient for melanocyte destruction, with their numbers correlating with disease activity [44]. A similar response occurs in melanoma, where CD8+ T cells recognise shared antigens, contributing to autoimmune manifestations such as melanoma-associated leukoderma or halo phenomena [43]. This shared immune pathway suggests that melanocyte-targeted autoimmunity in vitiligo may also promote anti-melanoma immunity and tumour regression [43]. Supporting this, prior research demonstrated that melanocytic antigens, including both UV-induced neoantigens and differentiation antigens expressed by healthy melanocytes, can enhance responses to immune checkpoint blockade [45]. Notably, mice that had previously cleared melanoma showed improved immune control of pancreatic cancer cells expressing melanocytic antigens, whereas this effect was absent in pancreatic tumours with no melanocytic antigen expression [45]. These findings highlight a potential cross-protective role of melanocyte-specific immune memory, warranting further research into how vitiligo-associated immune mechanisms could inform cancer immunotherapy.
Furthermore, behavioural factors may contribute to the reported lower incidence of melanoma in patients with vitiligo. Sunlight exposure, known to exacerbate vitiligo lesions, often leads to increased sensitivity and avoidance of UV radiation by patients with vitiligo [46]. This behaviour, while protective against further depigmentation, may also reduce UV-induced DNA damage, a key factor in melanoma development [47].
Risk of Non-Skin Malignancies
Interestingly, some studies have reported an increased risk of certain non-skin-related cancers in patients with vitiligo compared to healthy controls. A comprehensive nationwide study in Taiwan by Li et al. [48] revealed that the overall incidence of malignancies in individuals with vitiligo was 0.71 per 100 person-years, notably exceeding the 0.28 per 100 person-years observed in the general population. The study also found that the standardised incidence ratio for post-vitiligo malignancies was significantly elevated, with no discernible gender disparity. Furthermore, sex-specific analyses revealed that male patients were more likely to develop prostate cancer, while female patients exhibited a significantly higher propensity for thyroid and breast cancers, as reported in other studies [49, 50]. These findings suggest that the correlation between vitiligo and malignancy remains elusive, potentially because of the different pathomechanisms underlying various cancers and their unique relationship to vitiligo.
One plausible explanation for these observations lies in the role of CD8+cytotoxic T lymphocytes (CTLs), a specialised subset of immune cells, which play a pivotal role in the pathogenesis of vitiligo by targeting and destroying melanocytes, resulting in the characteristic depigmentation [48, 51]. Beyond their role in autoimmunity, these CTLs are also integral to the immune system’s defence against tumours, orchestrating the recognition and elimination of malignant cells [48, 52, 53]. However, aberrant activation of CD8+ CTLs can lead to their infiltration into tumour sites, potentially compromising the integrity of the tumour capsule and influencing tumour progression and metastasis [48, 52]. In the case of thyroid cancer, this aberrant CTL activation may contribute to the increased risk of thyroid malignancies in patients with vitiligo, although further research is needed to clarify the exact mechanisms involved [48]. Similarly, while vitiligo has been associated with breast cancer, the relationship remains poorly understood and is primarily based on isolated case studies [49, 48]. Furthermore, in prostate cancer, studies indicated that both ultraviolet exposure and vitamin D levels could influence prostate cancer risk [54].
Strengths and Limitations
Our study possesses strengths and limitations. We rigorously adhered to the Cochrane Collaboration guidelines to ensure the highest standards of quality, transparency, and replicability in our methodology and findings. Notably, to the best of our knowledge, this is the first meta-analysis to include non-skin cancers, specifically lymphoma, in the context of vitiligo, which represents a novel contribution to the existing literature.
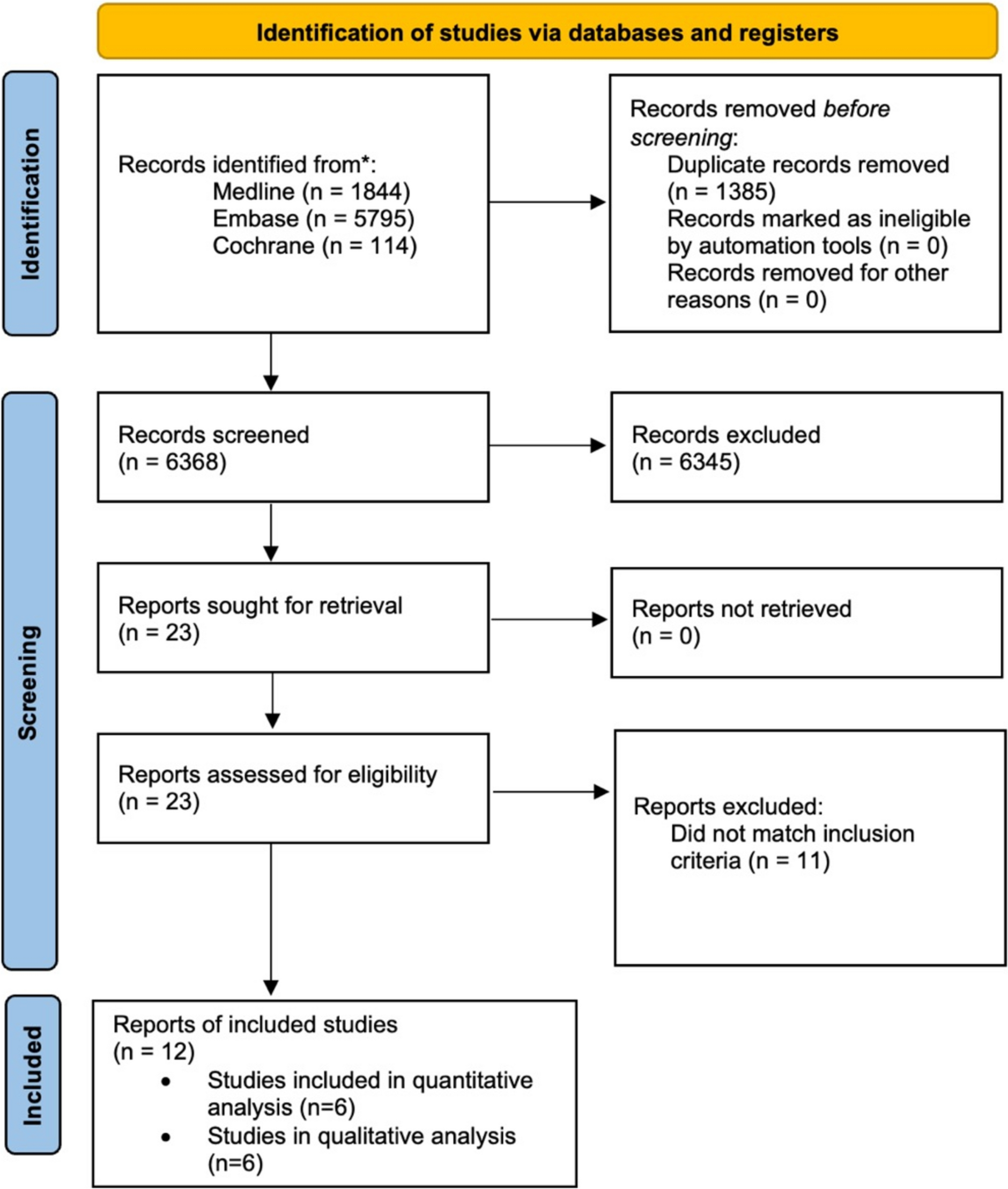
Nevertheless, several limitations must be considered. There was substantial heterogeneity across the included studies, particularly in the melanoma subgroup, where the I2 statistic reached 80%, indicating significant variability in the data. Additionally, only 6 out of 12 eligible studies could be included in the quantitative synthesis because of the absence of hazard ratio reporting, which limits the comprehensiveness of the meta-analysis. The small number of included studies, combined with the wide confidence intervals observed in several pooled estimates, undermines statistical power and reduces the precision and reliability of the findings. As a result, the ability to draw definitive conclusions is limited. Furthermore, key confounding factors such as exposure to phototherapy, behavioural tendencies toward sun avoidance, and regional variations in melanoma incidence were not consistently accounted for across studies, potentially influencing the robustness of our conclusions. Finally, for rare malignancies such as CTCL, the low number of events limits the ability to detect meaningful differences in incidence, and results should therefore be interpreted with caution in these contexts.
Implications for Practice and Research
The integration of scientific advancements into clinical practice is fundamental to enhancing patient care [55, 56]. Interestingly, patients with vitiligo do not appear to have a higher risk of skin cancers, despite the absence of melanocyte-mediated UV protection.
Our findings show that patients with vitiligo may exhibit a non-significant trend of reduced risk of melanoma and NMSC, potentially as a result of enhanced immune surveillance and melanocyte depletion. Clinicians should recognise these protective trends; however, they should also consider the heterogeneity of outcomes across studies and possible population differences. Although sun avoidance behaviours in patients with vitiligo may further reduce cumulative UV exposure, healthcare providers should continue to emphasise routine skin examinations, especially for patients undergoing treatments that may influence immune pathways, such as phototherapy or systemic immunosuppressants.
While our analysis did not identify an increased lymphoma risk in patients with vitiligo, clinicians should remain cautious, as evidence remains limited, and isolated studies have suggested variable outcomes. This underscores the need for tailored surveillance strategies and patient counselling, particularly for individuals with additional risk factors or long-standing immune dysregulation.
Future research must focus on addressing the current gaps and limitations in the literature. Large, multicentre cohort studies with robust methodologies are needed to further clarify the relationship between vitiligo and malignancies. Standardised reporting of outcomes, including hazard ratios, will be essential for improving comparability across studies. Additionally, prospective studies should evaluate the long-term impact of phototherapy and immunomodulatory treatments on cancer risk in patients with vitiligo. Research exploring non-skin-related malignancies, such as prostate, thyroid, and breast cancers, is warranted to better understand their association with vitiligo and identify potential underlying immunological or genetic mechanisms. Clinicians should always recommend regular follow-up. Given that patients with vitiligo often avoid sun exposure, it is important for clinicians to reinforce the need for adequate sun protection while also safely recommending UV-based therapies when appropriate. By addressing these knowledge gaps, future studies can guide evidence-based surveillance strategies, optimise clinical management, and enhance our understanding of vitiligo’s broader implications for cancer risk.





Comments (0)